
Abstract
Primary testicular lymphoma (PTL) is a rare variant of non-Hodgkin’s lymphoma that is predominant in old age group. Painless testicular swelling is the most common presentation. The standard of care is surgery in the form of radical orchiectomy followed by adjuvant chemotherapy and central nervous system prophylaxis. Because of blood-testis barrier, contralateral testis acts as a sanctuary site for chemotherapy to act and hence scrototesticular radiation is advocated in order to reduce the chance of testicular relapse. Due to lack of any consensus simulation procedure, we propose here a step-by-step procedure for simulation of a case of PTL using a case scenario.
Introduction
Primary testicular lymphoma (PTL) is a rare extra-nodal lymphoma that accounts for 1% to 2% of all non-Hodgkin’s lymphoma and around 9% of all testicular malignancies. It is predominantly seen in elderly age group with a median age of diagnosis being 60 years.1–3 The patient usually presents as a painless testicular mass that develops over days to months. It has propensity to disseminate to other extra nodal sites such as central nervous system, skin, lungs, and even contralateral testis. 4 The patients undergo inguinal orchiectomy that acts both as diagnostic and therapeutic purpose. The most common histology being diffuse large B-cell lymphoma accounting for 80% to 90% followed by Burkitt’s lymphoma and T-cell lymphoma.
The standard of care now is unilateral radical orchiectomy followed by adjuvant doxorubicin-based chemotherapy plus Rituximab if CD-20 is positive. In addition, intrathecal methotrexate is added for CNS prophylaxis. As the contralateral testis acts as a sanctuary site for chemotherapy to act because of blood-testis barrier and there is 15% to 45% risk of relapse in the contralateral testis, scrototesticular irradiation following chemotherapy is of paramount importance. 5 In the absence of any randomized control trials, an observational study found that testicular radiation can reduce the relapse in contralateral testis to less than 10% from 42%.6, 7 The International Extranodal Lymphoma Study Group (IELSG), a retrospective study on PTL, has shown that testicular radiations have increased the 5-year progression-free survival from 36%to 70% and overall survival from 38% to 66%.1, 7
In this article, we provide a detailed guide in simulating the scrotum for testicular irradiation in PTL that is explained here with the help of a case scenario.
Method
Case History
A 56-year-old male presented with painless swelling over the left scrotum since 2 months. The patient underwent left orchiectomy. The postoperative histopathology report was suggestive of PTL. Patient showed complete response after receiving 8 cycles of R-CHOP chemotherapy regimen and 2 cycles of intrathecal methotrexate for CNS prophylaxis. Now the patient planned for consolidative radiotherapy to scrotum and contralateral testis.
Radiotherapy Dose
Fractionated consolidative radiotherapy was planned to the whole of scrotum including postop tumor bed, contralateral testis, tunica albuginea, epididymis, and rete testis to a total dose of 30Gy in 15 fractions @ 2Gy per fraction as per IELSG and International Lymphoma Radiation Oncology Group (ILROG) guidelines.1, 8
Radiotherapy Simulation Technique
The detailed process of simulation of patient for scrototesticular radiation is summarized below in a step-by-step manner.
Step 1:
Patient was positioned in supine with frog leg position. A pelvic immobilization mask (Orfit) is prepared in this position (Figure 1A).
Depicts the 7-Step Simulation Procedure for Scrototesticular Irradiation.
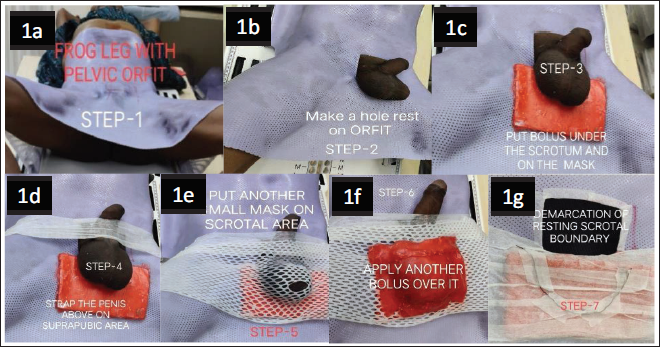
Step 2:
A hole was made in this mask around the penile region and the scrotum along with the contralateral testis was pulled out through this hole and made to rest on the mask (Figure 1B).
Step 3:
The posterior aspect of the scrotum was supported with a wax bolus to prevent under dosing to scrotum and testis (Figure 1C).
Step 4:
The penis was moved outside of the irradiation field by fixing it to the abdominal wall by the help of a tape (Figure 1D).
Step 5:
Now a small second mask was made over the previously prepared pelvic mask to stabilize the scrotum in position (Figure 1E).
Step 6:
Second bolus was made over the superior aspect of the second mask (Figure 1F).
Step 7:
A copper wire was used to demarcate the scrotal position over the second mask that can be seen in computed tomography (CT) scan so that we need not miss the target (Figure 1G).
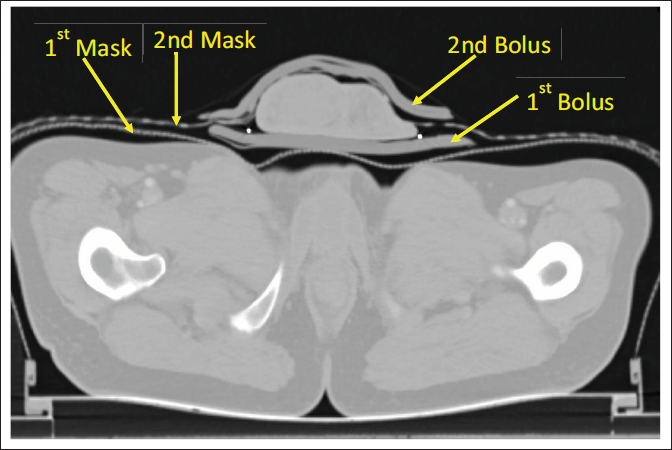
Planning CT Scan
A planning CT scan from xiphisternum to mid-thigh is taken with 3 mm slice thickness with and without contrast with hands over the chest. Both the immobilization mask and bolus can be seen in Figure 2.
Shows Both the Immobilization Mask and Both the Bolus During CT Simulation.
Target Delineation
CT images are transferred to treatment planning system for delineation of target volume. There is no gross tumor volume as it has been removed surgically. Clinical target volume includes contralateral testis, epididimys, and spermatic cord. Planning target volume (PTV) is institution specific.
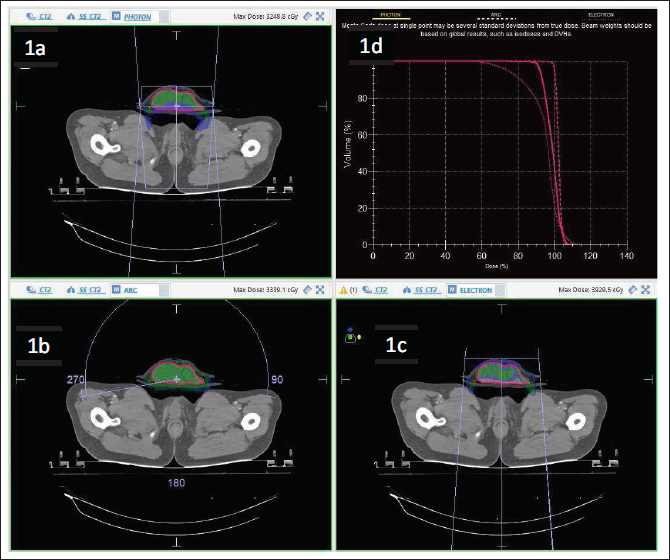
Treatment Planning
The treatment planning was done by using 6MV photon, ARC technique, and electron beams using anteroposterior portals (Figure 3A-C). The dose-volume histogram in Figure 3D gives a comparative study of all the 3 plans and it was seen that the coverage of PTV was better with the ARC therapy. So, the present case was treated using this ARC technique.
Shows the Treatment Plans in the Present Case by 6MV Photon (A), ARC Technique (B), and Electron (C) While the Dose-Volume Histogram of All the 3 Plans (D).
Discussion
Till date, there is no consensus simulation or planning technique for scrototesticular irradiation for PTL. This is due to the fact that PTL is very rare and there are only small retrospective studies which have used PTL irradiation. Here, in this article we have tried to explain one such simulation planning of PTL scrototesticular irradiation.
Conclusion
This article highlights the simulation planning of scrototesticular irradiation in detail which will act a guide for all radiation oncologist for scrotal irradiation in PTL.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Ethical Approval and Informed Consent
Necessary ethical clearances and informed consent were received and obtained respectively before initiating the study from all participants.