
Abstract
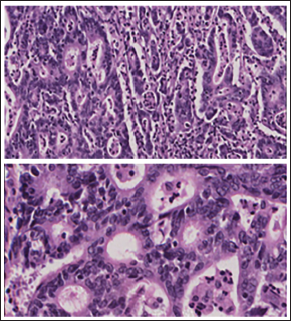
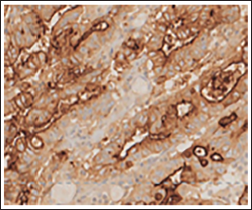
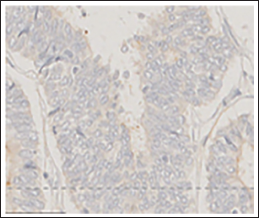
A woman in her 60s presented with complaints of postmenopausal bleeding. On ultrasonography, the endometrium was thickened and measured about 13.7 mm along with a well-defined hypogenic area on anterior cervical wall. On magnetic resonance imaging (MRI), a malignant polypoidal mass arising from the junction of the uterus and cervix with extension into the upper vagina was noted. Hence, total abdominal hysterectomy with bilateral salpingo-oophorectomy was done. On cutting the uterus, two distinct polypoidal tumors were seen in lower uterine segment and another in cervix without invasion. On micro-scopy, tumor in the cervix (Figures 1 and 2) was a moderately differentiated adenocarcinoma with complex branching glands, cords, and trabeculae. On immunohistochemistry (IHC), the tumor was positive for carcinoembryonic antigen (CEA; Figure 3) and p16, while negative for estrogen receptor (ER), Wilms’ tumor 1 (WT1), and vimentin. The tumor in the isthmus (Figures 4 and 5) was low-grade endometrioid carcinoma with back-to-back arranged glands with oval nuclei. The tumor cells expressed ER and vimentin while CEA (Figure 6) and WT1 were negative. P53 was wild type and p16 expression was mosaic type. MutL homolog 1 and postmeiotic segregation increased 2 were lost to IHC, while MSH2 and MSH6 were intact. Molecular testing for Lynch syndrome was conducted which was negative. A diagnosis of synchronous tumor was rendered. The patient received five sessions of SORBO brachytherapy (4 Gy per session). The patient is doing well on three years follow-up. Dual synchronous primary gynecological neoplasms have a low incidence rate and range from 0.6% to 5.4%.1, 2 Till date about nine cases of synchronous carcinoma cervix with carcinoma endometrium have been reported in the literature.2–4 The ovarian and endometrial cancers are most common synchronous cancers. 2 It is proposed that embryologically similar tissues, when subjected to either hormonal influences or carcinogens simultaneously, may develop synchronous neoplasms, as their etiology and pathogenesis remain unclear. 2 The synchronous tumors and the primary tumors are similar in diagnosis and treatment. 2
Tumor in Cervix Dispersed in Branching Glands, Trabeculae, and Cords 10×, 40×.
Immunohistochemistry Marker CEA Positivity in the Cervical Tumor Cells.
Isthmic Tumor Dispersed in Back-to-back Glandular Pattern 10×, 40×.

Immunohistochemistry Marker CEA Negativity in the Tumor Cells of Isthmus.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional or regional) and with the Helsinki Declaration of 1975, as revised in 2000.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
A general informed consent was taken from the patient regarding sharing of clinical data for research purpose. All the patients’ information in the manuscript was anonymized and only de-identified data was used.