
Abstract
Malignant peripheral nerve sheath tumor (MPNST) is a rare tumor of oral cavity. Tongue is an extremely rare site for MPNST. We present a rare case of MPNST of tongue in a 34-year-old male. Presentation remains same as carcinoma of tongue but histopathology and immunohistochemistry help to establish the diagnosis. Biopsy of lesion was suggestive of malignant spindle cell neoplasm. On immunohistochemical examination, tumor cells were immunopositive for vimentin and S100 and SMA. Patient underwent surgery followed by adjuvant radiotherapy in order to reduce the risk of recurrence.
Introduction
Malignant peripheral nerve sheath tumor (MPNST) is a rare tumor that accounts for 5% to 10% of all soft tissue sarcomas. It comprises 6% to 16% of head and neck sarcomas. 1 Almost half of the MPNST cases are associated with neurofibromatosis type-1. 2 Median age at diagnosis is 30 to 50 years. Males and females are equally affected. 3 MPNST of tongue is extremely rare. Till date, only few cases have been reported in literature. Herein, we report a case of MPNST of tongue in a 34-year-old male.
Case Report
A 34-year male, chronic smoker and tobacco chewer developed an ulcer over the right lateral border of tongue 15 days back. Contrast enhanced computed tomography (CECT) scan of the neck and chest revealed ulceroproliferative lesion in the middle third of the tongue on the right side extending up to the midline, size of the lesion was 4.6 cm × 2.6 cm × 3.7 cm. Metastatic workup in form of CECT chest was normal. Punch biopsy from lesion was suggestive of malignant spindle cell neoplasm. In view of tumor size and aggressive behavior, patient underwent right hemiglossectomy with more than 1 cm margins along with modified radical neck dissection type III preserving spinal accessory nerve, internal jugular vein, and sternocleidomastoid muscle.
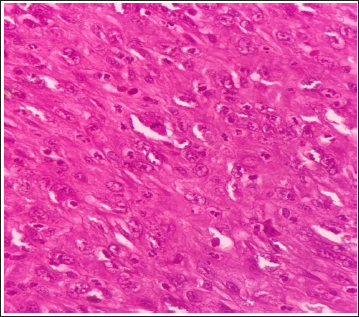
Histopathological examination of specimen showed presence of tumor cells arranged in sheets and fascicles. Cells were spindle in shape with irregularly clumped chromatin and prominent nucleoli (Figure 1). Mitotic activity was high (15-18 per 10 high power fields). Areas of necrosis were present. All resected margins were free of the tumor. Twenty-five lymph nodes were identified all of which showed reactive hyperplasia.
H/E 400X, Spindle Cells in Sheets.
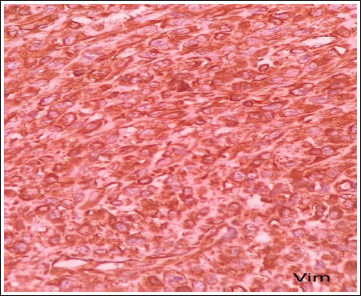
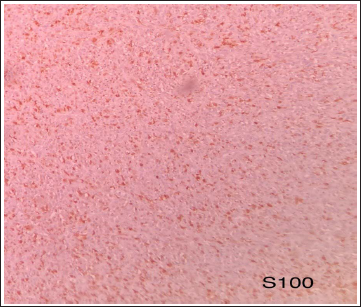
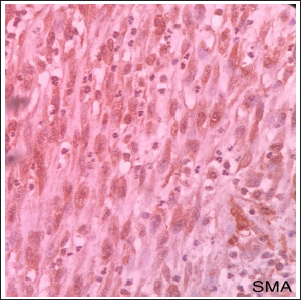
On immunohistochemical examination (IHC), tumor cells were immunopositive for vimentin (Figure 2) and S100 (patchy positive) (Figure 3) and SMA (patchy positive) (Figure 4) and were immunonegative for CD 34, Caldesmon, Desmin, TLE 1, HMB 45, Pan CK, and p53. On morphology and IHC, final diagnosis was made as MPNST.
IHC 400X, Vimentin Showing Diffuse Cytoplasmic Positivity.
IHC 100X, S100p Showing Patchy Cytoplasmic and Nuclear Positivity.
IHC 400X, SMA Showing Patchy Positivity.
Reconstruction was done using radial free flap. Postoperative course of the patient was uneventful with good functional outcome. Patient was treated with adjuvant radiotherapy after surgery.
Discussion
MPNST is a highly aggressive rare tumor. Overall incidence of MPNST is 4% to 10% of all soft tissue sarcomas. Majority of tumors occurs at extremities and trunk. It is extremely rare in oral cavity. Head and neck region are involved in about 8% to 14% cases. In head and neck, commonly involved sites are scalp and face, sinonasal tract, base of skull, upper aerodigestive tract, parotid, and neck. In oral cavity, commonly involved sites are lips, buccal mucosa, and mandible. Tongue is extremely rare site for MPNST. In our patient, the primary site was tongue and it was a nonmetastatic disease.
On histopathology, marbling is identified (alternating areas of hypocellularity and hypercellularity) with perivascular accentuation. Heterologous differentiation is present in 10% to 15% of cases MPNST.
They are divided into low grade and high grade on the basis of mitotic activity and necrosis.
Immunohistochemical antibodies like S100 and SOX10 are usually patchy or focal and only seen in up to 50% of cases. Although S100 expression is not exclusive of MPNST, it is indicative of the neural differentiation. Desmin, myogenin, and MyoD1 may be seen in rhabdomyosarcomatous elements. Molecular basis of these sarcomas is cytogenetically complex like inactivating mutations in CDKN2A/CDKN2B and PRC2 and NF1 mutations in the setting of NF. Point mutations may be seen in BRAF V600 in a subset of cases.4, 5
The mainstay of treatment of nonmetastatic MPNST is surgery. Incidence of lymphatic invasion is very less so prophylactic neck dissection is not advised. 6 The involved nerve should also be resected. After surgery, radiotherapy is given to prevent the recurrence. Role of chemotherapy is controversial in MPNST.
MPNST of head and neck region has poor prognosis. In reported cases, the 5-year survival rate ranges from 15% to 65%. 7 In a multivariate analysis, cellular differentiation and tumor grade were found as independent adverse prognostic factors for disease free survival and overall survival, retrospectively. 8 High Ki-67 labelling index is also associated with poor survival. Most common site of metastasis is lung and outcome in patients with metastatic disease is very poor.
Conclusion
MPNST of the tongue is an extremely rare entity. It should be kept a rare differential in a patient presenting with an oral cavity mass. As they are very rare tumors, there is no standard guideline for their management. Surgery with negative margins is the treatment of choice for nonmetastatic disease. Radiotherapy should be considered to reduce the risk of recurrence.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
It is a case report. Ethics committee approval not required. We have not disclosed identity of the patient in form of name initial, or photos.