
Abstract
Cancer patients experience a decrease in blood counts either due to the myelosuppressive effect of oncological treatment or bone marrow infiltration due to distant metastases. Oncological interventions, such as chemotherapy, immunotherapy or large-field irradiation, are common causes of neutropenia, thrombocytopenia, or pancytopenia in cancer patients. Non-oncological reasons for the decrease in blood counts can be attributed to drug-induced, autoimmune diseases, or viral infections. Recently, case reports have been published for neutropenia/thrombocytopenia due to the Coronavirus disease (Covid-19) pandemic too. Here, we discuss a case of phenytoin-induced neutropenia in a brain tumor patient and a pragmatic approach for managing unexplained neutropenia, that is, neutropenia unrelated to cancer or oncological intervention. Timely recognition and timely intervention can prevent fatal outcomes.
Keywords
Introduction
Non-metastatic cancer patients usually experience neutropenia/thrombocytopenia or pancytopenia due to the myelosuppressive effect of chemotherapy or immunotherapy or large field irradiation, such as craniospinal irradiation or whole pelvis.1, 2 Other non-oncological causes of decrease in blood counts can be drug-induced, autoimmune diseases, or viral infections. 3 Here, we discuss a pragmatic approach for managing unexplained neutropenia, that is, neutropenia unrelated to cancer or oncological treatment. Timely recognition and timely intervention can prevent fatal outcomes.
Case Presentation
Twenty-nine-year-old male with history of recent onset seizures was diagnosed with a space-occupying lesion in the right frontal lobe on magnetic resonance imaging. He underwent right frontal craniotomy and gross total excision of the lesion. Postoperative histopathology was suggestive of isocitrate dehydrogenase mutant, anaplastic astrocytoma, World Health Organization (WHO) Grade 3. Post-operatively he was continued on maintenance antiepileptic drug phenytoin at a dose of 100 mg, 3 times a day. Four weeks later, he was started on adjuvant radiation treatment only with 60 Gray/30 fractions/6 weeks. As per the second interim analysis report of the Concurrent and Adjuvant Temozolomide Chemotherapy in Non-1p/19q Deleted Anaplastic Glioma (CATNON) trial, patient was planned for adjuvant chemotherapy with temozolomide only after radiation completion, concurrent chemotherapy deferred as this was not beneficial, as per the results of this trial. 4
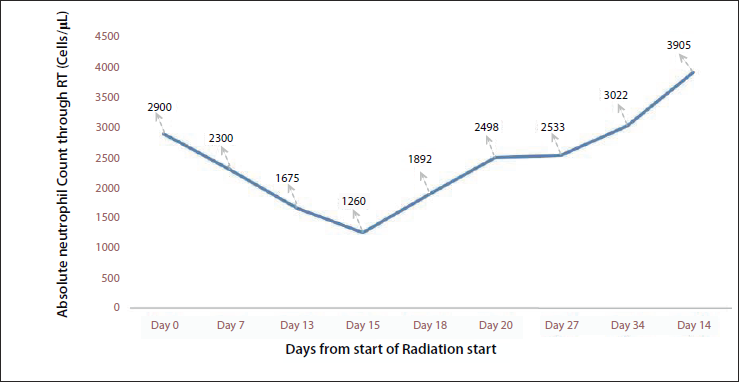
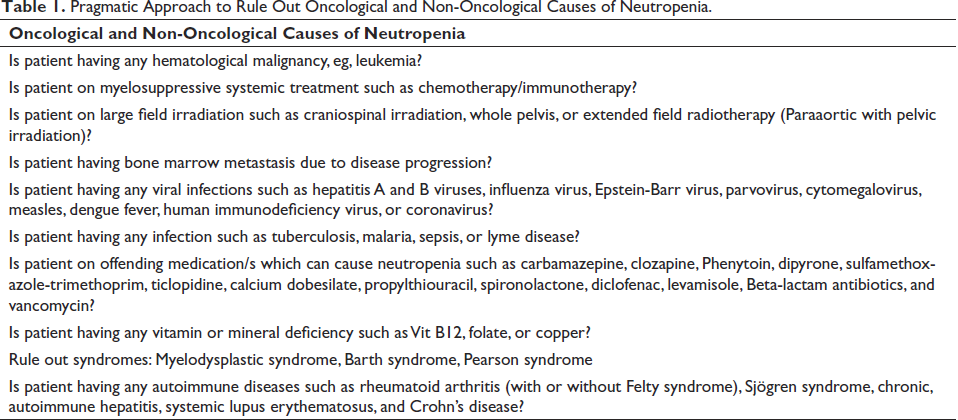
During the first 2 weeks of clinical and hematological review, it was observed that his neutrophil counts were following a decreasing trend. Clinically patient was asymptomatic. As the neutrophil count declined to more than half from the baseline and the counts were below normal on day 15 (Figure 1), we started working on various differential diagnoses of neutropenia, as listed in Table 1.
Absolute Neutrophil Count During Adjuvant Radiation Treatment.
Pragmatic Approach to Rule Out Oncological and Non-Oncological Causes of Neutropenia.
The patient had a non-metastatic brain tumor which is unlikely to cause a decrease in blood counts. The irradiation field was limited to the skull, constituting less than 3% of total bone marrow 5 ; this also precluded radiation-induced bone marrow suppression. He had not received any myelosuppressive drugs previously or concurrently with radiation. Recently many case reports were published for neutropenia and thrombocytopenia attributed to the Covid-19 pandemic. 6 Covid-19 polymerase chain reaction testing, for our patient was reported as negative.
The patient had no other symptoms or signs suggestive of viral infections, autoimmune disease, or vitamin B12/folate deficiency. His peripheral smear did not suggest any morphological abnormalities of hematopoietic cells. Antiepileptics can rarely cause neutropenia or pancytopenia, as reported in the literature. 7 With a provisional diagnosis of phenytoin-induced neutropenia, and on the neurologist’s opinion, Day 15 onwards the patient was gradually weaned off phenytoin and started on levetiracetam simultaneously.
After weaning off the offending drug on day 18 of radiotherapy—total leukocyte count and absolute neutrophil count, started rising, as shown in Figure 1. He was monitored for further fall/improvement in blood cell counts throughout radiation treatment. At the time of completion of radiation, the patient was on levetiracetam 500 mg thrice a day and had reported no seizure episodes nor had further fall in blood cell counts. At the time of reporting this case report—he had completed four cycles of adjuvant chemotherapy with temozolomide without any significant decrease in blood counts.
We evaluated the incident as per the adverse drug reaction probability scale, developed in 1991 by Naranjo et al. 8 We did not perform the rechallenge test with phenytoin as an alternative drug, that is, Levetiracetam was available. We did not keep the patient on placebo as antiepileptic treatment was mandatory to prevent any undue delay in ongoing oncological treatment. Our case received a Naranjo score of 8, suggesting possible causality for phenytoin being the cause of neutropenia, as shown in Table 2.
Naranjo Adverse Drug Reaction Probability Scale.
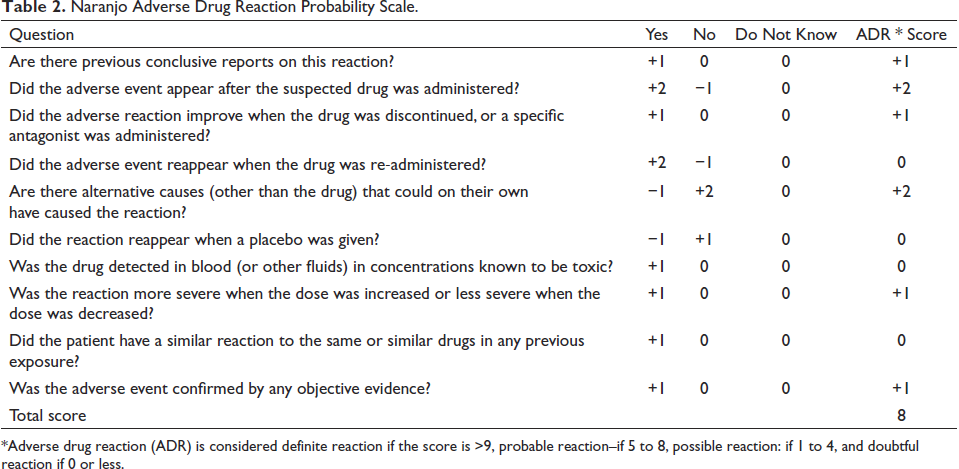
*Adverse drug reaction (ADR) is considered definite reaction if the score is >9, probable reaction–if 5 to 8, possible reaction: if 1 to 4, and doubtful reaction if 0 or less.
Discussion
Phenytoin is one of the most used, cheapest, and readily available drugs for preventing and controlling seizures, especially in a resource-limited setting like India. It is a non-specific sodium channel blocker that prevents seizures by inhibiting the positive feedback and limiting the repetitive neuronal firing. 9 Hematological dyscrasias have been reported in association with phenytoin consumption, including agranulocytosis, megaloblastic anemia, macrocytosis and in some cases, pancytopenia. Agranulocytosis reported after phenytoin usage has an incidence of less than 1%. Other drugs most associated with non-chemotherapy drug-induced neutropenia (DIN) are carbimazole, clozapine, dapsone, dipyrone, methimazole, penicillin G, procainamide, propylthiouracil, sulfasalazine, and ticlopidine. 10
The proposed mechanisms for DIN are either a reactive metabolite-mediated injury to neutrophils or a drug-induced immune allergy reaction. Phenytoin is chlorinated by the myeloperoxidase/H2O2/Cl-system to N, N’-dichlorophenytoin that causes covalent binding to activated neutrophils. Other less likely mechanisms include drug-antibody immune complex binding to the target neutrophils and causing destruction, and phenytoin acting as a hapten to induce an immune response against neutrophils by binding to the cell’s surface. 7 We did not elicit whether it was metabolite-mediated injury or drug-induced immune reaction in view of unavailability of anti-granulocyte antibody tests or other complex lab assays. However, on the Naranjo scale, with a score of8—the case fits in possible phenytoin-induced adverse drug reaction.
The time taken by phenytoin to induce marrow suppression is around 19–60 days, and our patient developed neutropenia in the same time range. His counts normalized after weaning off the causative drug and replacing it with another antiepileptic drug, levetiracetam.
Conclusion
If common causes of neutropenia, such as chemotherapy, large field irradiation, or viral causes, are absent then the next step should be to identify any offending drug present in the patient’s prescription. If so, it will be cost-effective to wean off or stop the offending drug and prevent unnecessary investigations. If left untreated, approximately 5% of drug-induced agranulocytosis can be fatal. Phenytoin is the commonly used anticonvulsant; it becomes mandatory to understand and identify the adverse effects it causes.
Timely recognition and intervention can prevent drastic consequences on a patient’s health, especially in patients with cancers where neutropenia and thrombocytopenia could lead to oncological treatment interruption and detrimental clinical outcomes. Therefore, it is advisable to be vigilant with weekly monitoring of clinical, hematological, and biochemical parameters in patients receiving radiation therapy to improve patient management.
Contributions
Narendhar Gokulanathan: Acquisition of data, conceptualization, and literature review.
Pooja Sethi: Drafting and review of manuscript.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement
The manuscript has been read and approved by all the authors and each author believes that the manuscript represents honest work.