
Abstract

Case Presentation
A 16-year-old girl presented with pain and swelling in right maxillary region for 2 months. There was no history of trauma or fever. Clinical examination revealed firmly fixed swelling over the right maxillary region with no redness or tenderness.
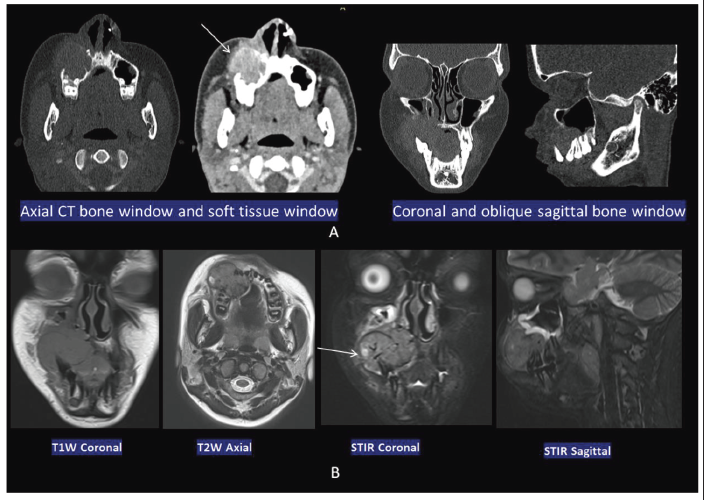
She was evaluated with contrast-enhanced computed tomography (CECT) and magnetic resonance imaging (MRI) scans. CECT revealed a well-defined expansile lytic lesion with heterogeneously enhancing soft tissue arising from the anterior maxilla on the right involving the alveolar process and the floor of maxillary sinus and reaching the midline, associated with the displacement of the teeth and buccolingual expansion with cortical erosion. Further MRI study showed expansile lobulated soft tissue with intermediate signal on T1WI, intermediate to hyperintense on T2WI, and hyperintense on short tau inversion recovery (STIR) images with a tiny cystic area. It shows mild diffusion restriction (Figure 1).
CECT Images; (A) Showing a well-defined expansile lytic lesion with heterogeneously enhancing soft tissue arising from the anterior maxilla on the right involving the alveolar process and the floor of maxillary sinus. It is associated with displacement of the teeth and buccolingual expansion with cortical erosion. MRI Images; (B) Showing expansile lobulated soft tissue with intermediate to hyperintense signal on T2WI and hyperintense on STIR images with a tiny cystic area and mild diffusion restriction.
Giant cell granuloma (GCG) Browns tumor Ameloblastoma
Subsequently, a biopsy of the lesion was performed. Hematoxylin and eosin (H&E)-stained slides demonstrated nonencapsulated aggregates of numerous foreign body giant cells admixed with inflammatory cells and fibrotic stroma. A few foci showed cystic space with a fibrocollagenous wall with areas of hemorrhage. Hemosiderin-laden histiocytes were also seen. However, there was no evidence of atypia/malignancy. On immunohistochemistry, the cells were negative for H3F3A G34W. A final diagnosis of Giant cell granuloma was made (Figure 2).
(A) Microphotograph showing nonencapsulated aggregates of foreign body giant cells in a fibrotic stroma. (B) Higher power shows numerous foreign body giant cells admixed with inflammatory cells. (C) Areas of hemorrhage and hemosiderin laden histiocytes (arrow) are also seen. (D) Immunostaining is negative for H3F3A G34W.

Giant cell granuloma (GCG) is a very rare intraosseous benign lesion but locally invasive; it preferentially occurs in the head and neck region. It involves the posterior mandible more than the anterior mandible, followed by the maxilla. It is associated with local trauma, inflammatory process, or repair process. GCG usually occurs in young women in the second or third decade of life.1, 2 Common clinical features of GCG are pain, swelling, or palpable bony lesions. Most often, GCG appears as a slowly growing mass. 2 Histologically, GCG showed osteoclast-like giant cells in a hypercellular fibrous stroma with hemorrhagic areas or cystic degenerative foci or osteoid production. 3 The histologic features of GCG, giant cell tumor, and brown tumor of hyperparathyroidism are usually similar to granulomas with immunohistochemical staining positive for cluster differentiation 68 (CD68) 68. 3 On radiography, a well-defined radiolucent multilocular (less often unilocular) lesion is usually appreciated. However, in some cases, expansion of bone or displacement/resorption of teeth is also seen. On CECT, aggressive lesions usually show a circumscribed expansile heterogeneous mass with bone remodeling and lytic destruction. A homogeneous or slight heterogeneous intermediate signal on T2 and STIR images is seen on MRI with contrast enhancement.2–4 T2 shortening is usually consistent with hemorrhage and giant cells in the lesion. 1
Benign but locally aggressive odontogenic tumor; occurs in fourth to sixth decades of life. The typical location is the body and ramus of the posterior mandible. Radiography reveals a unilocular/multilocular radiolucent lesion and a cortical breach, root resorption/soft-tissue extension in the aggressive lesion. The septations within the lesion give soap bubble appearance.
1
Enhancement with diffusion restriction of solid components on CT and MRI.
Focal bony lesions because of bone remodeling from either primary or secondary hyperparathyroidism. More common in women than men; occurs in the fifth to sixth decades of life. Single or multiple well-defined osteolytic expansile lesions, associated with bony destruction, pathological fractures, or adjacent soft tissue involvement. Parathyroid hormone, serum and urinary levels of calcium, phosphate and bone or serum alkaline phosphatase help in diagnosis.
Typical slow-growing lesions can be treated with conservative methods such as intralesional steroid injection, calcitonin injections, and radiotherapy.1, 5 Subcutaneous denosumab injection—monoclonal antibody against the receptor activator of nuclear factor-κB (RANK) ligand now considered as successful treatment for GCG.
6
Enucleation and curettage is definitive treatment with surgical resection in aggressive cases.1, 5
Conclusion
Giant cell granuloma is a very rare locally invasive benign lesion. Imaging helps in the evaluation of the extent and involvements of the lesion and determines its aggressiveness. Definitive diagnosis is made by histopathology and immunohistochemical analysis. Early diagnosis and treatment is required for better outcome and results in aggressive lesions.
Footnotes
Acknowledgements
We thank the patients and their families for their munificence in contributing to this study. We would also like to thank all members of the IRB committee who gave their approval for this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.