
Abstract
Background:
Cannabis use among older persons has been increasing relative to younger populations, and persons over 50 years old are more likely to use cannabis for age-related therapeutic purposes. We suspected that spouses, adult children, and other older informal care partners (ICPs) of older adults are using cannabis as a form of self-care to address physical and/or mental health needs.
Objectives:
We described ICPs over 50 years old who used cannabis in the past year, contrasted them with those who did not, and determined if cannabis use was associated with health care service use.
Research Design and Methods:
We obtained 2019 California Health Interview Survey (CHIS) public use files and linked base survey responses with caregiving and cannabis questions answered by 9,984 Californians aged 50 and over. We used survey data to measure background characteristics, health behaviors, physical health status, psychological status, caregiving characteristics, and cannabis use. We differentiated among older ICPs using logistic and multivariate regression models.
Results:
We identified a total of 2,802 (28.1%) CHIS respondents over 50 who provided care to an older adult. ICPs were more likely to have used cannabis in the past year compared with noncaregivers (odds ratio [OR] 1.4; confidence interval [CI]: 1.2, 1.7). When compared with those ICPs who did not use, we did not observe differences in self-reported physical distress but found cannabis users were more likely to report being diagnosed with asthma (OR 2.0; CI: 1.2, 3.2) and diabetes (OR 1.80; CI: 1.1, 3.0). ICPs who used cannabis also were more likely to report feeling nervous (OR 2.1; CI: 1.3, 3.8). ICPs who provided care to someone with Alzheimer’s disease or a related dementia (ADRD) were more likely to use cannabis (OR 1.50; CI: 1.1, 2.0).
Discussion:
Nearly one out of every three older Californians including those who serve as ICPs used cannabis in the past year. We found older ICPs were more likely to use than non-ICPs, especially if they were providing care to someone with ADRD. Given the demand currently placed on spouses and adult children over 50 years old to assume care for an older adult in need, further research should determine if cannabis serves as a benefit or harm.
As the population continues to grow older, the increasing number of aging Americans who require daily assistance, medical care, and long-term supportive services (LTSSs) continues to outpace the supply of formal (i.e., paid) care providers.1,2 When elevated to the population level, the need to provide ongoing care to aging Americans experiencing daily limitations has placed extensive burden on the health care and LTSS systems, 3 and this large and growing gap between demand and supply of paid formal care providers has devolved into a public health calamity. 4 Meanwhile, the provision of daily care to older persons increasingly has been left to unpaid informal care partners (ICPs); the majority of whom are spouses and adult children over 50 years old. 5
In 2020, approximately 18.0 million Americans provided informal care to one or more of the 9.0 million persons over the age of 65 who were residing in their own homes and needing daily assistance, offering an average of more than 10 h of support on a weekly basis. 5 More than 33.0% of these ICPs were a spouse or significant partner, and slightly more that 50.0% were identified as adult children over the age of 50. About 12 million of these Americans provided informal care to persons living with Alzheimer’s disease or a related dementia (PLwD), and approximately 8.0 million persons over 50 provided care for someone on a daily basis for more than 8 h. 6 Older ICPs, especially adult children, rarely plan on assuming this role, they largely are untrained and uncompensated, and many experience a change in paid employment.3,7 Researchers have identified significant physical health consequences among older ICPs including exacerbated chronic conditions, pain, and exhaustion.8,9 Relative to noncaregivers, ICPs also report higher rates of psychological distress, depression, and nervousness. 10 As the amount of time and duration of providing care escalates especially for those providing care to PLwD, ICPs experience increasing physical burden and psychological distress and are more likely to bring care recipients to emergency rooms and residential care facilities for relief, adding to the already overstretched health care and LTSS system.11,12
Despite the availability of evidence-based pharmaceutical and nonpharmaceutical interventions, few ICPs access these resources for support and relief.13,14 When they do, ICPs report benefits often are short-lived.15,16 Meanwhile, some researchers have identified a number of ways that “self-care” activities can be used to ameliorate health conditions and reduce psychological symptoms among ICPs. These include exercise, yoga, and other forms of complementary alternative medicine. 3 Other researchers have observed how cannabis increasingly has been identified as a form of self-care among older ICPs. A survey of 139 adults aged 60 and over indicated that older Coloradans who identified as a primary ICP were more likely to use cannabis than older adults who were not involved in caregiving. 17 ICPs who used cannabis also were more likely to report improved symptoms (e.g., pain and sleep) and quality of life than ICPs who did not use cannabis. 18 In California, interviews conducted with 26 ICPs recruited from the University of Southern California Rancho Los Amigos California Alzheimer’s Disease Center revealed higher rates of cannabis use than might be expected (19.2%) and these individuals reported using cannabis to relieve both physical burden and psychological distress. 19 We know little else about the ways ICPs are using cannabis as a form of self-care. The relationships among physical health, mental health, caregiving, and cannabis use are depicted in Figure 1.
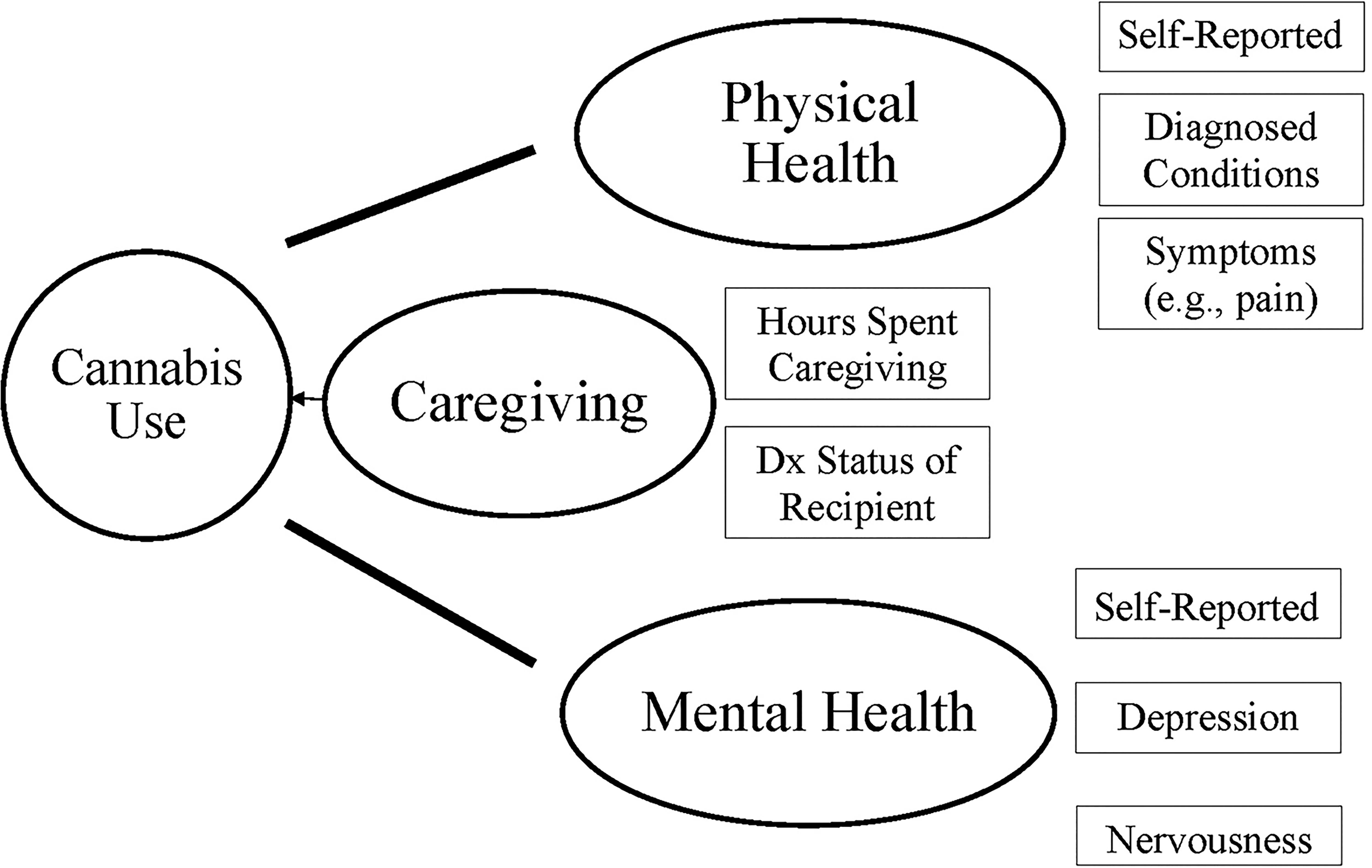
Determinants of cannabis use among informal care partners.
The California Health Interview Survey
The California Health Interview Survey (CHIS) offers the opportunity to observe a large number of ICPs who use cannabis and offers data needed to examine a range of drivers and outcomes. 20 In this study, we used the CHIS to identify ICPs aged 50 and older who provided care to someone aged 50 and older. We focused on the aging ICP population as previous research has shown spouses and adult children, who account for more than 8 of every 10 ICPs, are more likely to be engaged in caregiving tasks compared with those under 50, are more likely to live with the care recipient, and are more likely to report burden and stress than younger caregivers. 5 As such, we suspect the impact of cannabis on caregiving-related outcomes may be more pronounced with an older ICP population. In particular, we suspect ICPs are more likely to use cannabis to address symptoms associated with diagnosed health conditions (e.g., arthritis), alleviate pain, and manage other physical symptoms associated with caregiving.21,22 ICPs also may be more likely to use cannabis as a coping mechanism for psychological distress, depression, or nervousness. 23 Besides identifying possible physical and psychological correlates of cannabis use, the CHIS survey data allow us to examine how the nature of caregiving itself may contribute to cannabis use as we suspect cannabis use may be higher among those who provide care to someone with a persistent illness presenting cognitive and behavioral symptoms such as Alzheimer’s disease or a related dementia.7,8 In addition, the CHIS survey data allow us to examine if cannabis use is associated with health services use,23–25 including outpatient medical care emergency department visit access to case management or need for other health care or LTSS.
Research Objectives
Using the 2019 CHIS data, we (1) described persons over 50 years old who self-identified as ICPs and distinguished them from those older persons who were not involved with unpaid informal caregiving, (2) examined associations between caregiving and cannabis use by contrasting ICPs who used cannabis in the past year with those who did not, and tested whether health status, psychological distress, or the nature of caregiving affect these associations, and (3c) determined if ICPs who used cannabis were more or less likely to report visiting an emergency department or an outpatient medical clinic in the past year compared with ICPs who did not use cannabis, and we also examined their use of case management and need for other services. In particular, we tested six hypotheses: Cannabis use among ICPs is associated with physical distress. Cannabis use among ICPs is associated with psychological distress. Cannabis use among ICPs is associated with total time spent caregiving. Cannabis use among ICPs is associated with increased outpatient medical care. Cannabis use among ICPs is associated with increased emergency room use. Cannabis use among ICPs is associated with delays in self-care.
Methods
We obtained the public use file for the 2019 CHIS and linked base survey responses with supplemental questions about caregiving and cannabis use answered by 22,160 Californians over the age of 18. After excluding those who were under 50 years of age and those with missing information on caregiving or cannabis use, our analytical sample consisted of 9,984 late middle age and older individuals from all 58 California counties. This study was not qualified as human subjects research by the University of Iowa Institutional Review Board.
Data and variables
The CHIS is an internationally recognized representative panel survey of Californians over 18 years old that has been shown to collect reliable and valid self-reported data since 2001 covering a range of topics including demographics, health behaviors, physical health, mental health, as well as health care and LTSS use. 20 We used survey data to measure individual background characteristics (e.g., age, gender, education, employment, marital status, race, and insurance status) as well as health behaviors potentially associated with informal caregiving or cannabis use (e.g., smoking and illicit drug use). We measured physical health status using a self-reported measure of physical distress as well as diagnosed health conditions including asthma, diabetes, high blood pressure, and heart disease. Psychological status was measured by self-reported symptoms of distress, depression, and nervousness.
Cannabis use questions were embedded in the survey section concerning health behaviors and asked if the individual used marijuana or hashish in the past year. Prevalence of cannabis use was based on an affirmative response to the question “Did you use marijuana or hashish in the past year?”
The CHIS identified ICPs by asking survey respondents if they provided care to a family member or friend in the past year. Self-identified ICPs then answered questions about the total number of hours spent caregiving in the past week, the nature of the care recipient condition (e.g., Alzheimer’s, arthritis, back problems, cancer, lung disease, etc.), and symptoms related to caregiving including physical well-being and psychological distress. For the analysis, we separated ICPs who provided care to someone with diagnosed medical conditions and physical limitations relative to ongoing impairments (e.g., dementia) that persist over a sustained period of time. More information on outcome variables, predictor variables, and covariates is included as Supplementary Table S1.
Analyses
We explored the unadjusted differences between older caregivers and noncaregivers. We used logistic regression model to explore the association between caregiving and past year cannabis use while adjusting for the covariates. For further analyses, we limited our analytical sample to the subgroup of older ICPs. We used logistic regression model to analyze the associations between the nature of caregiving (hours of caregiving and whether the care recipient had Alzheimer’s disease or a related dementia [ADRD]) and cannabis use. Finally, we explored if cannabis use was associated with health care use (emergency department [ED] visits and outpatient physician visits), care coordination, and delays in seeking health care using regression models. We used logistic regression models for binary outcomes and ordinary least squared model for continuous outcome (number of doctor visits). All analyses were performed using Stata version 17.
Results
Using the 2019 survey results, we identified 9,984 respondents over the age of 50. Among these, 2,802 (28.1%) indicated they provided care to someone over 50 years old in the past year. Nearly half of these ICPs were between 50 and 64 years (48.2%) and more likely to be younger than noncaregivers (p < 0.001). Six of every 10 ICPs identified as female. ICPs also were more likely to be college educated (61.6% vs 51.9%) and employed (43.8% vs 37.3%). Older caregivers were less likely to report being in physical distress than noncaregivers or experience diabetes, high blood pressure, or heart disease. We also observed ICPs were more likely to report feelings of distress (7.2% vs 4.3%), depression (9.5% vs 5.8%), and nervousness (7.0% vs 3.8%) than noncaregivers, and they also experienced delays in accessing health care (16.7% vs 9.7%). ICPs provided an average of 16.2 h of care each week (standard deviation [SD], 22.2); 23.3% provided care to someone with ADRD and another 10% provided care to someone diagnosed with cancer.
Nearly 30% of all the adults over aged 50 included in our analytical sample used cannabis in the past year, and cannabis use was higher among older ICPs when compared with noncaregivers (36.3% vs 28.3%). These descriptive statistics are presented in Table 1.
Descriptive Statistics
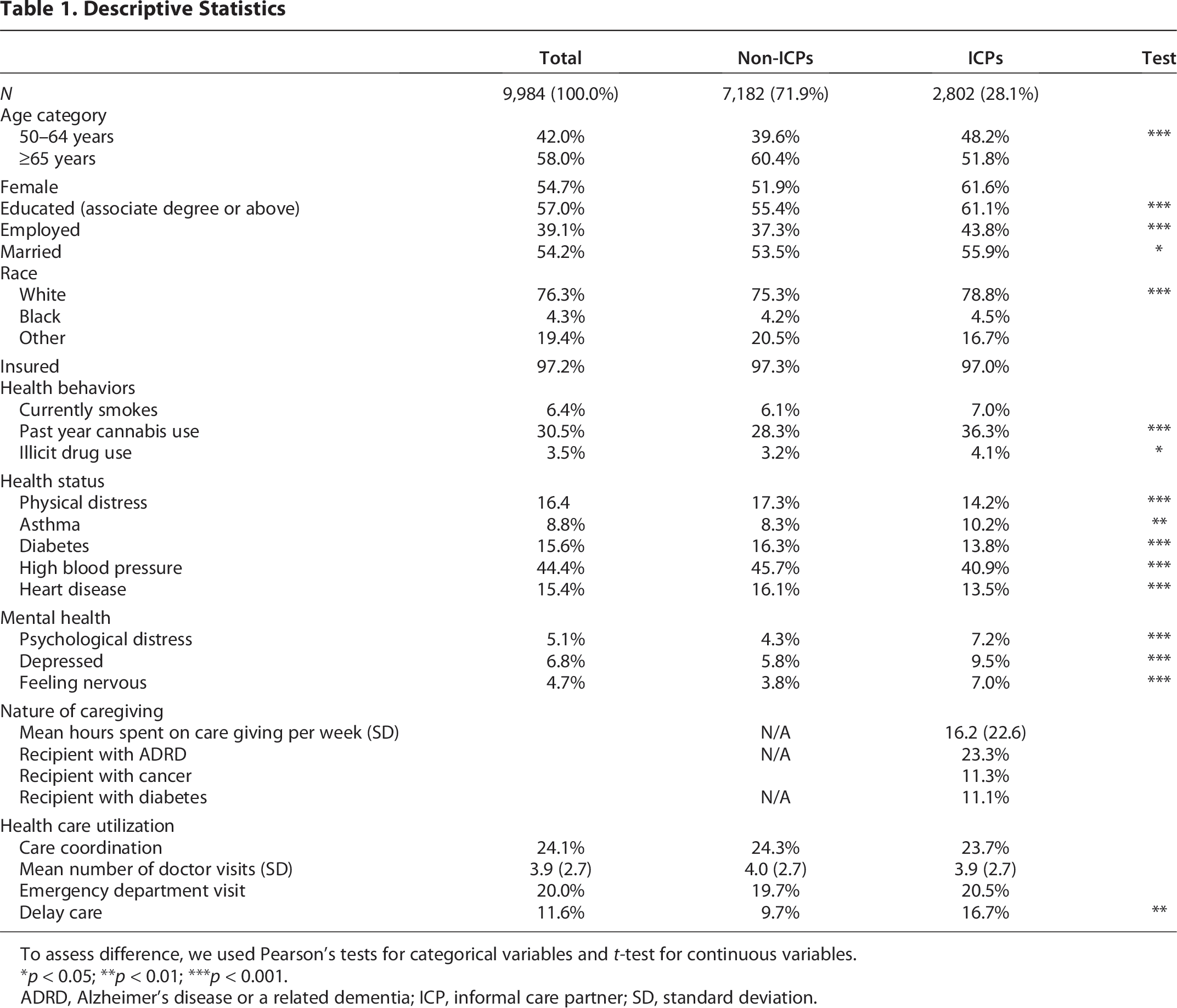
To assess difference, we used Pearson’s tests for categorical variables and t-test for continuous variables.
*p < 0.05; **p < 0.01; ***p < 0.001.
ADRD, Alzheimer’s disease or a related dementia; ICP, informal care partner; SD, standard deviation.
Table 2 shows the results of logistic regression model exploring the association between cannabis use and caregiving status. ICPs have statistically significant higher odds of cannabis use than older adults who were not involved in caregiving (odds ratio [OR]: 1.4; confidence interval [CI]: 1.2, 1.7). Older cannabis users also were younger (OR: 0.70; CI: 0.6, 0.8), more educated (OR: 1.7; CI: 1.4, 2.0), more likely to be smokers (OR: 3.2; CI: 2.3, 4.5), and have a history of illicit drug use (OR: 1.7; CI: 1.1, 2.8). Older cannabis users also were more likely to be diagnosed with asthma (OR: 1.6; CI: 1.2, 2.1) or diabetes (OR: 1.6; CI: 1.3, 2.0) and report feelings of being nervous (OR: 2.0; CI: 1.4, 2.9).
Multivariate Logistic Regression of Cannabis Use on Caregiving Status (N = 9,984)
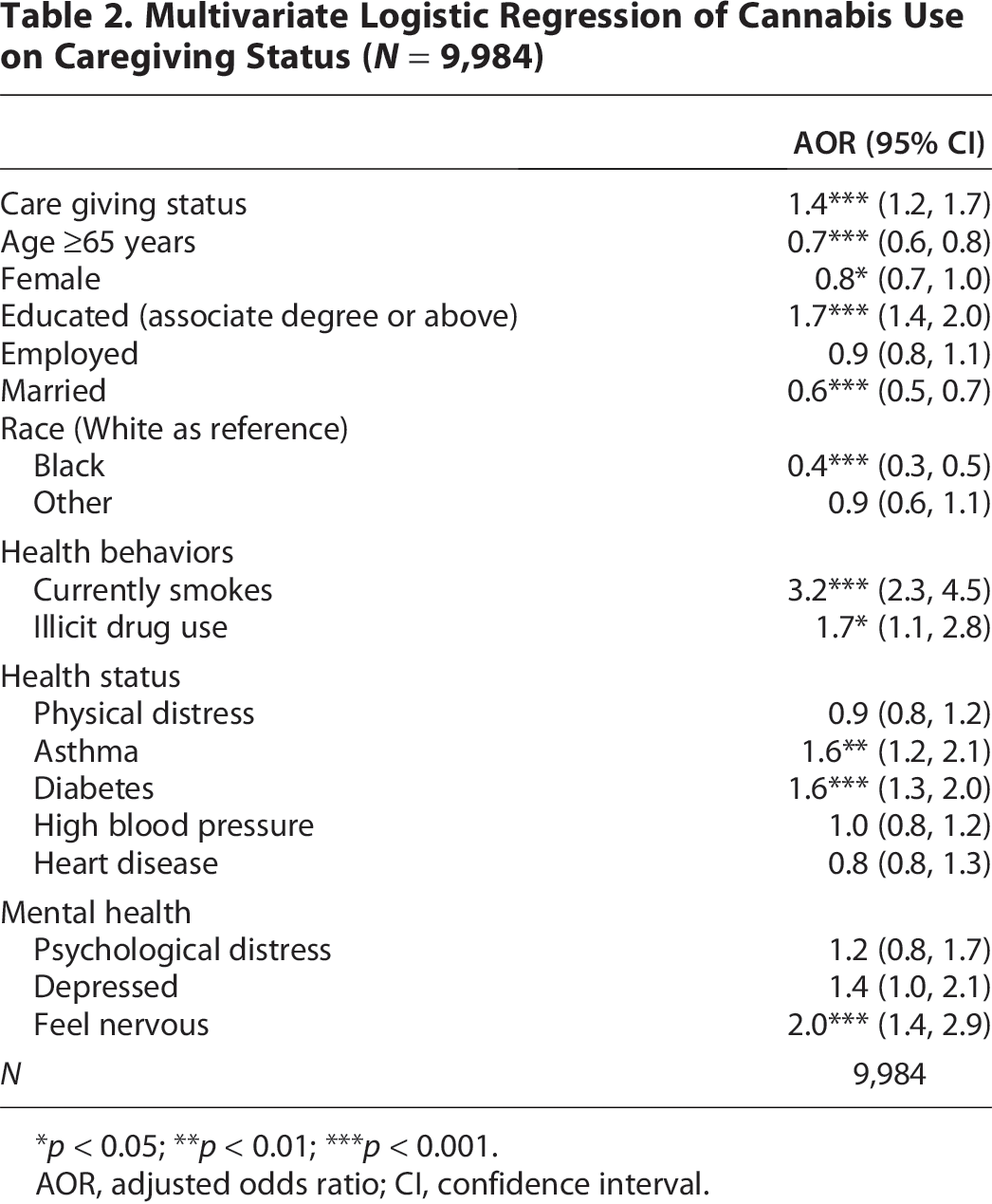
*p < 0.05; **p < 0.01; ***p < 0.001.
AOR, adjusted odds ratio; CI, confidence interval.
The results of the logistic model in which cannabis use among ICPs is regressed onto health status, mental health, and the intensity and nature of caregiving are provided in Table 3. ICPs who use cannabis are more likely to be younger (OR: 0.7; CI: 0.5, 0.8), college educated (OR: 1.6; CI: 1.2, 2.1),. and not married (OR: 0.7; CI: 0.5, 0.9). ICPs who use cannabis also are more likely to smoke (OR: 3.7; CI: 1.9, 7.2) and use illicit substances (OR: 2.5; CI: 1.2, 5.1). ICPs who use cannabis are more likely to be diagnosed with asthma (OR: 2.0; CI: 1.2,3.2) and diabetes (OR: 1.8; CI: 1.1,3.0) and report feeling nervous (OR: 2.1; CI: 1.3,3.8). We also observed those caring for someone with ADRD were more likely to use cannabis (OR: 1.5.0; CI: 1.1,2.0).
Multivariate Logistic Regression of Caregiving on Cannabis Use Among ICPs (N = 2,802)
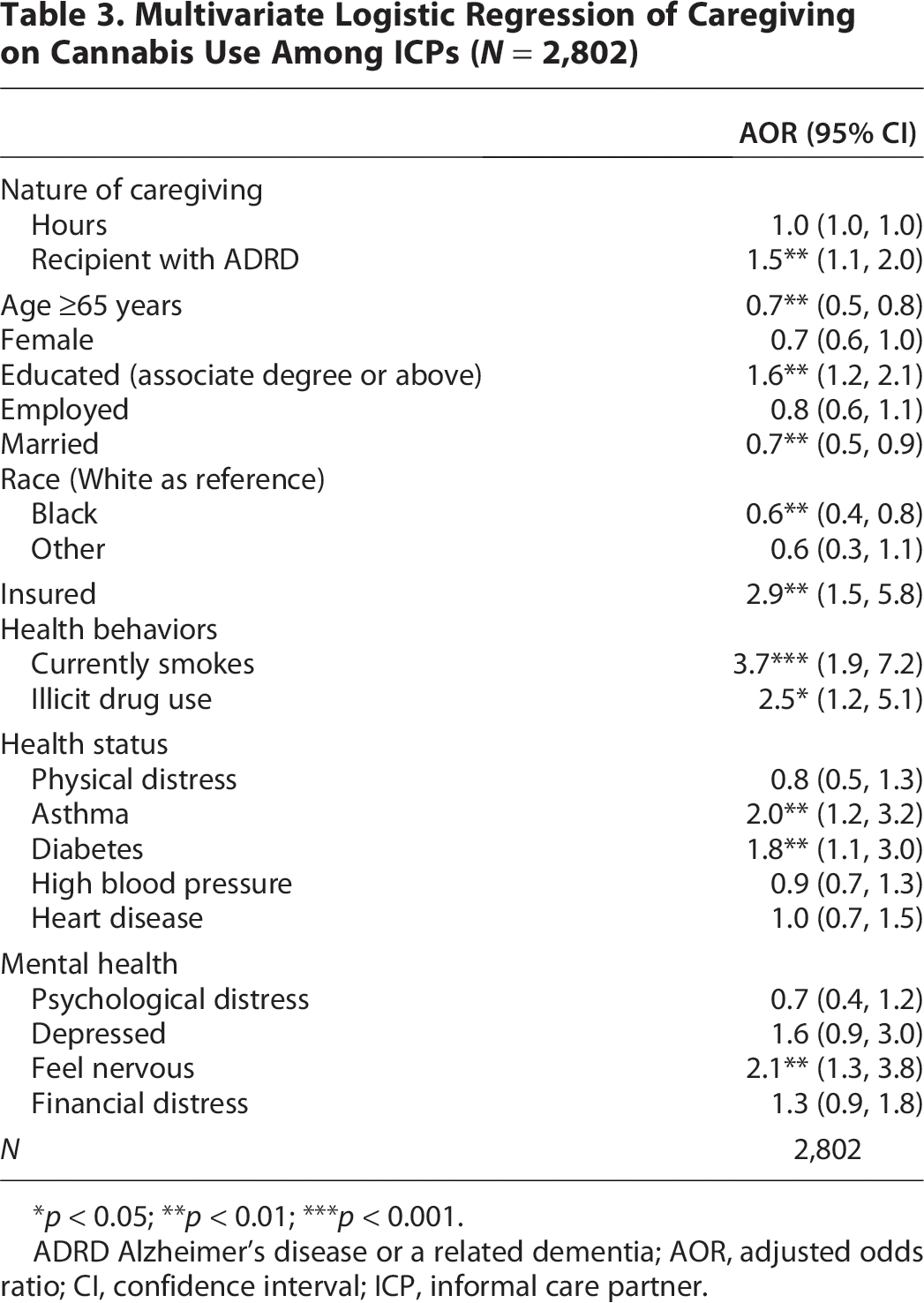
*p < 0.05; **p < 0.01; ***p < 0.001.
ADRD Alzheimer’s disease or a related dementia; AOR, adjusted odds ratio; CI, confidence interval; ICP, informal care partner.
Table 4 shows the results of regression models exploring association between cannabis use relative to use of outpatient medical care, ED visits, and care coordination among ICPs. These models control for all covariates included in Table 1 along with a variable accounting for the insurance status of the ICP. After adjusting for the covariates, past year cannabis use is associated with 0.6 additional number of doctor visits, and this association is statistically significant. We do not see any association between cannabis use and ED visits and care coordination. ICPs who use cannabis are more likely to delay care than ICPs who are nonusers of cannabis (OR: 2.7.0; CI: 1.9,3.8).
OLS and Logistic Regressions of Cannabis on Health Service Use Among ICPs (N = 2,802)
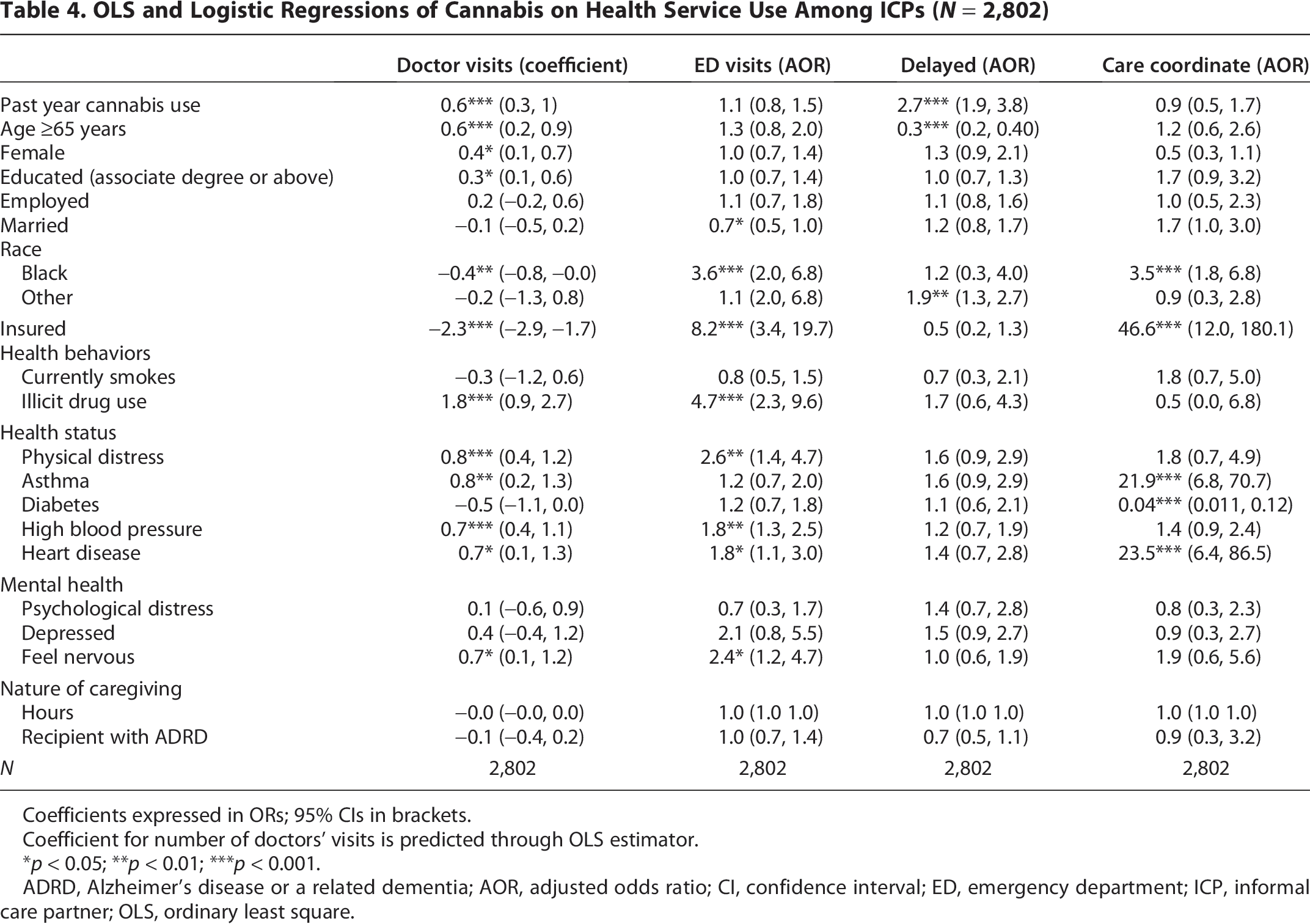
Coefficients expressed in ORs; 95% CIs in brackets.
Coefficient for number of doctors’ visits is predicted through OLS estimator.
*p < 0.05; **p < 0.01; ***p < 0.001.
ADRD, Alzheimer’s disease or a related dementia; AOR, adjusted odds ratio; CI, confidence interval; ED, emergency department; ICP, informal care partner; OLS, ordinary least square.
Discussion
This research advances scientific understanding of cannabis use among the understudied population of spouses, adult children, and others over age 50 who provide informal (i.e., not paid) care to the growing population of older adults who require daily assistance. 26 While our analytic sample of ICPs appears similar to ICPs nationwide (i.e., younger, female, well-educated, and employed),27–29 they clearly distinguished themselves in terms of past year cannabis use. We observed the cannabis use rates among older Californians substantially exceed national averages, and ICPs were more likely to use than non-ICPs. We suspect such large departures from national prevalence estimates (i.e., estimates suggest 10.7% among persons over 50 use cannabis) are a reflection of unique social and legal contexts. Californians have long held more generally favorable attitudes toward cannabis. 30 The state was among the first to legalize cannabis for medical purposes in 1996, 31 and our research team previously has observed older adults are more likely to use if living in a state where cannabis has been legalized. 26
Our finding that slightly more than one of every three older ICPs used cannabis in the past year warrants further consideration. On one hand, we observed how some ICPs who use cannabis appear like other older, life-long cannabis users as they are more likely to drink, smoke, and use illicit drugs than nonusers. On the other hand, older ICPs who used cannabis were more likely to be living with a diagnosed medical condition (i.e., asthma or diabetes), and among those who responded, nearly one of every four received guidance from a medical provider. These individuals may not have the same life-long history of cannabis use and may be more likely to use form therapeutic purposes only.
While previous research associated caregiving and mental health status, and other research has associated mental health status with cannabis use, our findings link the three. We observed how older ICPs experienced more mental health issues than those who were not involved in caregiving, and then we found that ICPs who used cannabis were particularly more likely to report being nervous. Are these older caregivers using cannabis as a form of self-care to address feeling nervous or some other type of distress? Is cannabis serving as a substitute or alternative to other evidence-based programs and services? Given the cross-sectional design of the CHIS survey and limited number of questions posed about mental health status (as well as physical health status), we did not have the opportunity to answer such critical questions.
Another critical discovery concerns how ICPs who use cannabis are more likely to care for PLwD. Given the absence of a federally approved cure or disease-modifying therapy, the persistence of ADRD, the lack of formal care providers, and the associated costs assumed by ICPs, there is a considerable public health need to promote access to therapeutic options. Yet, the most recently convened National Institutes of Health-sponsored Alzheimer’s forum ended with absolutely no discussion or guidance about cannabis use among caregivers of PLwD. Decision-making about cannabis use has been left to ICPs and their clinicians, resulting in widespread inconsistency at the patient, provider, and state policy levels about if, when, and under what conditions cannabis use may be helpful or harmful. 34
In this study, we also tested if cannabis use among ICPs was associated with outpatient medical care and emergency department visits. While we observed the former and believe that corresponds in some part with users seeking physicians to qualify them for cannabis program participation, we did not observe the latter. Given these mixed findings, future research should examine if such visits are associated with user experience (i.e., life-long users are less likely to seek out emergency care than naive users) or the type of product used (i.e., medically approved cannabis or recreational).
Interestingly, we also observed that ICPs who use cannabis were more likely to delay their own care, following previous research which reported nearly one of every three caregiver delays taking care of their personal health. 35 Perhaps some caregivers are using cannabis as a coping mechanism to manage nervousness or distress in lieu of seeking formal medical care, particularly when time, access, and even stigma may serve as barriers.
Limitations
While the CHIS offered an exceptional opportunity to examine a large sample of ICPs over 50 years old and identify correlates of cannabis use, the panel design only allows us a point in time snapshot. We attempted to address the need to test a longitudinal model by linking 2019 responses with the 2021 CHIS panel but found the survey questions were not standardized and limited our ability to draw reliable insights (e.g., temporal referencing questions concerning cannabis use to the past 12 months in 2019 and the past 30 days in 2021 limited comparisons between samples as incidence rates varied substantially). The CHIS also is limited in offering additional insights about ICPs and their cannabis use as the survey does not collect information about cannabis attitudes, historical use, and other variables that could further illuminate our models. Moreover, while we aspired to examine a range of physical and mental health effects associated with cannabis use, our modeling was constrained by the purposely limited number of questions fielded by the survey. While the CHIS data certainly illuminated an important and understudied population, we remain unsure if cannabis serves as a coping mechanism for caregivers. As rates of informal caregiving and cannabis use may increase over the next decade, researchers should continue to explore the drivers and outcomes of cannabis use. Looking forward, it may prove more productive for existing longitudinal surveys designed specifically for older adults and caregivers to consider adding questions that address these missing elements.
Concluding remarks
The number of aging Americans who provide informal care to another older adult is increasing. Meanwhile, we know little about the ways ICPs are taking care of or harming themselves by using cannabis. We expect cannabis use rates among ICPs will increase as younger cohorts, who already have higher cannabis use rates, grow older and increasingly become informal caregivers of older adults. Use rates also will increase as states continue to expand legal access.32,33 Moreover, we expect a growing number of ICPs who currently do not use cannabis are likely to consider cannabis use upon being informed by family, friends, formal care providers, or fellow caregiver support group participants about potential benefits. In fact, based on interviews of ICPs, we 19 found many ICPS would initiate cannabis use as a therapeutic alternative should other approaches to managing physical or psychological distress prove ineffective. Researchers must better understand the potential benefits and harms of cannabis use among ICPs and clinicians should consider increasing their engagement instead of leaving ICPs to make decisions without professional guidance.
Authors’ Contributions
B.K.: Concept, design, analysis, and article production. F.M.: Analysis and article production. D.B.: Design, analysis, and article production. K.A.: Concept, design, and article production. A.M.: Concept, design, and article production. A.L.N.: Concept, design, and article production. J.B.: Concept, design, and article production.
Footnotes
Acknowledgments
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the University of Iowa, College of Public Health, Department of Health Management and Policy.
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.