
Abstract
Background and study aims:
The objective of this study was to clarify the effectiveness of treatment selection for biliary-type sphincter of Oddi dysfunction by severe pain frequency and the risk factors for recurrence including the history of functional gastrointestinal disorder.
Patients and methods:
Thirty-six sphincter of Oddi dysfunction patients who were confirmed endoscopic retrograde cholangiopancreatography enrolled in this study. Endoscopic sphincterotomy was performed for type I and manometry-confirmed type II sphincter of Oddi dysfunction patients with severe pain (⩾2 times/year; endoscopic sphincterotomy group). Others were treated medically (non-endoscopic sphincterotomy group).
Results:
The short-term effectiveness rate of endoscopic sphincterotomy was 91%. The final remission rates of the endoscopic sphincterotomy and non-endoscopic sphincterotomy groups were 86% and 100%, respectively. Symptoms relapsed after endoscopic sphincterotomy in 32% of patients. Patients in the endoscopic sphincterotomy and non-endoscopic sphincterotomy groups had or developed functional dyspepsia in 41% and 14%, irritable bowel syndrome in 5% and 14%, and gastroesophageal reflux disorder in 14% and 0%, respectively. History or new onset of functional dyspepsia was related to recurrence on multivariate analysis. The frequency of occurrence of post-endoscopic retrograde cholangiopancreatography pancreatitis and post-endoscopic retrograde cholangiopancreatography cholangitis was high in both groups. Two new occurrences of bile duct stone cases were observed in each group.
Conclusion:
According to the treatment criteria, endoscopic and medical treatment for biliary-type sphincter of Oddi dysfunction has high effectiveness, but recurrences are common. Recurrences may be related to new onset or a history of functional dyspepsia.
Keywords
Introduction
The effectiveness of endoscopic sphincterotomy (EST) for sphincter of Oddi dysfunction (SOD) is thought to differ depending on the Milwaukee classification. 1 Endoscopic treatment has a strong effect in type I, which is regarded as an indication for treatment without manometric findings. 2 In patients with type II and type III, the presence of abnormal manometric findings is also considered an indication for endoscopic treatment due to the strong therapeutic effect. 3 However, for type III, the Evaluating Predictors & Interventions in Sphincter of Oddi Dysfunction (EPISOD) trial 4 showed that there was no benefit from endoscopic retrograde cholangiopancreatography (ERCP) even with follow-up for 5 years. 5 There is a report 6 that demonstrated experimentally the hypersensitivity of the duodenum in post cholecystectomy pain; therefore, it is highly likely that type III includes many cases in which the papilla is not a problem. It is reported that the reproducibility of manometry is not very high, 7 and factors related to the effectiveness of long-term endoscopic treatment are not sufficiently clear. In a previous report, 8 endoscopic retreatment was required in 28.3% of type III cases and 20.4% of type I/II cases, and incomplete treatment and recurrence were unexpectedly high. Furthermore, in cases of manometry-proven type II, the improvement rate was 55%, which was not different from the rate (60%) of preventive EST by experienced endoscopists. 9 Endoscopic effectiveness is surprisingly low despite confirming the diagnosis with manometry. Even in type I patients, 5 of 13 (38%) improved without EST, 3 and greater caution about the indications for EST is needed. 10 In SOD, no criteria have yet been established for it to be managed by conservative treatment without invasive treatment such as EST. In addition, there are few reports of long-term efficacy and complications of SOD in considering treatments such as EST.
However, SOD has aspects of a functional disorder. 11 There are few studies investigating the relationship between SOD and functional gastrointestinal disease (FGID). It has been reported that SOD merges with irritable bowel syndrome (IBS; 33.3% in types I and II). 12 Gastroesophageal reflux disease (GERD), functional dyspepsia (FD), and IBS often coexist and may share a common pathophysiological mechanism such as increased visceral hypersensitivity. 13 The similar mechanism may be related to SOD. There is no report on the relationship of the history of FGID and the clinical course of SOD. In this study, the aim was to investigate the effectiveness of treatment selection for biliary-type SOD by severe pain frequency and to clarify the risk factors for recurrence of SOD by analyzing factors including EST and history of FGID.
Patients and methods
From July 1998 to September 2018, 36 patients’ biliary-type SOD was confirmed by ERCP in our institution. These SOD patients were selected by questionnaire, liver function tests (LFTs), hepatobiliary scintigraphy, abdominal ultrasonography, upper gastrointestinal endoscopy, endoscopic ultrasonography, and magnetic resonance cholangiopancreatography.
Cases of suspected bile duct stones, gallbladder stones and chronic pancreatitis, depressive disorder, previous EST, previous endoscopic balloon dilatation (EPBD), and other medical treatments were excluded. The data registry of these 36 patients was retrospectively reviewed. Manometry was performed for type II SOD as much as possible.
Diagnostic criteria for biliary-type SOD are as follows: (1) biliary pain according to the Rome IV criteria and (2) elevated liver enzymes and/or dilated bile duct (>8 mm by imaging modality). 14 Based on clinical, radiographic, and laboratory data, patients were categorized according to the Rome IV criteria as having the prior type I (papillary stenosis) and prior type II (functional biliary sphincter disorder) SOD; type I has elevated liver enzymes and dilated bile duct. Type II has elevated liver enzymes or dilated bile duct. Cases with type III classified by Rome III criteria 15 were excluded according to the Rome IV criteria. 14
We did not include patients considered to have passed bile duct stones in this study. For the purpose of excluding bile duct stones, intraductal ultrasonography (IDUS) was performed as much as possible. In cases where IDUS could not be performed, we confirmed that there was no stone or bile sludge by abdominal ultrasonography and/or endoscopic ultrasonography.
The criteria for undergoing EST were as follows: EST was performed for type I and manometry-confirmed type II SOD patients with severe pain (⩾2 times/year; EST group). 14 Other cases, those with a low frequency of severe pain (<2 times/year) and type II without meeting the manometry criteria did not undergo EST. Severe pain is the level that patient’s daily activities are affected, or that the patient must attend the emergency department. After other organic disorders including malignancy and choledocholithiasis were excluded by ERCP, medical treatment was indicated (non-EST group). In EST group, we defined EST as effective when the previous pain disappeared. It was defined as recurrence when previous pain occurred without other causes during the course after EST or starting medical treatment. In EST group, the recurrence cases which medical therapy was effective were not included in long-term effective cases. As needed, catechol-O-methyltransferase inhibitors or anticholinergics were administered for abdominal pain as medical treatment.
Post-ERCP pancreatitis (PEP) was defined as new or worsened abdominal pain, hyperamylasemia (3 times or more the upper limit of normal), and requiring treatment with prolonged hospitalization. The severity of PEP was graded as mild, moderate, or severe according to a previous report. 16 Pancreatic stents were placed mainly in cases of difficult cannulation for the purpose of preventing PEP. Nonsteroidal anti-inflammatory drugs (NSAIDs) were not given to prevent PEP. Post-ERCP cholangitis was defined as fever with new or worsened abdominal pain and new or worsened LFTs and requiring treatment with prolonged hospitalization.
FGID was defined as a functional abnormality in patients who complained of abdominal symptoms in whom structural disease was excluded. FD was diagnosed when organic diseases and SOD symptoms (LFTs abnormality and biliary-type pain) had been excluded in patients who complained of upper abdominal symptoms including epigatric pain, early satiety, fullness, and nausea, but not heartburn. 17 GERD was defined as recurrent heartburn and/or regurgitation according to the Montreal definition. 18 IBS was defined as a condition of recurrent abdominal pain associated with defecation or a change in bowel habits. The recurrent abdominal pain had to have two or more of the following characteristics: (1) related to defecation, (2) associated with a change in stool frequency, or (3) associated with a change in stool form. 19
Due to the retrospective nature of this study, the need for informed consent was waived. This study was approved by the Institutional Review Board of our institution (no. S16-030).
Outcomes and measures
Whether the criteria for undergoing EST were appropriate was examined by comparing the two groups (EST group versus non-EST group). The short-term effectiveness rate of EST, symptom recurrence rate, and early/late complications were examined in the EST group. The short-term effectiveness rate was defined as the ratio of cases in which no previous symptoms requiring endoscopic retreatment recurred within 30 days after treatment. The long-term effectiveness rate was defined as the ratio of cases in which no previous symptoms requiring some medical treatment at the end of follow-up observation. The final remission rate was defined as the ratio of cases not requiring intervention such as endoscopic treatment at the end of follow-up observation. This included cases in which abdominal pain was controlled by medical treatment excluding NSAIDs and opioids. The symptom recurrence rate and late complications were also examined in the non-EST group.
In both groups, the rate of concomitant FGID in the past and during the course was also examined. The factors relating to recurrence of symptoms were examined by univariate and multivariate analyses.
Statistical analysis
The chi-square test was used for the analysis of categorical data. Quantitative data were compared using Mann–Whitney’s U-test, median test, or Student’s t-test. Values of p less than 0.05 were regarded as significant. Univariate analysis was used with simple logistic regression for the variables. Variables with p-values less than 0.1 on univariate analysis were all included in the logistic regression analysis for multivariate analysis. Multivariate logistic regression analysis was used to identify the risk factors for symptom recurrence in SOD. Values of p less than 0.05 were regarded as significant. Statistical analysis was performed using StatFlex version 6.0 (Artech Co., Ltd., Osaka, Japan).
Results
Basic characteristic of patients with biliary-type SOD is shown in Table 1. Of the 36 cases, 8 had a history of pancreatitis and there was a possibility of combined pancreatic and biliary SOD, but there were no cases of relapsed symptoms or recurrent pancreatitis. There were no differences in the patient background characteristics between the EST group and the non-EST group. In the non-EST group, there were no cases that required EST later. The short-term effectiveness rate of EST was 91% (20 out of 22) (Table 2). Antidepressants were effective for these two cases in which EST was ineffective. Symptoms relapsed at an average of 6 (1–19) months after EST in 32% (7 out of 22; 2 type I cases and 5 type II cases). Endoscopic retreatment was additionally given to 5 (23%; 5 out of 22) of 7 cases. In the non-EST group, symptoms relapsed at an average of 31 (2–67) months after ERCP in 36% (4 out of 14; 2 type I cases and 2 type II cases). There was a tendency for type II to have more recurrence after EST. However, there was no difference in the recurrence rate depending on the type of SOD in both groups.
Basic characteristics of patients with biliary-type SOD.

CBD, common bile duct; EST, endoscopic sphincterotomy; MPD, main pancreatic duct; SOD, sphincter of Oddi dysfunction.
Clinical outcomes.

EST, endoscopic sphincterotomy; SOD, sphincter of Oddi dysfunction.
Regarding the incidence of FGID, patients developed FD in 41% (9 out of 22), IBS in 5% (1 out of 22), and GERD in 14% (3 out of 22) in the past or during the course in the EST group (Table 3). There were 50% (11 out of 22) cases who had a history or developed FGID. In the non-EST group, patients had or developed FD in 14% (2 out of 14), IBS in 14% (2 out of 14), and GERD in 0%. Overall, 29% (4 out of 14) of cases had or developed either disease. There was no difference in the incidence of FGID between the two groups.
Coincidence of functional gastrointestinal disorder in the past and during the course.
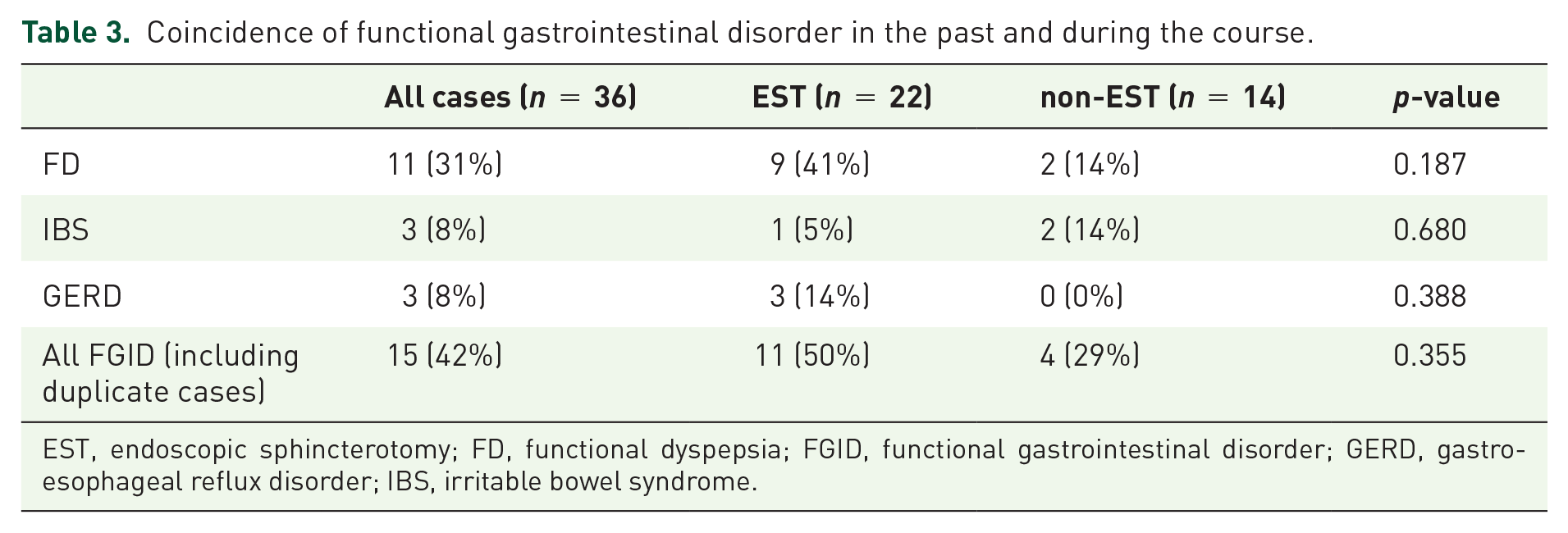
EST, endoscopic sphincterotomy; FD, functional dyspepsia; FGID, functional gastrointestinal disorder; GERD, gastroesophageal reflux disorder; IBS, irritable bowel syndrome.
As an early complication, PEP and post-ERCP cholangitis were observed in 36% (8 out of 22) and 18% (4 out of 22) of the EST group and 14% (2 out of 14) and 7% (1 out of 14) of the non-EST group, respectively (Table 4).
Adverse events after ERCP.

ERCP, endoscopic retrograde cholangiopancreatography; EST, endoscopic sphincterotomy.
As a late complication, two cases of calculous cholangitis were observed in the EST group (2 and 4 years after the first treatment). In the non-EST group, two cases (both type I) of calculous cholangitis were observed 4 and 14 years after the first ERCP.
All of these four cases belonged to type I, requiring two or three treatments for the complications. Late complications occurred in 19% (4 out of 21) of all type I cases. The mean period to onset of late complications was 6.0 ± 5.4 years, and the mean age at onset of complications was 82 ± 5.5 years. There were no differences in the incidences of short-term and late complications in both groups. No procedure-related deaths or disease-related deaths occurred.
Between the two groups, there were no differences in patients’ background characteristics, clinical outcome, incidence rate of FGID, and adverse events. The clinical course can be favorable if the treatment is appropriately selected according to the aforementioned indication criteria for EST. However, there are many cases of relapse during the course. Thus, the patients were subdivided according to symptom recurrence, and the factors related to recurrence of symptoms were analyzed by univariate and multivariate analyses.
Univariate analysis showed that FD was a significant risk factor for SOD recurrence (p < 0.01) (Table 5). Two variables with p-values less than 0.1 on univariate analysis were included in multivariate analysis. On multivariate analysis to identify factors related to the recurrence of symptoms after ERCP, history of FD or new onset was related to SOD recurrence (Table 6).
Risk factors for symptom recurrence in biliary-type SOD patients (univariate analysis).
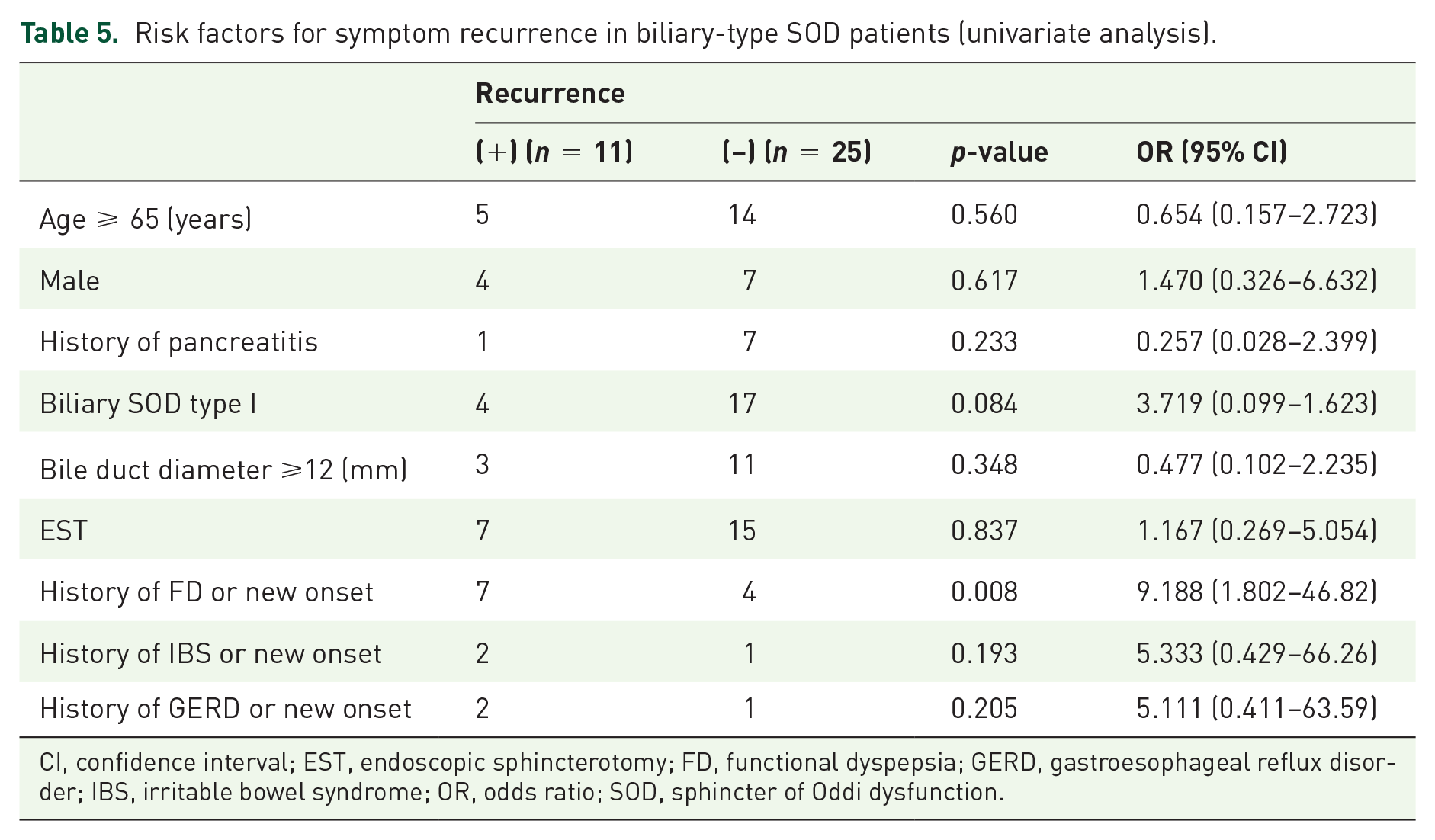
CI, confidence interval; EST, endoscopic sphincterotomy; FD, functional dyspepsia; GERD, gastroesophageal reflux disorder; IBS, irritable bowel syndrome; OR, odds ratio; SOD, sphincter of Oddi dysfunction.
Risk factors for symptom recurrence in biliary-type SOD patients (multivariate analysis).

CI, confidence interval; FD, functional dyspepsia; OR, odds ratio; SOD, sphincter of Oddi dysfunction.
Discussion
Biliary-type SOD is an organic or functional disease that causes repeated biliary pain,20–22 especially in post-cholecystectomy patients. 23 Conventionally, biliary SOD is classified into three types: types I, II, and III.20,24 EST has been confirmed to be an efficient treatment for SOD.25–27 Response to treatment is strongly related to the Milwaukee classification 24 and manometric findings. 28 However, many SOD cases may be controlled by medical treatment.29,30 In this study, 39% (14 out of 36) of the cases diagnosed as SOD were not treated endoscopically, and the symptoms were then controlled medically. Indeed, there are many cases in which EST seems effective, but even in such cases, there is a possibility that symptoms may be controlled without EST. However, EST does not change symptoms in many cases. Especially, in type III, EST has been proven to have no effectiveness. 4 Therefore, type III was excluded from the diagnostic criteria of SOD in Rome IV criteria. 14 According to the criteria, type III cases were excluded in this study. In clinical practice, it is considered that the distinction between type I and type II is difficult to strictly divide between organic stenosis and functional abnormality as in the Rome IV criteria. Both factors are thought to be involved in each pathophysiology to different extents. For this reason, in this study, both type I and type II were treated according to the frequency of severe pain.
In this study, the short-term effectiveness rate of EST was high, and the symptom recurrence rate was also high. The present result for the retreatment rate was similar to the past reports. 8 However, only in cases of type II, the retreatment rate is reported to be relatively low, at 4.7%. 31 Although the frequency of severe pain before EST is unknown in the report, it may be related to the recurrence rate.
Sphincter of Oddi manometry (SOM) is considered to be necessary to determine the indication for EST in types II SOD. Although there are reports that EST for type I2,32 and manometry-confirmed SOD1,10,33 can obtain long-term remission, there are reports that the improvement rate is not as high as expected.30,34,35 Furthermore, the results of SOM are not always reproducible,7,36 and the indication for EST cannot be decided based on one examination. 36 Evaluation of symptomatic improvement is subjective; it is difficult to judge the effect of the treatment. In theory, it is preferable to compare by evaluation using a unified questionnaire, and so on. As for SOD, there is no such score at present, but pain evaluation by a score was carried out experimentally in the EPISOD trial. 4 In this study, the symptom of SOD was finally controllable in most patients with or without endoscopic treatment. Even severe abdominal pain that required hospitalization could be relieved so as to not interfere with daily activities by endoscopic and medical treatment. EST is effective in most cases if its use is limited.1,2,32 However, there are not many cases for which EST is necessary.4,29,30 For this reason, EST for SOD continues to be controversial. From the results of this study, unnecessary EST can be avoided by deciding whether or not endoscopic treatment should be performed depending on the pain frequency. In fact, the incidence rate of PEP in EST group is very high at 36%. The incidence rate of PEP was 7–33.9% when ERCP was performed on a suspected SOD case in previous prospective studies.26,37,38 Even in suspected cases of SOD, the incidence of PEP is very high. In our study, the incidence of PEP seems to be even higher because we performed EST on confirmed SOD cases.
However, SOD has aspects of a functional disorder. 11 There has been a report on the relationship between IBS and papillary sphincter abnormality. 12 In the report, duodenal distension reproduced SOD symptoms in all but one patient. Furthermore, the patients showed high levels of somatization, depression, obsessive-compulsive behavior, and anxiety. The researchers concluded that abdominal pain in type III SOD patients may not originate exclusively from the biliary tree. In this study, some patients had symptoms of FD, IBS, or GERD before the SOD occurred or after improvement of biliary pain due to SOD, even if they were not type III. There has been a report that psychosocial distress may cause papillary motor dysfunction in SOD patients. 11 It has been pointed out that each disease may overlap with FGID, which is closely related to stress.39,40 Considering the functional disorder aspect of SOD, other FGID may develop synchronously or asynchronously with SOD. The prevalence of both FD and IBS was higher in women than in men.41,42 The frequency of SOD also tends to be higher in women than in men. However, the frequency of SOD in women is much higher in the literature3,8,11,29,30 than in our series (83–97% versus 70%). This may be related to the fact that there are more elderly SOD patients in our series than in the literature3,8,11,29,30 (age 65 versus 44–45).
In this study, the recurrence rate of symptom in biliary SOD was high in patients who had a history of FD or newly developed FD. Symptom recurrence after EST improves with an additional incision in cases of an insufficient incision or restenosis, 31 and similar results were obtained in the present cases. From the viewpoint of complications of FGID, the ease of recurrence of symptoms may be related to visceral hypersensitivity regardless of endoscopic treatment.
There have been few reports describing complications of the biliary tract in SOD after long-term follow-up. In this study, there were four cases of biliary stones with cholangitis due to biliary infection after EST and ERCP. The mean period to onset was 6 years, and the mean age at onset of complications was 82 years. All cases were type I SOD. It has been reported that acute cholangitis due to bile duct stones is common in elderly people and those with biliary dilation.43,44 Furthermore, for relapse after EST for bile duct stones, older age and biliary dilation are regarded as risk factors.45–47 Although the absence of bile duct stones is confirmed by imaging at the time of SOD diagnosis, bile duct stones may develop easily because the patients are elderly and due to biliary dilatation (type I SOD).
This study has some limitations. First, this was a retrospective, single-center study, and the number of cases was relatively small because typical SOD cases were rare. Second, an evaluation questionnaire often used for FGID was not used. Therefore, since the history and new onset of FGID were judged based on the symptoms found on the medical records of the patients, the incidence of FGID may have been underestimated.
Conclusion
Both endoscopic and medical treatments for biliary-type SOD have high effectiveness according to the indication criteria, but recurrences are common. The recurrence of symptoms of biliary-type SOD was found to be related to new onset or history of FD. Complications associated with biliary tract were relatively common in the long-term course of biliary type I SOD. Because there is no report on the risk of recurrence of SOD and late complications, attention may be required on long-term follow-up.
Footnotes
Acknowledgements
The authors would like to thank all of their colleagues at the institution for their work in data collection. The authors would also like to express their deep gratitude to Yukio Yoshida, Professor Emeritus of Jichi Medical University, for giving them useful advice and the opportunity to start the research.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Institutional Review Board of Jichi Medical University Saitama Medical Center (approval no. S16-030). The Institutional Review Board waived the need for ethical approval and the need to obtain consent for the collection, analysis, and publication of the retrospectively obtained and anonymized data for this non-interventional study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.