
Abstract
A 72-year-old patient presented with malaena secondary to two antral ulcers which were discovered in oesophagogastroduodenoscopy (OGD) after admission. One of the ulcers with a visible vessel was injected with adrenaline and clipped with an OVESCO clip. The patient continued to have coffee ground vomitus on the following day with a drop in haemoglobin level. Repeat OGD showed a large intra-mural haematoma with the clip still in situ and no bleeding from the surface of the ulcer. Patient underwent a coil embolization of the distal gastroduodenal artery (GDA), right gastroepiploic artery and a medial branch of the GDA. Repeat OGD showed that the submucosal haematoma had evacuated, leaving a large, clean-based mucosal defect.
Introduction
Bleeding from the upper gastrointestinal tract (UBGIT) is a common cause for admission into the general surgical ward of an acute hospital. There can be 80–150 such incidences every year in a population of 100,000. 1 Medications such as antiplatelets and anticoagulants can increase the likelihood of such bleeds. The clinical presentation can vary between haematemesis, coffee ground vomitus, malaena, black stool and abdominal pain. Most of these patients will need adequate resuscitation and antacids prior to endoscopic evaluation and therapeutics. Therapeutic options to stop the bleeding include thermal coagulation to achieve haemostasis, epinephrine injection to stimulate vasoconstriction of the bleeding blood vessel or using clips. 1 This case report looks at one patient who underwent endoscopy and received the therapeutics suggested above but suffered an unusual complication.
Patient information and diagnostic assessment
A 72-year-old male with no past medical history was admitted after two episodes of melaena. He did not take any regular medication. His haemoglobin level on admission was 9.5 g/dl. He was started on intravenous esomeprazole infusion and underwent an oesophagogastroduodenoscopy (OGD) which showed two antral ulcers; one had a clean base and another one had a visible vessel and a clot at the base of the ulcer [Figure 1(a)].

Antral ulcer before (a) and after (b) endoscopic clipping.
Therapeutic intervention
Biopsies from the edge of the clean-based ulcer were taken. The ulcer with an adherent clot was injected with 2 ml of 1 in 10,000 adrenaline and an OVESCO OSTC clip was placed over the ulcer to secure haemostasis [Figure 1(b)]. The ulcer was pulled inside the applicator cap using endoscopic suction and the clip was applied around the captured ulcer by turning the handwheel. The OVESCO clip used was OVESCO type 11/6 t. It has a cap size of 11 mm and an applicator cap depth of 6 mm. It also has teeth with small spikes for compression and anchoring effect. It delivers constant force at the application site, securing the haemostatic effect.
The patient however continued to have six further episodes of coffee-ground vomitus the day after the scope and his haemoglobin level dropped further from 9.5 to 7.9 g/dl. He received blood transfusion and continued to be kept nil by mouth. A repeat OGD was done and the endoscopic findings were as shown in Figure 2(a). He also underwent a computed tomography (CT) mesenteric angiogram [Figure 2(b)].
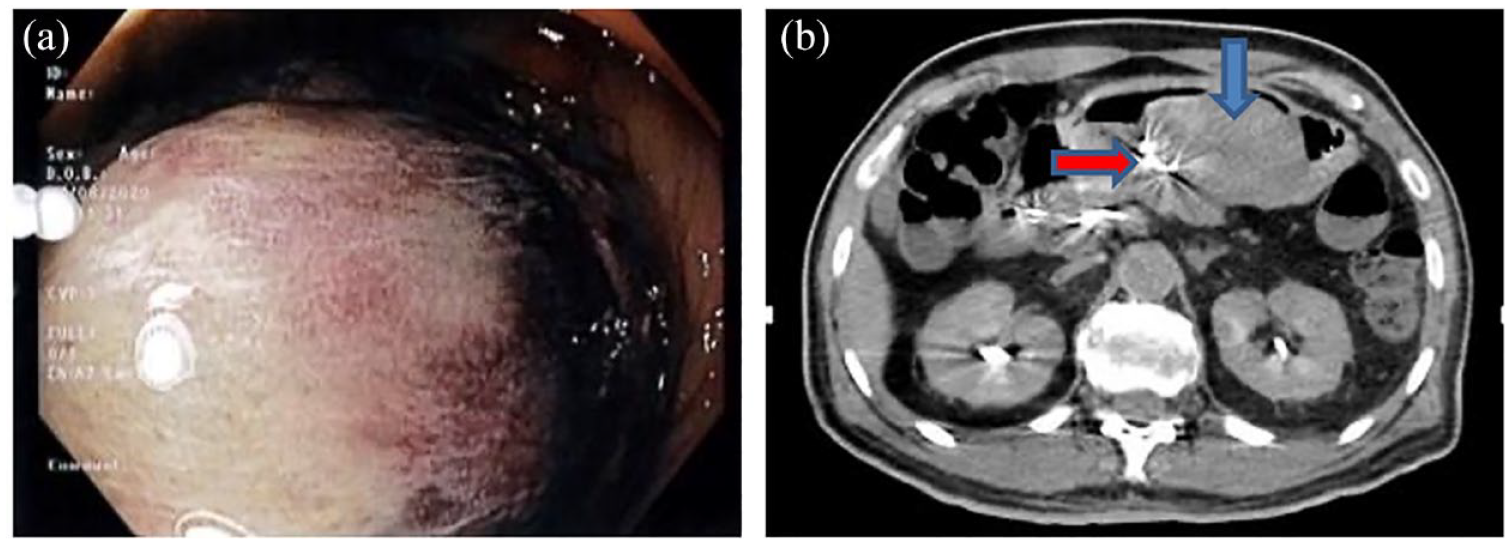
Intramural haematoma viewed on endoscopy (a) and on CT imaging (b).
The repeat OGD showed a large intramural haematoma in the gastric body and antrum. The previously placed OVESCO OSTC clip was still in situ, and the clipped ulcer was not bleeding from the surface of the gastric mucosa. The CT mesenteric angiogram showed no active bleeding point or vessel. In Figure 2(b), the blue arrow points to the haematoma and the red arrow points to the OVESCO clip.
Follow-up and outcome
A decision was made to prophylactically embolize the gastroduodenal artery (GDA) and the branches supplying the gastric antrum as a precautionary measure. The patient underwent prophylactic coil embolization of the distal GDA, right gastroepiploic artery and medial branch of GDA leading towards the OVECSO clip [Figure 3(a)]. Post procedure, patient was well and had no further vomiting. Another OGD 3 days later showed the clip still in situ but the previous haematoma had evacuated leaving a large clean-based mucosal defect [Figure 3(b)]. The histology from the other clean-based ulcer which was not clipped showed chronic gastritis.

(a) Coil embolisation and (b) Mucosal defect after resolution of haematoma.
Discussion
Gastric intramural haematoma is a complication that can occur after endoscopic therapy for peptic ulcers.2,3 Contributing factors include underlying coagulopathy, blood dyscrasias or endoscopic therapy.2,3 Management of this complication depends on the underlying cause and the clinical suspicion of ongoing bleeding. Management options include conservative management, endoscopic intervention, surgery and transarterial catheter embolization.2 –4
With clipping of an ulcer or an exposed vessel, there is a risk that the clip may be distal to the actual point of bleeding. Another possibility in this case is that the clip may not have covered the complete diameter of the blood vessel. Given the mechanism of the OVESCO clips, the chance of failure may also increase if the site of bleeding is not clearly visualized by the endoscopist or if attempted by someone less experienced. Hence, patients who undergo therapeutic endoscopy for UBGIT should be monitored closely in the ward or in high dependency care. Haemoglobin level should be checked the following day to ensure that the bleeding has stopped and not recurred. A raised heart rate or a drop in blood pressure are indications to repeat a full blood count earlier.
One strength of this report is that we have accurate images of the initial insult discovered via OGD and the subsequent submucosal haematoma seen in both OGD and the CT. We also have identified the exact clip which was used. A limitation is that the above information is still insufficient to draw conclusions about how to prevent such a complication in future. 5
Supplemental Material
sj-docx-1-cmg-10.1177_26317745231220477 – Supplemental material for An unusual complication after endoscopic clipping of a gastric ulcer
Supplemental material, sj-docx-1-cmg-10.1177_26317745231220477 for An unusual complication after endoscopic clipping of a gastric ulcer by Lakshman Ramu, Soo Kian-Tak and Gerald Ci-An Tay in Therapeutic Advances in Gastrointestinal Endoscopy
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.