
Abstract
Endoscopic therapy of early Barrett’s oesophagus–related neoplasia is the treatment of choice for low-grade-dysplasia, high-grade dysplasia and mucosal Barrett’s cancer. Low-grade-dysplasia without any visible lesion should be ablated, preferably with radiofrequency ablation. In cases with the presence of a visible lesion, high-grade dysplasia and early Barrett’s adenocarcinoma, endoscopic resection techniques like multiband ligation endoscopic resection or endoscopic submucosal dissection should be applied. After complete resection of all visible neoplastic lesions, ablation of the remaining Barrett’s oesophagus should be performed to prevent recurrence. Ablation techniques available are radiofrequency ablation, argon plasma coagulation and cryoablation.
Indication for endoscopic therapy
Today, endoscopic therapy is the treatment of choice for early Barrett’s oesophagus–related neoplasia (BORN). Endoscopic therapy should be preferred over surgical treatment because it is associated with a lower morbidity and mortality rate and has similar long-term survival rates. The success of every endoscopic eradication therapy depends on the right patient selection for the respective treatment modality and the experience of the endoscopist.
Nondysplastic Barrett’s oesophagus (BO) has a very low risk of progression to high-grade dysplasia (HGD) or cancer, and therefore, endoscopic treatment is not advised. Recent studies have shown that 0.2–0.5% of patients per year will develop HGD or cancer only. Any ablative therapy is associated with costs and potential complications and therefore should not be performed outside controlled studies.
Indications for endoscopic therapy are low-grade dysplasia (LGD), HGD, and mucosal and ‘low-risk’ submucosal Barrett’s adenocarcinoma.
LGD
LGD is a major risk factor for malignant progression of BO.1,2 Because there is uncertainty among pathologists regarding the histopathological diagnosis of LGD, histological expert review is advised.2,3
Several studies have demonstrated that there is very often overdiagnosis of LGD through histopathology by pathologists whose focus is not on BO. Duits and colleagues 4 analysed 293 patients with an initial diagnosis of LGD made by community-based pathologists. Review by a panel of expert pathologists found the initial diagnosis of LGD could be confirmed in 27% only. The diagnosis of the residual patients was downstaged to indefinite for dysplasia in 14% and nondysplastic BO in 59%. During follow-up, for patients with an expert diagnosis of LGD, the incidence rate for progression to HGD or adenocarcinoma was 9.1% per patient-year compared with 0.6% per patient-year for those patients who were downstaged. In a subsequent study by the same group, confirmation of the LGD diagnosis by three expert pathologists and LGD diagnosis at baseline endoscopy with confirmation of LGD at a subsequent endoscopy were associated with highly increased progression rates [odds ratio (OR), 47.14; 95% confidence interval (CI), 13.10–169.70 and OR, 9.28; 95% CI, 4.39–19.64, respectively]. 2
Therefore, confirmation of LDG by an expert pathologist should always be obtained prior to further treatment.
In a randomized clinical trial published by the Amsterdam group, radiofrequency ablation (RFA) and endoscopic surveillance were compared in 136 consecutive patients with LGD in BO. 5 Progression to HGD or adenocarcinoma over a follow-up period of 3 years was the primary outcome parameter in this study. Patients were randomized to receive either RFA or proton-pump inhibitors (PPIs) with endoscopic follow-up. Patients who received ablation had a risk reduction of progression to HGD by 25% and to adenocarcinoma by 7.4%. LGD was successfully eradicated by RFA in 92.6% compared with 27.9% in the control group. In another study, patients with a baseline diagnosis of LGD and a confirmation of LGD in a follow-up endoscopy had a significantly increased progression risk (OR, 9.25; 95% CI, 4.39–19.64).
The high progression rate of confirmed LGD is the reason why ablation is usually recommended. Alternatively, follow-up endoscopies every 6 months are a valid alternative. Prior to every ablative therapy, the Barrett’s segment has to be inspected carefully for visible abnormalities. Every visible lesion should be resected by endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD) to obtain a histopathological diagnosis of the lesion to avoid undertreatment by ablation. LGD on biopsy in combination with a visible lesion very often indicates more advanced BORN.
HGD and early Barrett’s adenocarcinoma
Endoscopic resection
Endoscopic resection (ER) of lesions with HGD or mucosal Barrett’s cancer should always be the first step in endoscopic therapy of BORN. ER of all visible lesions should be followed by ablative therapy of the remaining nondysplastic BO.3,6–8 When HGD or cancer is detected during random biopsies, all advanced imaging techniques should be applied to localize the neoplastic lesion.
Advanced imaging techniques that have shown to be effective in detection are virtual chromoendoscopy, narrow-band imaging (NBI), blue laser imaging (BLI), and i-scan. In combination with optical magnification, even subtle neoplastic lesions can usually be localized. Another very simple and cheap advanced imaging technique is the use of acetic acid in a concentration of 1.5–2.5%. Acetic acid is sprayed over the entire Barrett’s segment. After a few seconds, the Barrett’s epithelium turns to a whitish colour (aceto-whitening effect). After another 30–40 s with HGD and Barrett’s cancer, there is a loss of aceto-whitening and neoplastic lesions turn red. Therefore, acetic acid staining is the ideal red flag technique with a sensitivity of 92% and a specificity of 96%. 9
In our daily practice, we perform a thorough inspection of the entire Barrett’s segment with high-definition white-light imaging, usually with a transparent distal attachment cap at the tip of the endoscope. Afterwards, we switch to NBI or BLI to make a second thorough inspection of the entire Barrett’s mucosa. At the end, we spray 1.5% acetic acid solution over the BO. We perform targeted biopsies of all suspicious lesions and four-quadrant biopsies of the remaining Barrett’s mucosa. Prior to any endoscopic treatment, a thorough inspection of the BO is very important to detect even subtle neoplastic lesions and to identify their borders prior to ER.
If a lesion cannot be localized, referral to an expert centre should be considered. ER can be performed with a multiband ligation device and a dedicated 5-Fr snare that can be advanced through the working channel with the mounted ligation device. ER is an advanced endoscopic procedure requiring extensive training in experienced high-volume centres. The reported perforation rate of six trainees during their first 120 ERs (20 ER/trainee) in anesthetized pigs was 5%. 1 Another series from the United Kingdom demonstrated that upper gastrointestinal (GI) EMR was associated with a significantly higher mortality and perforation rate when performed by a less experienced endoscopist. 10 Therefore, the European Society of Gastrointestinal Endoscopy (ESGE) guidelines recommend that Barrett’s neoplasia should only be treated in expert centres defined as a minimum of 10 new cases with early neoplasia per year, access to experienced oesophageal surgery and prospective data collection of all Barrett’s cases. 3
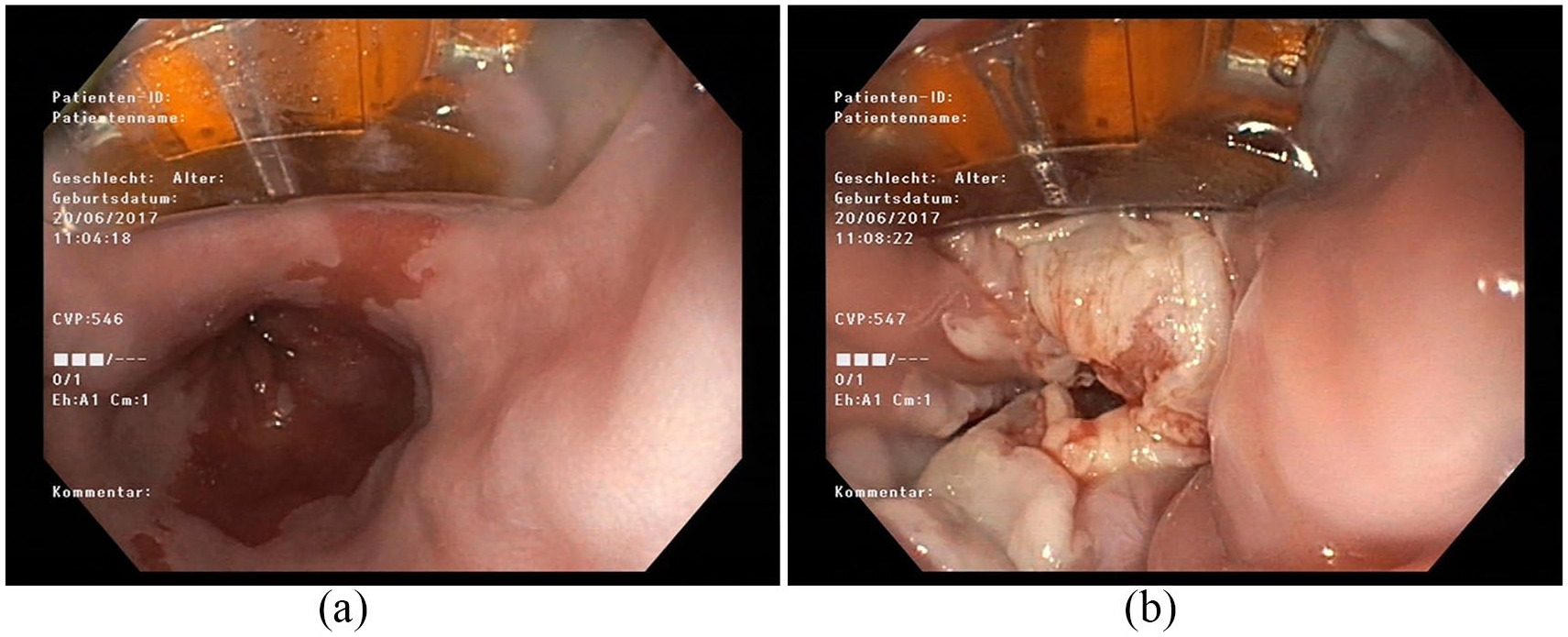
The largest series on ER in 1000 patients with mucosal Barrett’s adenocarcinoma demonstrated excellent long-term complete remission rates of neoplasia in 93.8% after a follow-up of almost 5 years with a very low complication rate of 1.5%. 8 A problem of endoscopic treatment is the relevant rate of neoplastic recurrences, 14.5% in this series. As all patients were in a follow-up programme, recurrences were diagnosed at an early stage, making endoscopic retreatment feasible in almost all cases (Figure 1).

ER of an early Barrett’s adenocarcinoma with the multiband ligation device (MBM ER): (a)–(d) multiband ligation ER of an early Barrett’s adenocarcinoma.
ESD
ESD has been established as an important treatment method for T1 Barrett’s adenocarcinoma, also in Western centres. With ESD, early neoplastic lesions can be resected en bloc independent of their size. ESD is difficult to learn and requires intensive training until endoscopists are proficient. Several series have been published in recent years, showing that ESD is safe in the hands of experts. The rates of complete resection (R0; tumour-free horizontal and vertical margins) of Barrett’s cancer were reported to be from 38.5% to 79%. The stricture rates are up to 60% due to the larger areas resected with ESD.11–13 A recently published prospective randomized series compared EMR with ESD in 40 patients with mucosal Barrett’s cancer. There was no significant difference regarding the rates of complete remission between both groups. 14
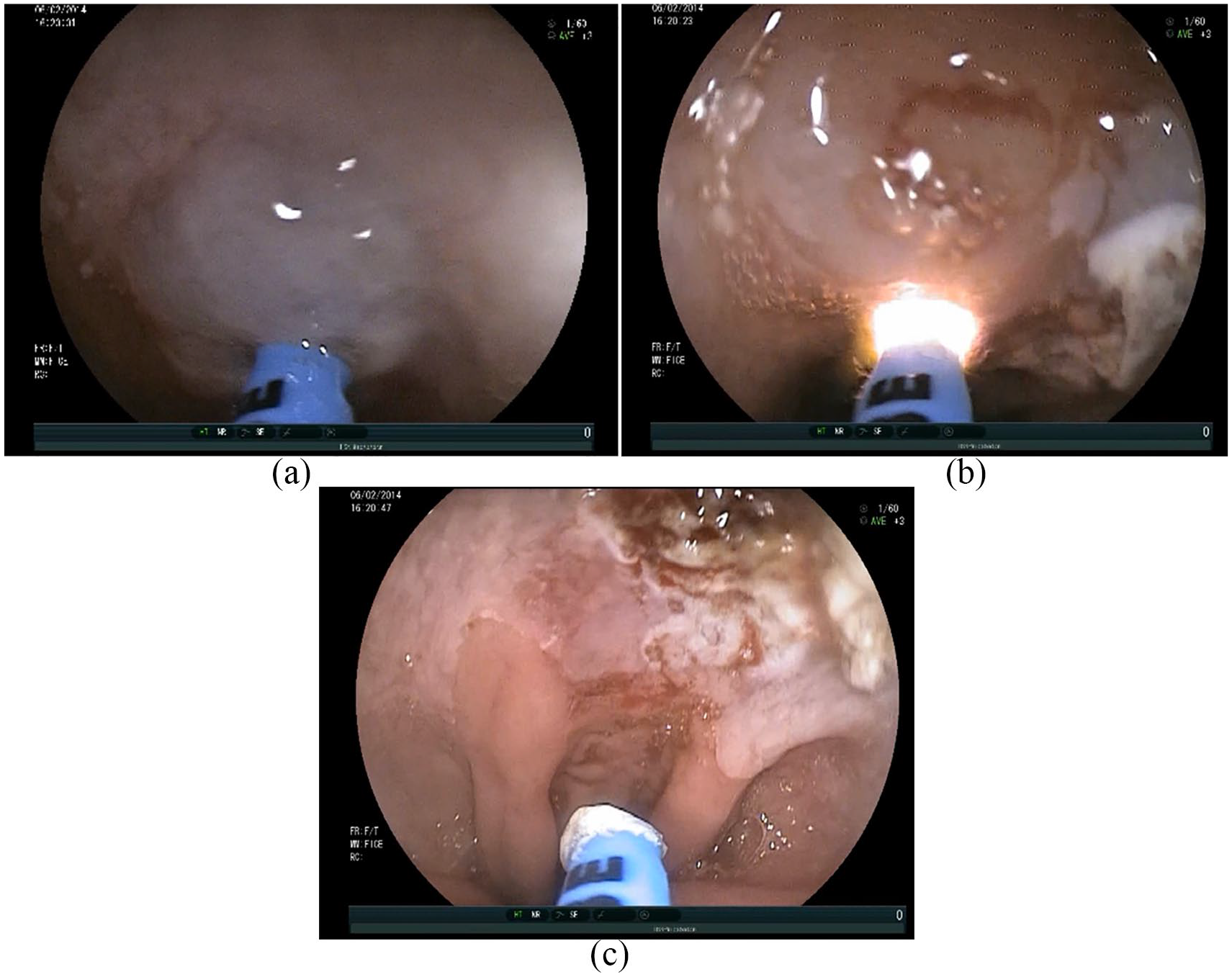
According to most guidelines, ER is still the treatment of choice. 13 ESD should be performed in nodular Barrett’s cancer >15 mm and when there is a suspicion for submucosal infiltration. In those cases, an en bloc resection allows a more exact histopathological evaluation regarding the complete resection status and the lymphatic and vascular infiltration status (Figure 2).

ESD of early Barrett’s adenocarcinoma type IIb + c: (a)–(d) ESD of early Barrett’s adenocarcinoma.
Ablation of the residual BO after ER/ESD
Complete ablation of the residual Barrett’s epithelium after ER of the neoplastic lesion can significantly reduce the recurrence rate of neoplasia.10,15 Therefore, ablation of the whole Barrett’s epithelium should be the treatment aim. This can be achieved with different ablation methods like RFA, argon plasma coagulation (APC) and cryoablation.
RFA
RFA of the remaining Barrett’s epithelium is the current treatment standard and has been studied extensively in many high-quality prospective studies. A large prospective multicentre study from Europe (Euro-2 study) evaluated the efficacy and safety of RFA of the residual Barrett’s epithelium after ER of HGD and early Barrett’s adenocarcinoma in 13 experienced European centres. 16 In all, 132 patients with high-grade intraepithelial neoplasia (HGIN) and early Barrett’s adenocarcinoma were prospectively included. Patients were treated according to the ‘two-step concept’: ER followed by ablation. 17 The complete remission rates for neoplasia and intestinal metaplasia were 98% and 93%, respectively. Due to the excellent results of several studies, the recommendation in most current guidelines is that the ‘two-step concept’ is the treatment of choice in patients with HGIN and early Barrett’s adenocarcinoma.3,6,7
Those excellent results could not be confirmed in all studies. In a large meta-analysis of 18 studies with 3802 patients, the complete remission rate of intestinal metaplasia was 78% and of dysplasia was 91%. 18
Another way to remove the remaining Barrett’s epithelium at risk of neoplastic progression is a complete stepwise ER of the neoplastic lesion and afterwards resection of the whole BO. The treatment results were excellent with a high complete remission rate, but this approach had a high stricture rate of more than 50%.
A recent meta-analysis compared the two-step concept consisting of focal ER and RFA with the stepwise radical resection method. 19 Nine studies with 774 patients of focal EMR + RFA and 11 studies with 751 patients of stepwise ER were included. Both groups had a similar complete remission rate, but the complication rate was significantly higher in the stepwise ER group (strictures 33.5% versus 10.2%; bleeding 7.5% versus 1.1%; perforation 1.3% versus 0.2%) (Figure 3).
RFA of residual Barrett’s mucosa: (a) and (b) RFA of residual Barrett’s mucosa.
Cryoablation
Among all Barrett’s ablation techniques, cryoablation is the new ‘kid on the block’. It induces tissue necrosis by freezing the target mucosa. With this method, the extracellular matrix is preserved. A major advantage compared with RFA is that cryoablation seems to be less painful than RFA.20,21 In addition, a recent study indicates that it also has a lower stricture rate. 20
There are two cryoablation systems on the market:
Endoscopic spray cryotherapy either with liquid nitrogen or with rapidly expanding carbon dioxide gas. This is sprayed over the Barrett’s segment, resulting in cell death.
Cryo-balloon ablation, where a balloon is expanded at the level of the Barrett’s segment and then a focal spray ablation is performed.
So far, there are limited data on treatment of early Barrett’s neoplasia. However, complete eradication of dysplasia was observed in 87–96% and complete ablation of Barrett’s mucosa in 57–96% of patients.20–23 Cryotherapy was also effective in patients with early Barrett’s adenocarcinoma with complete remission in 75%, including patients who have failed other endoscopic treatments21,23 (Figure 4).

Cryoablation of residual Barrett’s mucosa: (a) and (b) cryoablation of residual Barrett’s mucosa.
APC
APC is an effective and inexpensive Barrett’s ablation method that has been used for more than 15 years. Remission of BO can be achieved in most cases.15,22–25 Manner and colleagues 16 demonstrated in a recently published prospective randomized trial that ablation of the remaining Barrett’s epithelium with APC after successful treatment of mucosal Barrett’s adenocarcinoma by ER can significantly reduce the rate of recurrences or metachronous neoplasia compared with PPI alone. A novel development is hybrid-APC. With one single catheter, combining a high-pressure water jet with an APC probe, submucosal injection can be performed as the first step. Afterwards, the Barrett’s epithelium can be ablated with the APC probe with a higher energy dose than with conventional APC because of the protective effect of the submucosal fluid cushion. This prevents deep damage to the oesophageal wall and seems to be associated with fewer strictures. 24
APC is operator-dependent, and a large number of sessions are required to achieve complete ablation of Barrett’s epithelium. In addition, there is a relatively high risk of residual islands of metaplasia. APC is less expensive compared with RFA and cryoablation (Figure 5).
APC of residual Barrett’s mucosa: (a) hybrid-APC of residual Barrett’s mucosa.
Which ablation method should be used?
All ablation methods mentioned have proven their efficacy and safety in multiple studies. However, by far the most high-quality studies investigate RFA. Therefore, RFA is recommended as the first-line ablation method by the ESGE, British Society of Gastroenterology (BSG) and American Society for Gastrointestinal Endoscopy (ASGE) guidelines. However, failure of RFA and APC is reported in 10–20%. 18 In those cases, cryoablation seems to be an effective and safe salvage therapy.26–28 A recent meta-analysis included 11 studies with 148 patients with persistent intestinal metaplasia or dysplasia after RFA. Cryotherapy achieved a complete eradication of intestinal metaplasia in 46% and of dysplasia in 76%.
After any ablative therapy or ER of BO, sufficient acid suppression is crucial to enable healing of the defect and to induce re-epithelialisation with neosquamous mucosa. Patients should be on high-dose PPI therapy with a standard dose twice daily (e.g. pantoprazole 2 × 40 mg) for at least 8 weeks. In addition, sucralfate and ranitidine 150–300 mg at night are usually recommended. Insufficient acid control is associated with failure of endoscopic therapy of BO and BORN. However, despite high-dose PPI treatment, about 10% of patients will fail to regenerate with normal squamous epithelium instead of BO. Those patients very often have a large hiatal hernia and a long-segment BO. Laparoscopic fundoplication can be discussed in those patients and are beneficial in some cases (Figure 6).

Suggested treatment algorithm for early Barrett’s neoplasia.
Follow-up after ablation
The follow-up intervals should be planned according to the baseline histology of the individual patient. According to a recently published study from two high-volume expert centres, the follow-up strategy after RFA ablation of LGD should be a surveillance endoscopy at 1 and 3 years after complete removal of BO. 29 In case of HGD or intramucosal adenocarcinoma, surveillance endoscopies should be scheduled at 0.25, 0.5 and 1 year and then annually. There are no prospective studies investigating whether these surveillance recommendations can also be applied to patients who received APC or cryoablation, and recommendations should be according to the national guidelines.
Adverse event of endoscopic therapy of BORN
Endoscopic therapy is safe and has a low complication rate, at least in experienced hands. It has been demonstrated that EMR in the upper GI tract is associated with a substantially higher mortality and perforation rate when performed by less experienced endoscopists. 10 This is the reason why current guidelines recommend that BORN should be treated only in expert centres with at least 10 or more new cases with early neoplasia per year and access to experienced oesophageal surgeons.
The most common complications of EMR are strictures and bleeding.8,19 When following the two-step approach with EMR of all visible lesions followed by RFA of the residual Barrett’s mucosa, the stricture rate is around 10% and the bleeding rate 1%. The risk of the development of strictures increases significantly when more than 50% of the circumference of the oesophagus is resected, especially in case of stepwise complete circumferential resection of the entire Barrett’s mucosa with a stricture rate of more than 30% of patients. There are some studies suggesting the use of systemic or local steroid treatment to prevent strictures, but more prospective data are needed to draw final conclusions. In most cases, strictures occurring after endoscopic therapy of Barrett’s neoplasia are successfully treated with a few sessions of Savary or balloon dilatations.
Significant bleeding is a rare event after EMR and even more rare after ablation.8,19 Peri-procedural bleedings can usually be treated with coagulation of small bleeding vessels with the tip of the snare. After resection of the whole target lesion, clips can be applied to stop bleeding. However, clips should be only used when the target lesion is resected completely, as clips could make consecutive EMR impossible.
The risk of perforation is very low and <1% in most published series.8,19 Perforations can be managed with clip closure or fully covered self-expanding metal stents.
Management of Barrett’s adenocarcinoma invading the submucosal layer
Barrett’s adenocarcinoma infiltrating the submucosa is associated with a significant risk of lymph node metastasis of up to 41%. Pathologists usually divide the submucosal layer in thirds and report the tumour infiltration as T1sm1-3. In addition, they should measure the depth of infiltration into the submucosa from the muscularis mucosa in microns. When the adenocarcinoma is infiltrating the upper third of the submucosal layer (pT1sm1 up to 500 μm), the lymph node risk varies between 0% and 21%. However, when the cancer is invading deeper layers of the submucosa (pT1sm2/3; >500 μm) the risk is between 36% and 54%.30–33
Most current guidelines suggest that Barrett’s cancer limited to the upper third of the submucosa (up to 500 μm) without the presence of further risk factors can be treated endoscopically because the risk of lymph node seeding is less than 2%. Risk factors that have to be considered are lymph vessel infiltration (L status), blood vessel infiltration (V status), poorly differentiated cancer (grade 3) and tumour size <20 mm. Some data are suggesting that endoscopic therapy can safely be performed in so-called ‘low-risk’ submucosal Barrett’s cancer (definition: Tsm1-cancer with invasion up to 500 μm, G1/2, L0, V0; diameter <20 mm).31,33 A recently published series treated 67 patients with ‘low-risk’ submucosal Barrett’s cancer. 33 In this large series, all patients received ER. One patient developed a lymph node metastasis during follow-up with endoscopic ultrasound (EUS) after 9 months. This results in a calculated lymph node risk of 1.5%, which is lower than the usual mortality rate of esophagectomy.
According to the available data, endoscopic treatment of ‘low-risk’ T1sm1 Barrett’s adenocarcinoma can be recommended as an alternative to surgery.