
Abstract
Objective
Breast surgery is often followed by severe pain. Erector spinae plane block (ESPB), a regional technique used to manage postsurgical pain as well as acute and chronic pain. Adding an adjuvant to ESPB can improve its quality and efficacy. We conducted a study to evaluate the effect of adding dexamethasone to ESPB for postoperative analgesia following modified radical mastectomy (MRM) under general anaesthesia.
Methods
The study was conducted on 60 female patients posted for ultrasound-guided ESPB in MRM. These patients were randomly divided into two groups before the induction of general anaesthesia. In Group L, patients were given ESPB with 20 ml of 0.25% levobupivacaine plus normal saline, whereas in Group D, patients were given ESPB with 20 ml of 0.25% levobupivacaine plus 4 mg dexamethasone. Tramadol was given as a rescue analgesic. The duration of analgesia, verbal numerical rating scores, postoperative analgesic consumption, patient satisfaction and side effects were evaluated.
Results
The duration of analgesia was significantly longer in Group D (982.3 ± 65.7 min) when compared to Group L (711.0 ± 68.9 min) (P < .001). Total requirement of tramadol was significantly lower in Group D (133.33 ± 47.95 mg) compared to Group L (230.00 ± 46.61 mg) (P < .001). The VNRS scores in Group D were significantly lower compared to Group L at rest. Patients in Group D experienced higher satisfaction compared to Group L.
Conclusions
Dexamethasone with levobupivacaine in ESPB for MRM provides increased duration of analgesia and decreased rescue analgesic consumption with better quality of analgesia and patient satisfaction.
Introduction
Modified radical mastectomy (MRM) is the most often used therapeutic option for patients with breast carcinoma. After MRM, 30%-50% of patients experience moderate to severe acute pain, and 8%-25% of patients experience persistent postoperative pain. Approximately 25%-60% of these patients may develop post-mastectomy pain syndrome. 1
Forero et al. described the erector spinae plane block (ESPB) in 2016 as a paraspinal fascial plane block for the management of thoracic neuropathic pain. 2 In this technique, local anaesthetic is injected deep into the erector spinae muscle to block the ventral and dorsal rami of numerous spinal nerves. This block may be useful for treating neuropathic pain in addition to acute post-operative abdominal and thoracic procedures. Since then, this block has been successfully utilised in numerous procedures, including thoracotomies, percutaneous nephrolithotomies, ventral hernia repairs, and rib fractures.3–5
Despite increased awareness and developments in pain management, post-operative pain is still not adequately managed. The emerging research demonstrated ESPB as a technically simple, safe and less invasive regional anaesthetic technique to manage acute post-surgical pain in adults and children.6, 7 It is relatively a superficial block, so there are low incidences of complications like hypotension and haematoma.
Dexamethasone is a synthetic, long-acting, and highly potent glucocorticoid. It acts by binding to glucocorticoid receptors and inhibiting potassium conductance. It plays a role in modulating pain and inflammatory response by inhibiting ectopic nerve discharge, reducing inflammation, and delaying C-fibre impulses. The levobupivacaine is a more recent local anaesthetic drug with reduced cardiac and neurotoxicity and a larger threshold for systemic toxicity. The lower toxicity of levobupivacaine is mostly due to a faster protein binding rate.
As the data regarding dexamethasone use with ESPB in MRM for analgesia are very sparse, especially in the Indian population, and there are conflicting reports about its effect on the duration of postoperative analgesia. We conducted this clinical trial to evaluate the efficacy of the drug with regard to postoperative analgesia. Our primary objective was to compare the duration of analgesia provided by levobupivacaine alone and levobupivacaine plus dexamethasone in ESPB for patients undergoing MRM surgeries. Secondary objectives included pain scores, quality of analgesia, rescue analgesic consumption, to assess the side effects and the level of patient satisfaction.
Materials and Methods
This was a prospective, randomised, double-blind study. The study was conducted after obtaining institutional ethical committee approval (vide approval no. ECR/836/Inst/PB/2016/RR-20) dated 27 January 2020. This study was registered with the Clinical Trials Registry of India with registration number CTRI/2020/11/028919. We enrolled 60 American Society of Anaesthesiologists (ASA) physical status I and II, female patients with an age group of 20-65 years, posted for elective MRM surgeries, and it was carried out in accordance with the Declaration of Helsinki, 2013.
We excluded patients having a history of allergy to study medications, a history of substance use and chronic use of pain medications, patients with psychological and neurological disorders, with a body mass index >35 kg/m2, and patients with coagulation disorders. All the patients who met the inclusion criteria were included, and written informed consent was taken for participation in the study. During the pre-anaesthetic checkup visit, the verbal numerical rating scale (VNRS) was discussed and described to the patients.
Prior to surgery, all patients were kept fasting for at least 6 hours. On the night before the procedure and at 6
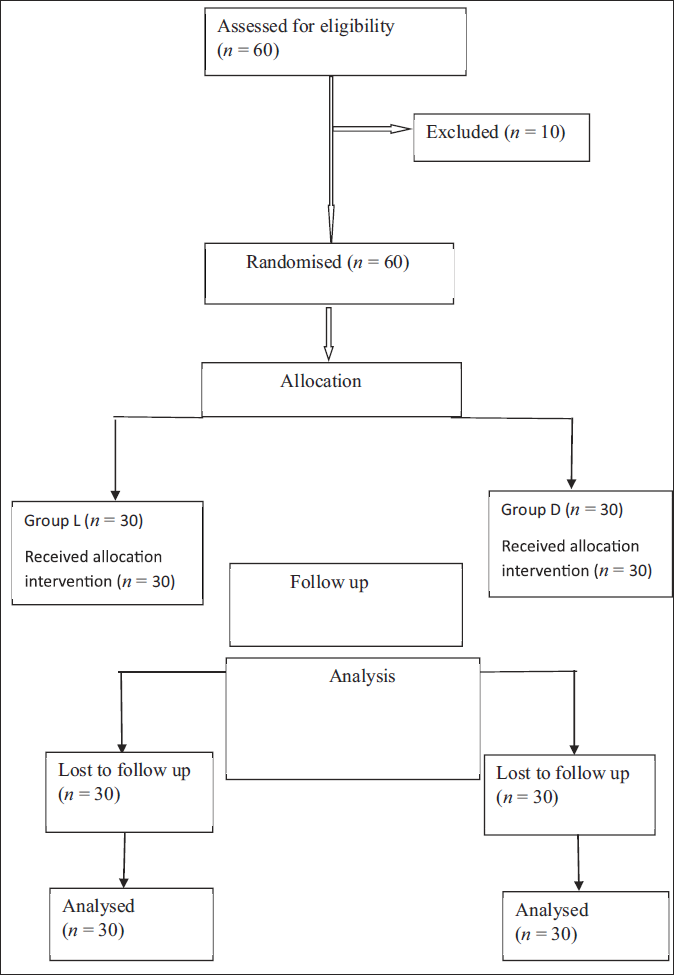
Using a computer-generated randomisation list, all patients were randomised into two groups and received either of two regimens. For Group L (n = 30), 20 ml of 0.25% levobupivacaine with normal saline and for Group D (n = 30), 20 ml of 0.25% levobupivacaine with 4 mg dexamethasone was prepared to maintain the same volume of study drug in both groups (Figure 1). The study infusions were prepared by an Anaesthesiologist not involved in study. The patient and the Anaesthesiologist observing patients in the perioperative period were blinded to the group allocation.
An intravenous (IV) access was established, and IV fluid was started as soon as the patient entered the operating room. After attaching the standard ASA monitoring, such as ECG, pulse oximeter, and non-invasive blood pressure monitor and baseline data was recorded. Prior to ESPB, patients were positioned in the sitting posture.
Ultrasound-guided ESPB were done with an in-plane technique at the T4-T5 level of the spine. A linear high-frequency (5-10 MHz) probe of a real-time ultrasound machine (Esaote Europe BV) was placed transversely to locate the level of the spinous process. Thereafter, the probe advanced 3 cm laterally until the transverse process was located.
On the transverse process, the probe was rotated at 90° and kept its positioning in a parasagittal plane. Superficial to hyperechoic transverse process shadows, three muscles, including the trapezius, rhomboid major and erector spinae, were identified. After identifying the erector spinae muscle, a stimulation needle (Stimuplex A, B. Braun Melsungen AG, Germany) was placed in a cranio-caudal direction deeply into the muscle. After injecting the study solution, the erector spinae muscle was visibly lifted, and a clearly defined hypoechoic elliptical shape was observed in the fascial plane. Sensory block was assessed by the pin-prick method in each dermatomal distribution from T1 to T8.
After performing ESPB, Preoxygenation was done for 3 min and standardised general anaesthesia was induced with IV fentanyl 1 mcg/kg and IV propofol 1.5-2.5 mg/kg. IV vecuronium 0.1 mg/kg was used for endotracheal intubation and confirmed by capnography. Anaesthesia was maintained by N2O:O2 in a ratio of 60:40 and with isoflurane (0.2%–2%).
IV paracetamol 20 mg/kg and IV fentanyl 1 mcg/kg were administered as part of multimodal analgesia, and the patients were mechanically ventilated to keep the EtCO2 at 35-45 mm of Hg. Haemodynamic parameters, such as systolic and diastolic blood pressure, mean arterial blood pressure, respiratory rate, oxygen saturation and heart rate, were noted every 5 min for the first 30 min and then every 10 min until the end of the surgery. At the end of surgery, IV neostigmine 50 mcg/kg and glycopyrrolate 10 mcg/kg were administered to antagonise the residual neuromuscular block. Patients were extubated and shifted to a post-anaesthesia care unit. The Anaesthesiologist collecting the data was clueless about the group allocation.
Every patient, assessed immediately following entrance to the PACU, and at 2, 4, 8, 12, 18, and 24 hours after surgery for pain at rest using VNRS and hemodynamic parameters. On patient demand or when VNRS ≥3, IV tramadol 2 mg/kg was given as a rescue analgesic.
The time interval starting from completion of study drug administration to the first demand of tramadol was termed as duration of analgesia. The time of first demand of tramadol, total consumption of tramadol in the first 24 hours period post-surgery, quality of analgesia (0 = Indicates no discomfort, 1-3 = Indicates mild pain, 4-7 = Moderate discomfort, 7-10 = Severe pain), patient satisfaction with pain management, a five-point numeric scale was used at the end of 24 hours (1 = Very satisfied, 2 = Satisfied, 3 = Uncertain, 4 = Dissatisfied, and 5 = Extremely dissatisfied) and side effects like hypotension, bradycardia, sedation, pruritus, nausea and vomiting were noted.
Statistical Analysis
Our primary outcome was the duration of analgesia. We needed at least 25 patients in each group based on the results of our pilot study and using t-test and α = 0.05, to detect 15% difference in duration of analgesia with 80% power, the significance level of 5% and a confidence interval 95%. To compensate for any dropouts from the study, we increased the sample to 30 patients in each group. MS Excel was used to enter the data, while SPSS 21.0 (IBM Corp., Armonk, NY, USA) was used for analysis. The continuous variables were expressed as mean and standard deviation, and categorical variables as percentages. An unpaired t-test was used to compare two group means. The chi-square test was used to find out the association between category variables. P value of <.05 were considered statistically significant, and values .001 were considered highly significant.
Results
For this study, a total of 60 patients were included for eligibility and divided into two groups of 30 patients each. All participants completed the study, and none of them were excluded (Figure 1).
Consort Flow Chart.
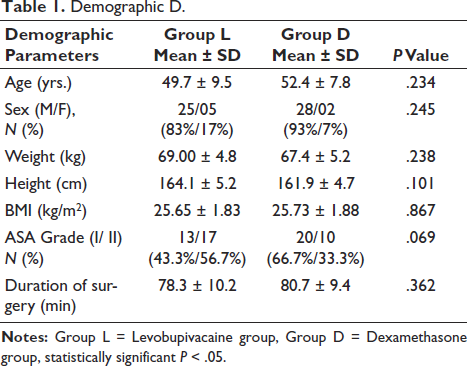
Baseline comparisons of demographic parameters showed the two groups were comparable in terms of all the parameters. Group L had a mean age distribution of 49.7 ± 9.5 years, while Group B had a mean age distribution of 52.4 ± 7.8 years (P = .234).
In Groups L and D, there were, respectively, 25 (83%) and 28 (93%) male patients and 5 (17%) and 2 (7%) female patients (P = .245). The weight distributions (in kg) were 69.00 ± 4.8 and 67.4 ± 5.2, in Groups L and D, respectively (P = .238).
The height distribution (in cm) was 164.1 ± 5.2 and 161.9 ± 4.7, in Groups L and D, respectively (P = .101). The BMI distributions (in kg/m2) were 25.65 ± 1.83 and 25.73 ± 1.88, in Groups L and D, respectively (P = .867). In Group L, there were 13 (43.3%) and 20 (66.7%) ASA Grade I and 17 (56.7%) and 10 (33.3%) ASA Grade II patients in Groups L and D, respectively (P = .069). Also, duration of surgery (in minutes) was 78.3 ± 10.2 and 80.7 ± 9.4 in Groups L and D, respectively (P = .362) (Table 1).
Demographic D.
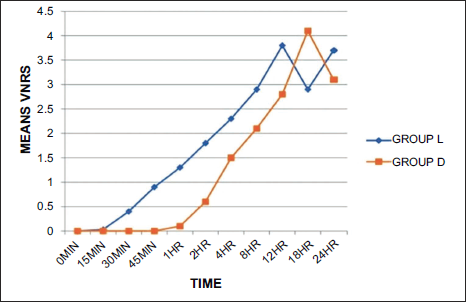
The VNRS scores during the first 24 hours postoperatively, remained below 3 in both the study groups, except at 12 hrs in Group L and 18 hrs in Group D, which correlated well with the duration of analgesia in the present study (Table 2, Figure 2).
Verbal Numerical Rating Scores.
The mean duration of analgesia (time from completion of ESPB till request of first rescue analgesia) was statistically significantly longer in Group D (982.3 ± 65.7 min) when compared to Group L (711.0 ± 68.9 min), with a P value of <.001.
The total amount of first rescue analgesic (IV tramadol) during the first 24 hours postoperatively was significantly less in Group D (133.33 ± 47.95 mg) when compared to Group L (230.00 ± 46.61 mg) with P value of <.001.
In Group D, twelve (43.3%) patients required one dose of rescue analgesic, and two (6.6%) patients required two doses of rescue analgesic. In contrast, 23 (76.7%) patients in Group L required two doses, and seven (23.3%) patients required three doses of rescue analgesic. This difference in patient requirement was statistically significant, with P value of <.001 (Table 2).
Study Parameters.
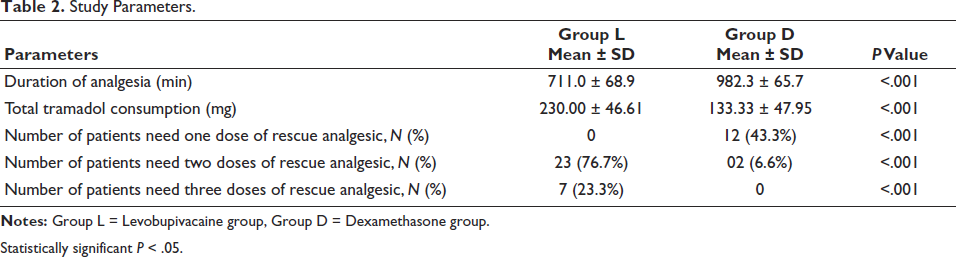
Statistically significant P < .05.
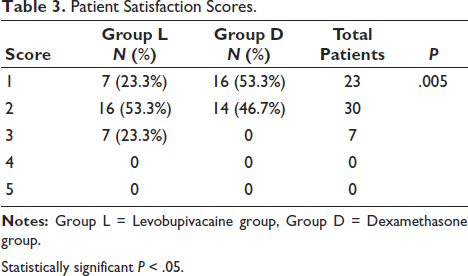
There were 7 (23.3%) and 16 (53.3%) patients with patient satisfaction scores of 1 and 16 (53.3%) and 14 (46.7%) patients with patient satisfaction scores of 2 in Groups L and D, respectively. Only 7 (23.3%) patients had patient satisfaction score of 3 in Group L. Patient satisfaction was significantly higher in Group D compared with Group L, with a P value of .005 (Table 3). The incidence of haemodynamic parameters and side effects was comparable between the groups. There was no significant difference in the frequency of adverse effects or hemodynamic metrics between the study groups.
Patient Satisfaction Scores.
Statistically significant P < .05.
Discussion
The findings of our study state that adding 4 mg of dexamethasone to levobupivacaine in ultrasound-guided ESPB significantly prolongs the duration of analgesia, reduces consumption of rescue analgesics, lowers pain scores, and better patient satisfaction when compared to levobupivacaine alone for MRM surgeries.
The drug that provides early onset of both sensory and motor block, followed by prolonged sensory block, and early offset of motor block postoperatively, would be ideal for peripheral nerve block. Since the local anaesthetic alone may not be able to prolong the analgesic effect, so it is advisable to add an adjuvant while providing regional anaesthesia and analgesia. Use of adjuvants along with local anaesthetics can also avoid problems of carrying continuous catheterisation for pain management.
Several adjuvants have been employed with local anaesthetics to extend the analgesic action in MRM surgeries with varying results. 8 Dexamethasone is the most effective and investigated of such adjuvant drugs. 9 Cochrane review suggested that low-dose dexamethasone (4-5 mg) increased block duration more than high-dose dexamethasone (8–10 mg) when comparing perineural and systemic dexamethasone. 10 Fusco et al. had also used dexamethasone in a dose of 4 mg with levobupivacaine in ESPB for laparoscopic abdominal surgery. 11 According to the literature, the lowest sufficient dose of dexamethasone added to a local anaesthetic is 4 mg for peripheral nerve blockage. Therefore, we chose a dose of 4 mg of dexamethasone for the present study while also considering the safety profile of the drug.
In our study, we found that adding 4 mg of dexamethasone to levobupivacaine provides significantly extended duration of analgesia when added to 0.25% levobupivacaine compared to levobupivacaine alone in ESPB for MRM surgeries. A study conducted by Farahat TEM et al. used 4 mg dexamethasone with levobupivacaine in ultrasound-guided ESPB for total hip arthroplasty, also showed that dexamethasone provides prolonged analgesia compared to levobupivacaine alone. 12 Previous studies have shown similar results of prolonged analgesia with dexamethasone used as an adjuvant to local anaesthetics, in different regional blocks.13–19
Dexamethasone has the appropriate anti-inflammatory property by increasing the release of anti-inflammatory substances and decreasing the release of inflammatory mediators. This feature may be responsible for its systemic mechanism that extends the block duration. 20
In a study conducted by An K et al. in a mouse sciatic nerve blockade model, it was found that perineural dexamethasone added to bupivacaine prolongs the duration of sensory blockade. 21 However, a study conducted by Gao et al. found that dexamethasone as an adjuvant with ropivacaine in an ESPB for thoracoscopy lobectomy surgery did not prolong the duration of sensory block analgesia. 22 Similarly, a study done by Marhofer et al. also states that 4 mg dexamethasone with ropivacaine at the ulnar nerve has no influence on the duration of sensory block that is clinically relevant. 23 The discrepancy might result from heterogeneous research designs including different types and concentrations of local anaesthetics, with or without vasoconstrictors, different types of surgery and differences in regional anaesthetic technique and block sites, so variation might develop when interpreting the data. 24
The present study found that the total rescue tramadol requirement was lesser in Group D as compared to Group L. Akkaya et al. used 8 mg dexamethasone with 0.25% levobupivacaine in transverses abdominis plain block (TAPB) for caesarean sections and found significantly lesser consumption of tramadol in dexamethasone group (P = .001) when compared with levobupivacaine alone group, which was in concordance with our results. 25 Our results are consistent with the meta-analysis done by Chen et al., and we found that dexamethasone as an adjuvant to TAPB significantly reduced the 24-h analgesic consumption. 26 This finding of our study is very beneficial to patients for reducing pulmonary complications, earlier mobilisation and shorter hospital stay. Tulgar S et al. used ESPB and quadratus lumborum block in combination for anaesthetic management of a high-risk patient for hemiarthroplasty. 27 They found that both the blocks in combination increased the effectiveness and complemented the missing aspects. So, it may be a good option when general and spinal anaesthesia are not safe to manage the patient.
The present study demonstrates that in the first 24 hours after surgery, VNRS scores were significantly lower in Group D as compared to Group L. Similarly, Sharma et al. found that pain scores were significantly lower in dexamethasone with ropivacaine as compared to ropivacaine only in the transverse abdominis plane block for inguinal hernia repair. 28
Regarding haemodynamic variables in our study, both groups were comparable during the perioperative period, and the results were in concordance with the previous study. 12 No participant experienced serious adverse events during the study. Similarly, Ammar et al. found no evidence of adverse events in their study. 29
Patient satisfaction was significantly higher in Group D as compared with Group L can be due to longer duration of analgesia and lesser tramadol consumption in Group D. Our results are in concordance with the previous study. 30
This limitation of the study was that we did not measure serum levels of study drugs; therefore, we were unable to determine whether the duration of the analgesic effects of dexamethasone results from a direct perineural mechanism of action or from its systemic absorption. Further clinical studies are required to determine its mechanism of action. Secondly, our study did not include ASA physical status III and IV, obese, pregnant patients and children, so our results cannot determine the effectiveness of dexamethasone as an adjuvant to ESPB in high-risk patients and children.
Conclusion
Perineural dexamethasone in a dose of 4 mg with 0.25% of levobupivacaine can prolong the duration of analgesia, reduce verbal numerical rating score (VNRS), reduce the total requirements of postoperative rescue analgesics, and improve patient satisfaction when compared to levobupivacaine alone. However, there was no difference in terms of hemodynamic parameters and postoperative complications between the groups. Therefore, administration of perineural dexamethasone in a dose of 4 mg with levobupivacaine provides adequate and prolonged analgesia while maintaining hemodynamic stability without any adverse effect in ultrasound-guided ESPB for MRM.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.