
Abstract
Country-specific institutional quality is one of the traditional factors of location choice of multinational corporations. However, the related literature for a long time has ignored the effect of the health system of the economy on attracting foreign direct investment (FDI). This study is an attempt to bridge the gap in the related literature and focus on the joint impact of country-specific institutional quality and health on FDI inflows for a panel of 44 developing countries over the period 2000−2022. The hypothesis of the study suggests that countries with strong institutional quality and good quality of health would attract more FDI. On the contrary, countries with low quality health levels and quality of institutions will struggle to bring FDI into the country. The results of the model strongly support our hypothesis. Our results are robust to alternative measures of the quality of health in the country. From a policy point of view, countries are expected to enhance the quality of health and institutions in the country to attract more FDI.
Introduction
The country-specific quality of institutions and governmental policies to attract foreign direct investment (FDI) are some of the important factors of the host economy that enhance the growth of multinational corporations (MNCs) in the country. Although there exists a plethora of studies that focus on the drivers of FDI inflows in a country, one of the factors that has been under-investigated is the health sector of the host economy. Several questions can arise. How is the health care system related to FDI of the host country? What is the role of the institutions of the host country in this regard?
The year 2023 was a year of celebration for the World Health Organization (WHO) and several countries worldwide, as they saw a record number of disease eliminations. This was achieved through collaborative actions from different countries and health partners all over the world. In March 2023, WHO announced that Azerbaijan and Tajikistan were free from malaria. Belize was announced malaria-free in June 2023. Egypt was the first country to achieve ‘gold tier’ status in the elimination of hepatitis C (WHO, 2023). On a similar note, Ghana was able to eradicate Human African trypanosomiasis, which is a disease related to life-threatening sickness found in the rural population of Sub-Saharan Africa. In another story, Bangladesh and Lao People’s Democratic Republic eradicated lymphatic filariasis, which was commonly known as elephantiasis, a disease transmitted by mosquitoes. In addition to this, on 5 May 2023, the WHO Director-General declared COVID-19 is no longer a global emergency. The worldwide signs were indeed promising, particularly for the low-to-middle-income countries. But areas of concern remain. Bangladesh, Indonesia and Nigeria are some of the Asian countries with poor and marginalised women facing the risk of cervical cancer. The latest estimates show that 140 countries have been enrolled in the HPV (Human Papillomavirus) vaccination goal, ensuring a widespread objective to reach the goal of vaccination of young women towards 2030. Along with this, the headquarters of WHO monitors health-related signals throughout the world. In 2023, WHO responded to 65 emergencies, among which 22 are new. Most of them are related to conflict in countries such as the Democratic Republic of the Congo, Ethiopia, Haiti, Myanmar, Sudan and Ukraine. The above goals were not reached in 1 year. WHO and several other organisations related to the health sector acted to prevent, detect and respond to different disease occurrences over the years. On the other hand, the country-specific quality of institutions and governmental policies are some of the major determinants that design and implement the health system of a country and address the health-related challenges. Effective health systems are essential for ensuring that healthcare services are accessible, efficient and affordable, playing a crucial role in promoting economic growth.
The importance of the healthcare sector in driving development is a crucial aspect of social progress. According to Bloom et al. (2004a, 2004b), Alsan et al. (2006) and Ogundari and Awokuse (2018), health is an essential part of human capital. Ill health and disability hinder human capital accumulation and have a negative impact on the economy. In addition, health has direct effects on the workers’ productivity. Physically and mentally fit workers are more active and robust than those who have compromised health conditions and therefore contribute more to the economy. Ribero (1999), Savedoff and Schultz (2000) and Schultz and Tansel (1997) analyse the effect of good health on both earnings and productivity. Accordingly, good health in turn increases the absorption capacity of the nation that attracts FDI. Therefore, the condition of the health system of a nation can be considered as an important factor to attract FDI along with infrastructures, education, labour force and R&D expenditure (see Blomström, 2006; Ingram & Silverman, 2002).
Though there exist several studies trying to associate human capital with FDI, empirical evidence between the health quality of a country and the inflow of FDI is noticeably absent in the literature. This study tries to fill the research gap in this respect by discovering the link between FDI, health and institutions. We focus on how advancement in the level of healthcare system of a country influences the FDI inflow while considering the country-specific quality of institutions. In this context, we consider the country-specific institutional quality to investigate the conditional link between FDI and health quality of a nation for a set of 44 developing countries over the period 2000–2022. In this study, we use OLS and fixed effect modelling to find the conditional influence of health quality on FDI inflows for different levels of country-specific quality of institutions.
The rest of the article is structured as follows. Section ‘Literature Review’ contributes to the survey of the literature on FDI, institutions and health. Section ‘Research Gap, Objective of the Study and Hypothesis Building’ studies the research gap, the objective of the study and hypothesis building. Section ‘Empirical Model, Data and Methodology’ discusses the model, data and methodology, followed by the ‘Results’ Section. In Section ‘Initiatives to Improve Health Situation in the Developing Countries’, we discuss the initiatives taken by the WHO to improve the health situation in the developing countries and also propose a rough sketch of a model that says about the interlinkage between health, FDI and institutions. Section ‘Conclusions and Policy Recommendations’ concludes with the limitations of the study and policy analysis.
Literature Review
FDI promotes greater integration of a country with the world economy through the transfer of technology and capital, upgradation of skill and promoting human capital formation in the host country through the spillover effect. It has been well recognised in the related literature that investment is a major factor that acts as a driver towards economic growth and development. However, sustainable growth and development may not be achieved by investment alone. In the relevant literature, there exist two strands of thought that determine the selection of the location of FDI in the world. One of the strands in the literature is dependent on the resource-based view, and the other embraces the institutional view. According to Porter (1990), the resource-based view focuses on resources, markets, capabilities and the firm’s technical efficiency. On the other hand, the institutional approach laid by Dunning and Zhang (2008) and Dunning (2014) considers the institutional environment where the multinationals operate. Though a large strand of the institutional literature in this respect supports the idea that FDI and institutions of a country are positively related and they have a positive impact on the health quality of the country, COVID-19 describes the worldwide disorder where it has created an unparalleled socio-economic problem both for institutionally strong and weak nations. It has caused an unbelievable interruption to the world economy, and therefore, the importance of the health care sector as a potential engine for development has become one of the most important areas of discussion in the present scenario. Country-specific institutional level impacts the flow of FDI to different countries. There are many studies where the impacts of institutional quality on FDI have been examined. According to Globerman and Shapiro (1999, 2002), the inflow of FDI in a nation is determined by ‘governance infrastructure’, which is measured by a composite index of governance (see Kaufmann et al., 1999). The index was constituted taking into consideration the following parameters, such as political and civil liberties, political instability, violence, regulatory burden, government effectiveness and rule of law and bribery. Accordingly, a country’s governance infrastructure index has a positive impact on the inflows of FDI. Following Globerman and Shapiro (2002), a similar study done by Bhardwaj et al. (2007) find a positive association between governance infrastructure and FDI. In a recent study, Dang et al. (2021) investigated the factors that attract the inflow of FDI in ASEAN-7 with a set of panel data. The importance was given to tax burden, institutional quality and some macroeconomic factors in attracting FDI inflows. The empirical results indicated that some of the factors, like economic growth, quality of economic institutions, inflation and so on, positively contribute to attracting FDI in the economy, whereas there are some factors (e.g., quality of political institutions and population growth) that have a negative association with FDI inflows. In another study, Peres et al. (2018) show that the institutional quality (institutional quality is measured by the sum of two variables, one is the control of corruption and rule of law indicators) has a positive and significant effect on FDI inflows for the developed countries in comparison with developing countries. The impact on the developing nations is insignificant due to the poor institutional structure of the countries.
The positive effect of institutional quality on the inflow of FDI was demonstrated by Wei (1997, 2000), Daude and Stein (2007), Bénassy-Quéré et al. (2007), Pearson et al. (2012), Dutta et al. (2017), Riedl (2010), Arbatli (2011). While Riedl (2010) and Arbatli (2011) showed a positive association between political stability and inflow of FDI, Wei (1997, 2000), Bénassy-Quéré et al. (2007) and Dutta et al. (2017) showed positive evidence between the rule of law and FDI inflow. The positive connection between inflow of FDI and investment profile of a country is reflected in the works by Siddica and Angkur (2017). In another set of studies, the negative correlation between corruption and FDI inflows is studied by Wei (2000), Al-Sadig (2008), Mateev (2009), Kersan-Škabić (2013), Du et al. (2012), Bénassy-Quéré et al. (2007) and Dutta et al. (2017). However, a positive connection between corruption and FDI inflows is also studied by Jiménez et al. (2011) and Barassi and Zhou (2012). In another research, Siddica and Angkur (2017) studied the effect of health, institutions and other possible determinants on FDI inflow for 40 countries over the period 1990−2010 by using the panel data model.
In most of the developing and underdeveloped nations, the public healthcare sector that tries to meet the need of the poorer sections of the population, suffers from poor infrastructural facilities. Thus, much more investment on health sector is required to make the nation healthier, so that the people of the nation can work more efficiently and make the nation more fit to engross FDI inflow. A healthy workforce in affluent nations is seen to be a significant factor in inviting FDI inflows towards nations.
The indirect mechanism of health affecting economic performance is through education and work experience. Bhargava et al. (2001) showed that increased cognitive activity and higher school turnout increase the potentiality of children to become more educated and higher learning adults. Moreover, healthy workers have lesser rates of absenteeism, extended life expectancies and they can obtain more job-related experiences. Accordingly, improvement in the quality of health has a more pronounced growth effect for developing countries compared to developed or industrialised countries. The relation between the asymmetric effect of FDI and life expectancy for Pakistan was studied by Rahman et al. (2022) over the period 1980−2020. The results of the model verify that positive changes in FDI have bidirectional causality to life expectancy, while unidirectional influences from FDI to life expectancy are constructed by negative shocks. From the policy perspective, the study recommended government expenditure in the health care system to improve the life expectancy at birth (LEB) of the people of the country. The relation between infant mortality rate, life expectancy and FDI was once again addressed in a study by Ma et al. (2022) for emerging ASIAN economies over the time period 1991−2019 using the ARDL method. They studied the effect of FDI and external debt on the health outcomes for ASEAN countries. According to the study, an increase in external debt was negatively related to health consequences (LEB and infant mortality rate) in the long run, whereas an increase in the inflow of FDI led to a fall in the infant mortality rate and a rise in the life expectancy in the long run. From the policy point of view, the study recommended a rise in the health expenditure to cut the infant mortality rate and improve the life expectancy of the population. The role of LEB on the inflow of FDI for a host country was also studied by Alsan et al. (2006). They investigated the role of public health in the inflow of FDI over the time period 1980−2000 for a set of 74 developed and developing countries. The empirical results predicted that population health has a positive and robust effect on the inflow of FDI for low- and middle-income countries, and that raising the LEB (while controlling for other variables) can increase the FDI inflows by 9%. In the article, Socoliuc et al. (2022) validated that higher institutional quality is associated with reduced child mortality rates and improved life expectancy within the European Union region. In a similar article, Vian (2020) highlighted that the presence of corruption weakens the capacity of health systems, economic growth and overall development of a nation. Therefore, addressing corruption through interventions and allocating resources towards prevention and control are crucial components of strengthening health systems for Universal Health Coverage (UHC). Mackenbach and McKee (2015) found a significant positive association between the quality of democracy and indicators of healthy policies. Similarly, Makuta and O’Hare (2015) proved that better governance quality is related to improved health consequences in Sub-Saharan Africa. This indicates that public health expenditure is more effective in countries with higher levels of governance compared to those with lower levels.
On the other hand, health can affect the level of FDI a country can fetch. While FDI has undoubtedly brought growth and development in many developing and developed nations, its relationship with health has largely remained unexplored. According to the WHO (2001), healthy workers are central to attract the foreign investment as health is directly related to workers’ productivity. According to Globerman and Shapiro (2003), health is an important aspect of human development, and the quality of health of a country has serious positive implications in attracting inward FDI.
As per the literature survey, there exists a restricted number of studies that link FDI and health quality of a country (see Alsan et al., 2006; Globerman & Shapiro, 2002), although it is proven in the related literature that health is an integral part of the human development of a nation. The effect of health cost on FDI for a set of low- to high-income countries has been taken up by Chen and Sheng (2013). They used two stage panel regression model for the period 1995−2010. Olofin (2019) studied the factors attracting FDI in Nigeria using a fully modified ordinary least squares (FMOLS) model. They found that health expenditure, along with other variables (e.g., tax revenue, net trade, human capital, etc.), is positively related to income growth. In another study, Kumari and Sharma (2018) examined the link between the health of the population, FDI inflows and economic growth in the context of the Indian economy over the time period 1990−2013 using time series data. They used applied cointegration and vector error correction (VEC) model in the study. Accordingly, there exists a long-run relationship among the variables. In another study, Giammanco and Gitto (2019) examined the quality of health on the inflow of FDI and found a positive association between the two variables. The study examined the role of different institutional settings for 28 member countries of the European Union (EU) in attracting FDI. In another study, Aziza et al. (2019) investigated the relationship between military health expenditure and FDI inflows, conditioning on the exposure of a country to armed conflict in the long run. The inflow of new immigrants to a country and its effect on public and out-of-pocket health expenditure was studied by Rana et al. (2020) for 33 OECD countries over the period 2000–2015. It was found that the increasing inflow of immigrants is significantly related to out-of-pocket expenditure but not to public health expenditure. However, the role of FDI was not studied in the model. In a study, Dalango (2020) examined the empirical relationship between inflow of FDI and health (along with other determinants) for Ethiopia, taking the time period 1981−2018. Similarly, in a recent article, Raeskyesa and Suryandaru (2020) studied the empirical relationship between competitiveness and FDI inflows for ASEAN countries over the time period 2007−2017. The study revealed that most of the countries have a strong positive association between the two variables, provided institutions, health, human capital and so on have a strong effect in attracting FDI. The policy recommendations suggested that institutional quality and human capital of the ASEAN countries should be improved to increase the health and basic education of these countries. The dynamic relationship between health expenditure and FDI inflows for ASEAN countries was also studied by Verma (2021). The study noticed the potential of FDI in developing the health care expenditure of a country. It was suggested (see Azolibe et al., 2020; Kolawole & Odubunmi, 2015) that the countries should incur more expenditure on projects related to energy, infrastructure, road, health and education in order to boost economic growth and attract more FDI. A series of studies (see Immurana, 2020; Immurana et al., 2023) examined the effect of FDI inflow on health indicators like life expectancy and death rate for African countries. Immurana et al. (2023) recommended increasing the health of the population of the host country by increasing access to quality health care and vaccination, improving sanitation facilities, safe drinking water, among others, to attract more FDI. In a series of recent studies (see Shah et al., 2022; Zhang et al., 2023), the effect of FDI inflows on human health was studied for China. While Shah et al. (2022) studied the impact of FDI on human mortality consumption in China, Zhang et al. (2023) aimed to examine the link between FDI, renewable energy consumption, CO2 emissions and population health quality over the period 1980–2020.
Though most of the above-mentioned literature confirms the positive association between health and FDI, however, to mitigate the risk of health hazards, foreign investors can refrain from investing in areas with high-risk potential. One of the most classic instances when disease intervened with investment took place during the construction of the Panama Canal. The predominance of the yellow fever during 1882 and 1888 forced Ferdinand de Lesseps and the French to leave the project. The recent outbreak of the SARS coronavirus is another example when the flow of FDI dampened around the world. These trends quickly reversed once the epidemic was controlled, but they showed us that prolonged epidemics (e.g., HIV/AIDS or malaria) could have severe effects on the worldwide flow of FDI. Asiedu et al. (2015) in a study showed the negative effects of HIV/AIDS virus on FDI for a panel data of 84 nations over the time period 1990−2008. In a similar work, Azémar and Desbordes (2009) showed the positive effects of the absence of any epidemic on the net FDI inflow in Sub-Saharan Africa over the period 1985−2004. In another study, Alsan et al. investigated the role of public health on the inflow of FDI over the time period 1980−2000 for a set of 74 developed and developing countries. The empirical results indicate that population health has a positive and robust effect on the inflow of FDI for low- and middle-income countries, and that raising the LEB (while controlling for other variables) can increase the FDI inflows by 9%. The effect of the COVID-19 pandemic on FDI inflows was once again taken up by Hayakawa and Mukunoki (2021). Accordingly, there was an adverse effect of COVID-19 on the trading countries, and these were relevant since July, 2020. In another study, Fang et al. (2021) showed that figures related to the pandemic (new figures of death, figures related to confirmed cases and figures related to cumulative confirmed cases) have a crucial negative impact on FDI. By using monthly bilateral FDI data, Fu et al. (2021) identified that: (a) the pandemic reduced both the wide and rigorous boundaries of FDI, (b) the death rate condensed FDI limits, (c) For both OECD and developing countries, FDI was more delicate to the contagion circumstances in host countries and (d) the most harshly exaggerated sectors’ FDI was service sector’s FDI by the epidemic. In another study, Nawoa and Njangang (2021) examined the pandemic impact on FDI in 79 industrialised and emerging nations. Accordingly, the total number of deaths and cases was negatively correlated with FDI.
Research Gap, Objective of the Study and Hypothesis Building
After extensive review of the related literature, it has become evident that foreign direct investors place substantial importance on the institutional quality of the host country. As a result, a considerable portion of research has been centred on investigating the connection between FDI and institutional factors. Conversely, there lie a limited number of studies that are dedicated to exploring the relationship between FDI and one of its pivotal determinants—health capital. Moreover, to the best of our knowledge, none of these studies tries to explore the conditional relationship between health and FDI inflows of a country given the country-specific institutional quality.
This notable absence underscores the fact that researchers have not only neglected the role of the health of a nation on the inflow of FDI but also have ignored the conditional impact of both health quality and institutional quality on the inflow of FDI. This aspect, which investigates the interplay between health quality and the quality of institutions, has remained unexplored in the related literature, highlighting an area suitable for exploration.
The hypothesis of this study says there lies a positive relationship between the quality of health of a country and the inflow of FDI, given different levels of country-specific quality of institutions. In other words, countries with good health conditions will receive a significant amount of FDI if they have good institutional quality. On the contrary, low institutional quality will have a negative impact of health on FDI inflows.
Empirical Model, Data and Methodology
This section discusses the empirical modelling, data and methodology used in this study to investigate the relationship between FDI, institutional quality of countries and health in an empirical set-up. According to the hypothesis of this study the conditional effect of institutional quality, measured in terms of the combined institutional index (COMBINDEX which is a combined index of the five ICRG variables such as investment profile (invpro), government stability (gov_stab), socio-economic conditions (soc_cond), internal conflict (intr_cont) and external conflict (extr_cont), has a positive significant effect in attracting FDI with increasing quality of Health. We have used a panel of 44 countries (See Table A1) over the time period 2000−2002 and applied fixed effects modelling. 1 In this set-up, we have used country-specific health expenditure as a percentage of GDP (HEPGDP) as a proxy variable to measure the level of health for different countries. Another ICRG variable, LEB, has been used for a robustness check.
The Model
The main focus of this study is to examine the role of quality of health in attracting FDI, conditioned on the level of quality of institutions. The joint/conditional effect between the two variables (COMBINDEX and HEPGDP) in attracting FDI is given in Equation (1) following the related literature (see Sen & Sinha, 2017; Sinha & Saha, 2022; Sinha et al., 2024; Sinha & Das, 2025) the conditional effect is demonstrated for the panel fixed effects technique in Equation (1) over the period 2000−2022 for 44 developing countries.

where, FDIPGDP is the FDI as a percentage of GDP and is our dependent variable. The focus variables are COMBINDEX (measure of institutional variable in terms of a combined index of five variables), HEPGDP (measure of HEPGDP of a country) and the interaction term HEPGDP*COMBINDEX (which captures how the COMBINDEX of a country in combination with strong health expenditure can attract FDI in countries). Z is a vector of control variables,
Our variable of interest is the interaction term HEPGDP*COMBINEDX. A positive coefficient 훼3 indicates that the joint effect of COMBINDEX and HEPGDP increases the level FDI inflows in a country. The quality of institutions and the level of health expenditure might not work effectively at the individual level, but they are effective in attracting FDI jointly. The anticipated sign of the 훼3 coefficient is positive. A positive 훼3 implies that nations that are better placed in the institutional index according to COMBINDEX receive relatively more FDI as their level of health expenditure rises. The summary statistics and correlation matrix are given in Table A2 and Table A3, respectively.
Control Variables
The selection of control variables is as per the related literature. The control variables as chosen in this study are:
Urban index of a country—percentage of urban population to total population (URBAN). Macro-economic instability of a country—inflation consumer prices, annual percentage (INFCP). Govt size of a country—general government final consumption expenditure as a percentage of GDP (GGFCEPGDP). Measure of the infrastructure of a country—telephone lines per hundred people (TEL). It is anticipated that a lower inflation rate, better telephone service, a smaller size of the government and greater urbanisation (proxy for market size) would foster FDI inflows (see Al-Sadig, 2008; Noorbakhsh et al., 2001).
Data Sources
Data for all the institutional variables were taken from ICRG (
Methodology
Equation (1) is estimated by a panel of the least squares method for 44 countries over the period 2000–2022.3 Two-way fixed effects (country and year fixed effects) are used in this study to capture any unobserved effects specific to individual cross-sectional units or time.
Results
We begin our empirical analysis by looking graphically at the bivariate relationship between health expenditure as a % of GDP and FDI as a % of GDP for the countries over the time period 2000–2022. To check this bivariate relationship, we divide the countries in four percentiles according to their institutional quality (countries below the 25th percentile, countries below the 50th percentile, countries below the 75th percentile and countries below the 100th percentile) measured by the COMBINDEX rank (see Figures 1a–1d). In most of the cases, we have a positive relationship between health expenditure and inflow of FDI averaged over the years. Countries within the 25th and 50th percentiles of COMBINDEX (e.g., Armenia, Bangladesh, Colombia, Ecuador, Ethiopia, Haiti, India, etc.) have a positive correlation between FDI and health expenditure. However, countries within 75th percentile had a negative correlation between the variables.
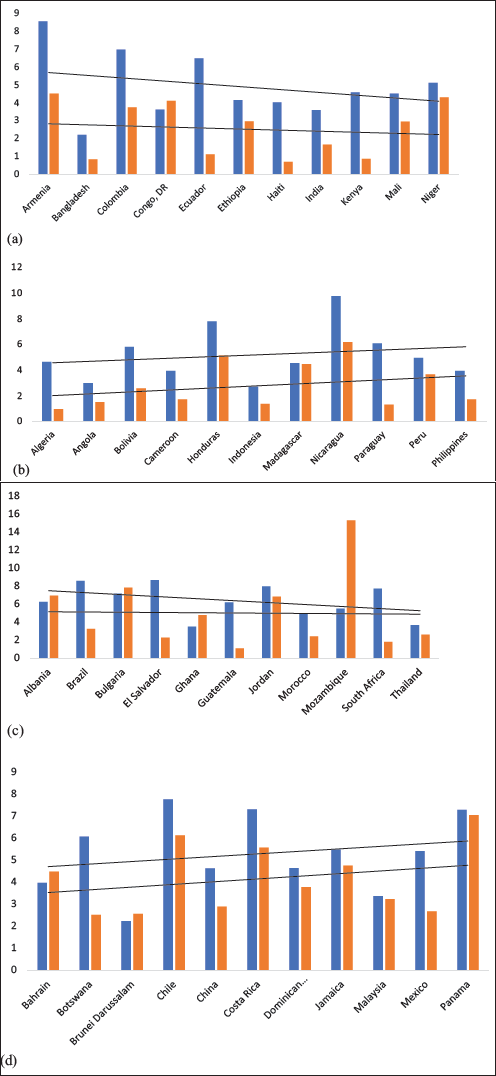
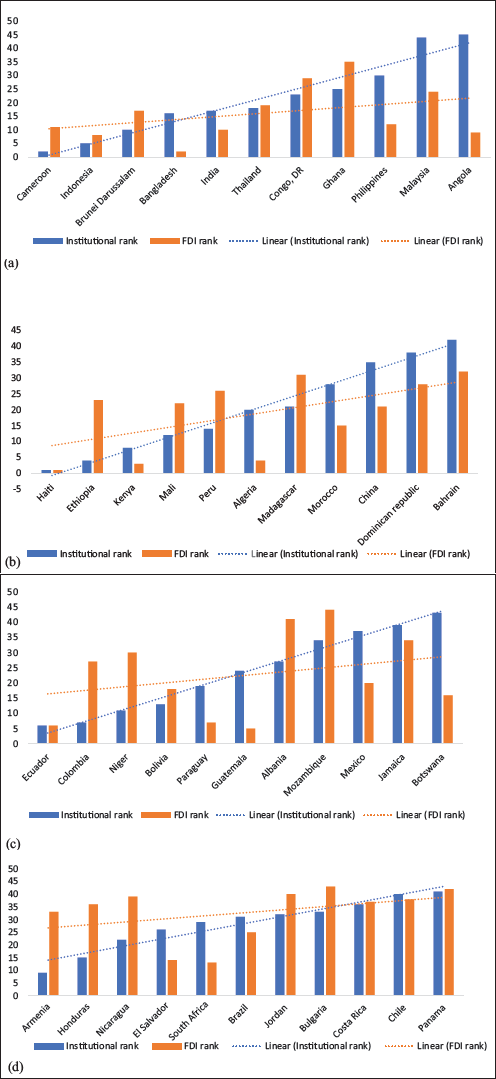
In a similar fashion, we have grouped the countries according to their level of health expenditure and have derived the relationship between FDI and COMBINDEX averaged over the years 2000−2022. Most of the cases show a positive relationship between COMBINDEX and the inflow of FDI.
The above analysis helps us to check the marginal effect of health expenditure on FDI for different levels of Institutional quality graphically (see Figures 1a–1d) and again the marginal effect of institutional quality on FDI for different levels of health expenditure (see Figures 2a–2d).
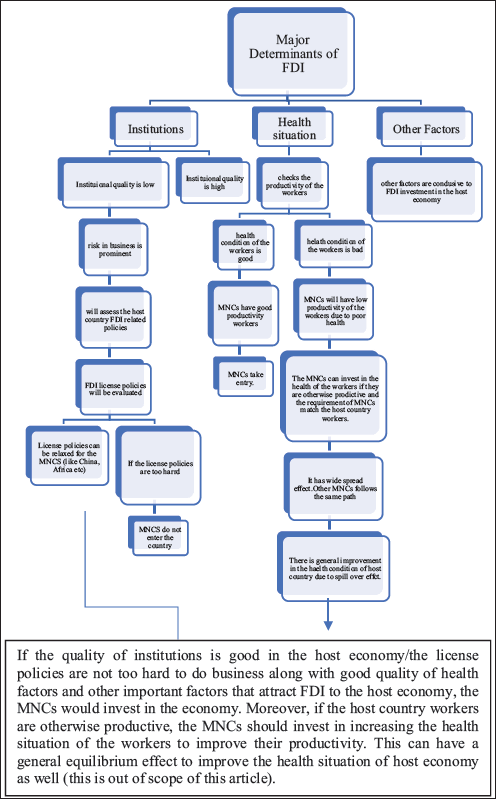
Proposed Model of Health, Foreign Direct Investment (FDI) and Institutions for the Developing Countries by the authors.
Regression Results
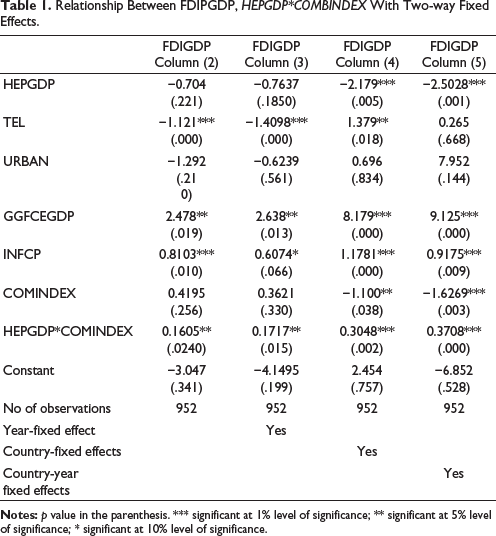
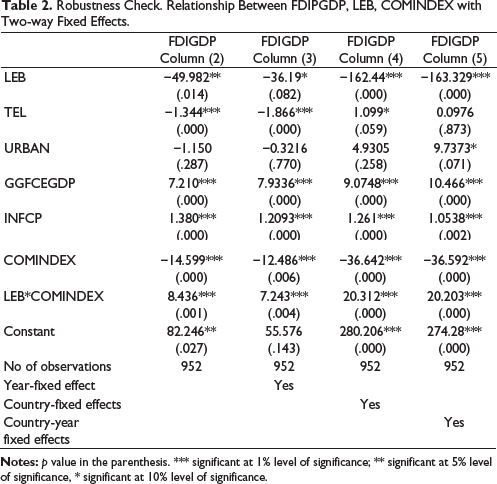
The relationships between the combined institution index (COMBINDEX) with FDI are explored extensively using OLS and panel fixed effects, and the results are reported in Table 1. The coefficients of health expenditure and COMBINDEX are negative at the individual level but significant, suggesting that health expenditure and COMBINDEX are not able to bring FDI inflows at the individual level. However, the interaction term between health expenditure and COMBINDEX is positive and significant, indicating that the level of health expenditure and quality of COMINDEX are jointly effective in bringing FDI (see Table 1). The two-way fixed effect results also show that the joint effect between COMBINDEX and health expenditure is positive (see columns 2–6 for Table 1). This supports our core hypothesis that countries with strong institutions are more likely to attract FDI if they have a good quality of health expenditure. Our hypothesis passes the robustness check (for robustness check we have used LEB, see Table 2). Countries with strong institutions complemented with good quality of health expenditure will not be devoid of foreign investments. We have used an additional variable called infant mortality rate from the World Bank for a robustness check. Our results are robust to all the alternative measures of health. With respect to our control variables, the coefficients of GGFCEPGDP and INFCP are surprisingly positive and significant. On the other hand, coefficients of TEL and URBAN vary in sign (see Tables 1 and 2).
Relationship Between FDIPGDP, HEPGDP*COMBINDEX With Two-way Fixed Effects.
Robustness Check. Relationship Between FDIPGDP, LEB, COMINDEX with Two-way Fixed Effects.
Initiatives to Improve Health Situation in the Developing Countries
The regional road map for improving the health results and resilience for different parts of the world is taken care by the WHO. The Southeast Asian region saw a boost in the initiatives taken after Saima Wazed assumed charges as the regional director of the WHO of Southeast Asia. Her bold initiative through extensive consultation and discussion of the roadmap was subsequently endorsed by the member states in Geneva in May 2024. In another story, in the African region, the TY Danjuma Foundation has signed an agreement to strengthen the health sector of Nigeria (a 2.2 million dollar investment agreement has been signed). Every year, 146,000 deaths are reported in Africa due to the prevalence of the use of tobacco, and Mali is no exception to this (WHO, 2023). To control the death rates caused by smoking tobacco, along with other prevailing measures, the country has increased the tax rate on imported tobacco products from 25% in 2018 to 34% in 2023. For Southeast Asian region, the road map was initiated in such a way that it can guide the member states in the persistent health problems and well-being. A holistic approach was taken instead of fragmented approach to solve the health problems of the region. Reinforcing the mental health issue along with investment in adolescent, vulnerable and information technology, were prioritised. HPV vaccination for the girls and women population has been given priority. Bhutan has launched the PEMA mental health symposium. The Second International Mental health training and workshop was hosted by Thailand with the support of WHO (2023). Recently, initiatives were taken by Bangladesh and Nepal and has also launched a mental well-being programme with the support of the WHO. In another groundbreaking story, Botswana received the WHO’s gold-tier status for the elimination of vertical transmission of HIV. In Seychelles, WHO has taken the initiative to curb obesity, which has recently shown a rising trend from 4% in men and 13% in women in 2000 to 27% and 49% in 2023, respectively. Ethiopia has seen multiple emergency health programs during disease outbreaks and climate shocks. Six decentralised operational hubs are strategically located throughout Ethiopia (Addis Ababa, Jijiga, Mekelle, Bahir Dar, Hawassa, Gambella), and each hub is well equipped to handle an emergency situation (WHO, 2023).
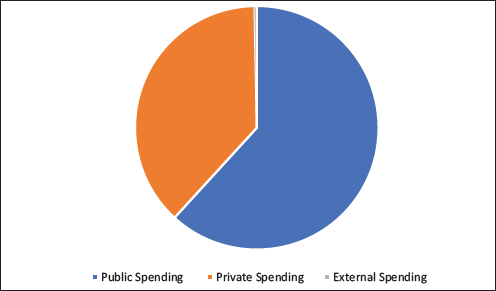
The Global Health Expenditure Report focuses on the health spending of 2021, the second year of the pandemic (Figure 3). WHO Report (2023) acknowledges health disruptions caused by COVID-19, a lack of trained health workforce and less investment in education and employment. The organisation’s 2024−2025 budget aims to balance between the organisation’s normative functions and strengthening the country offices. Global spending on health reached $9.8 trillion in 2021.
Figure 4 presents the proposed model of health, FDI and institutions for the developing countries.
Conclusions and Policy Recommendations
The aim of this study is to explore the joint influence of health and institutional quality on FDI inflows. The key findings imply that health has a positive and significant effect on country-wise FDI inflows. The joint impact of health expenditure and institutional quality is positive in attracting FDI in the host country. Our hypothesis passes the robustness check. Moreover, for different levels of COMBINDEX, the correlation between health expenditure and COMBINDEX is positive for most of the cases, implying that an increasing health expenditure can accelerate the absorption capacity of a country by increasing the health quality of the economy to attract more FDI inflow. As healthy workers are the backbone of society, the objective of the social planner would be to increase the health conditions of the workers to increase the absorption capacity of the economy, thus providing enough space for being more competitive in the global economy to fetch more FDI and also have the benefit of the spillover effects of foreign investment. The health conditions can be improved by increasing the spending on health and increasing the number of trained health workers, and this has already been cited in the report of WHO (2023). However, this study suffers from data limitations. The World Bank’s data for the health expenditure percentage of GDP before 2000 is not available, which thus restricts our work from taking a broader time horizon.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.