
Abstract
Background:
Autistic adults frequently have negative workplace experiences, as well as challenges with their psychological health, yet few studies have examined the linkages among aspects of employment and mental health in this group. To address this gap, we drew from the Job Demands-Resources model to investigate which aspects of employment were associated with psychological health outcomes in autistic adults.
Methods:
Participants were autistic adults (n = 109; 18–43 years old) employed in community settings, who completed online surveys and interviews about aspects of employment (perceived workplace climate, part-time vs. full-time employment, and occupational contact with others) and psychological health (depressive symptoms, psychological quality of life [PQOL]).
Results:
Perceived workplace climate was the only aspect of employment significantly associated with psychological health; adults who reported more positive workplace climates had higher PQOL. Workplace climate was more strongly associated with PQOL among adults in this sample who were older (vs. younger) and had lower (vs. higher) daily living skills.
Conclusion:
These findings highlight the importance of safe and supportive workplace climates for autistic adults, especially for those who have more challenges with daily living skills and are further into adulthood. Importantly, results may not generalize to those from racial or ethnically diverse backgrounds, nor to autistic adults who are minimally verbal or would otherwise be unable to self-report.
Community Brief
Why is this an important issue?
Autistic adults are more likely to have difficulties at work and with their mental health compared to non-autistic individuals. For many non-autistic adults, different aspects of their job (hours, workplace climate) are associated with better mental health. We do not know what parts of work are related to mental health in autistic adults.
What was the purpose of this study?
The purpose of this study was to understand what parts of a job are related to mental health in autistic adults. We also asked if there are differences for people based on their age, daily living skills (e.g., preparing a meal, using transportation), gender, or if they are in a college/university program.
What did the researchers do?
We collected data from 109 autistic adults (18–43 years old) through online surveys and interviews. Adults answered questions about their mental health (psychological quality of life, depressive symptoms). Adults also shared their feelings about their job and if they worked part-time versus full-time. We coded each adult’s job into a type of occupation using the Occupational Information Network. Each occupation is assigned an average score for the level of contact with others that was typical for the job. We tested if these aspects of employment were related to mental health.
What were the results and conclusions of the study?
Autistic adults who felt their workplace climate was more positive (i.e., safe, accepting of diversity, supportive) had higher psychological quality of life. The typical level of contact with others at the job and working part-time versus full-time were not related to psychological quality of life or depressive symptoms. The relationship between workplace climate and psychological quality of life was stronger for middle-aged autistic adults than those in early adulthood. This relationship was also stronger for autistic adults who had lower and average daily living skills (compared with those with higher daily living skills).
What is new or controversial about these findings?
Autistic adults reported better mental health when they were in more positive workplace climates. We found that working part-time versus full-time and the level of contact with others at the job were not related to mental health in this sample.
What are potential weaknesses in the study?
We only used data collected at one time point. We could not show whether aspects of employment caused autistic adults’ psychological health. We also did not talk to many autistic adults with intellectual disability so we do not know much about their feelings toward their jobs. We only examined a few job characteristics. Understanding if other aspects of employment (such as pay, accommodations, sensory environment) are related to autistic adults’ mental health is important for future research.
How will these findings help autistic adults now or in the future?
We found that autistic adults’ perception of their workplace climate is associated with mental health. Autistic adults need jobs they feel are safe, supportive, and valuing of diversity. These findings are important for interventions that help autistic adults with employment.
Background
It is well-known that, in the general population, positive workplace experiences are associated with heightened psychological well-being. 1 However, it is not fully understood whether workplace experiences impact autistic adults in similar ways. Autistic employees often experience stressors in the workplace, such as lack of support from supervisors and bullying from coworkers, 2 and they also tend to have worse psychological health than non-autistic individuals. 3 Yet, there have been few investigations of whether and which aspects of employment might be associated with psychological health in this group. To address this gap, we examined the associations between aspects of employment and psychological health, specifically depressive symptoms and psychological quality of life (PQOL), in a sample of autistic adults with community-based employment. Note that in this study, we use the term “aspects of employment” to refer to different facets of the job itself (e.g., weekly hours, job sector) as well as how the employee perceives their workplace experiences (e.g., how supportive or safe the workplace is).
Aspects of employment and psychological health in the general population
In the current study, we used the Job Demands-Resources (JD-R) model4–5 as a framework to understand different aspects of employment and their impact on autistic employees’ psychological health. Under the JD-R model, job demands are defined as aspects of employment that impose stress (e.g., lack of support from supervisors), whereas job resources are defined as those that facilitate personal growth and decrease the negative impacts of demands (e.g., positive relationships with coworkers).5–7 The JD-R model is a leading framework for understanding how aspects of employment impact mental health, with ample evidence supporting its utility in the general population; for example, research has shown that negative workplace climates in which employees feel unsupported by supervisors and coworkers are associated with reduced well-being. 8 In contrast, positive workplace climates in which employees feel supported by supervisors and coworkers are associated with heightened well-being. 1
Other job demands and resources include the number of hours employees are working (i.e., part-time or full-time). Part-time employment is associated with positive psychological health when these jobs improve work–life balance 9 and provide schedule flexibility.10–11 However, part-time employment is associated with negative psychological health among low-income adults 12 and among employees who desire full-time work, 13 as these jobs typically lack security, provide low wages, and lack social benefits. 14 These findings demonstrate how job demands and resources are associated with psychological health outcomes in the general population; however, little is known about how aspects of employment are associated with psychological health among autistic adults in the workforce.
Aspects of employment and psychological health in autistic adults
Prior researchers have used the JD-R framework in qualitative research to examine job demands and resources among autistic employees,15,16 but few studies have quantitatively examined associations between multiple aspects of employment and psychological health outcomes in this group. Autistic adults frequently report experiencing negative interactions with their supervisors and coworkers, such as bullying and disability-related stigma and discrimination.2,17 These job demands may negatively impact the psychological well-being of autistic employees, although this has yet to be tested directly. Alternatively, positive workplace climates in which autistic employees feel understood, supported, and treated fairly by their supervisors and coworkers may be especially beneficial to their psychological well-being.6,15 In addition, autistic employees frequently report difficulties interacting with others in the workplace 18 and often describe communication challenges as a job demand. 15 In a qualitative study from Hayward and colleagues, 19 several autistic employees reported a preference for jobs that they could perform independently without the need to interact with others. Although there is variability in preferences for social interaction among those on the autism spectrum,20,21 it may be that some autistic adults experience better psychological health in jobs where requirements for social contact are limited.15,19
As in the general population, the number of hours autistic employees work (part-time vs. full-time) may further impact their psychological health. Researchers have not examined associations between work hours and psychological health in autistic samples, yet there is reason to believe that autistic employees who work part-time may experience greater emotional well-being than those who work full-time. Autistic employees frequently report that they prefer flexible work schedules (which is more typical of part-time jobs) and the ability to choose their work hours,19,22 which are associated with positive psychological health in the general population. 10 Autistic adults are more likely to have part-time than full-time employment 23 ; therefore, it is important to understand how the number of working hours is associated with psychological health in autistic populations.
Autistic adults are a highly heterogenous group, and thus it is unlikely that aspects of employment are associated with mental health in a uniform way across the autism spectrum. Research in the general population has demonstrated that psychological health tends to differ across various demographic subgroups.24–26 For example, research in the general population indicates that females are at higher risk than males of experiencing depressive symptoms,27–28 and as adults increase in age, aspects of employment have a greater impact on mental health.29–30 It is also likely that aspects of employment have a lesser impact on psychological health when autistic adults are also enrolled in postsecondary education (PSE), particularly if the adult perceives the PSE program (and not the job) as their primary activity. In addition, because autistic adults with fewer daily living skills generally have a more difficult time obtaining employment31–34 and experience lower self-efficacy, 35 aspects of employment may have a greater impact on the psychological health of this subgroup. By investigating whether the psychological health of subgroups of autistic adults is more closely tied to aspects of employment, we can provide important information about who might be most vulnerable to job demands or benefit most from job resources.
Current study
To our knowledge, no study has tested a range of aspects of employment (both demands and resources) that may promote or impede psychological health among working autistic adults. Prior studies have examined individual aspects of employment in relation to autistic adults’ mental health.36,37 However, it is important to assess the relative impacts of multiple aspects of employment to understand which factors are particularly influential on psychological health. To address this gap, in the current study we focused on two research questions. First, we examined the associations between aspects of employment (i.e., perceived workplace climate, part-time vs. full-time employment, and occupational contact with others) and psychological health (depressive symptoms, PQOL). Second, due to heterogeneity across the autism spectrum, we investigated whether the strength of associations between aspects of employment and psychological health differed by the autistic adults’ gender, age, daily living skills, and whether they were enrolled in a PSE program. Based on prior research, we hypothesized that having a more positive workplace climate would be associated with better PQOL and fewer depressive symptoms. We did not have a priori hypotheses regarding the effects of working full-time versus part-time or level of contact with others because the majority of studies examining these issues in autism are qualitative and exploratory.
Methods
Participants
Participants in this study were part of a larger longitudinal study on employment stability among autistic adults. To be included in the larger study, participants were required to meet the following eligibility criteria: (1) 18–45 years old at the time of data collection; (2) able to provide documentation of an autism spectrum disorder diagnosis (e.g., diagnosis records from health care professionals, individualized education programs); (3) have exited high school and are no longer receiving services from the high school system; and (4) able to self-report and assent/consent independently. We required that participants be 18–45 years old because the larger longitudinal study focused on postsecondary employment and education in early adulthood. We required diagnosis documentation because understanding the impact of access to formal services was a goal of the larger study. Study team members asked each adult to identify an informant to participate with them, although we did not require that an informant participated for eligibility. A total of 199 adults and 176 informants participated in the larger study at baseline, and 131 of these adults (65.8%) were working for pay in the community. 38 ,1 To be eligible for the current analysis, we required that participants were working for pay in the community and have completed measures related to workplace experiences and psychological health in the questionnaire. Out of the 131 working autistic adults, we removed 22 from analyses due to missing or inconsistent data (primarily because they did not complete the survey). The current sample included 109 autistic adults between 18 and 43 years old (see Table 1 for demographic characteristics). The majority of adults included in the current sample (n = 96; 88.1%) participated in the larger study alongside an informant (76.0% mothers).
P
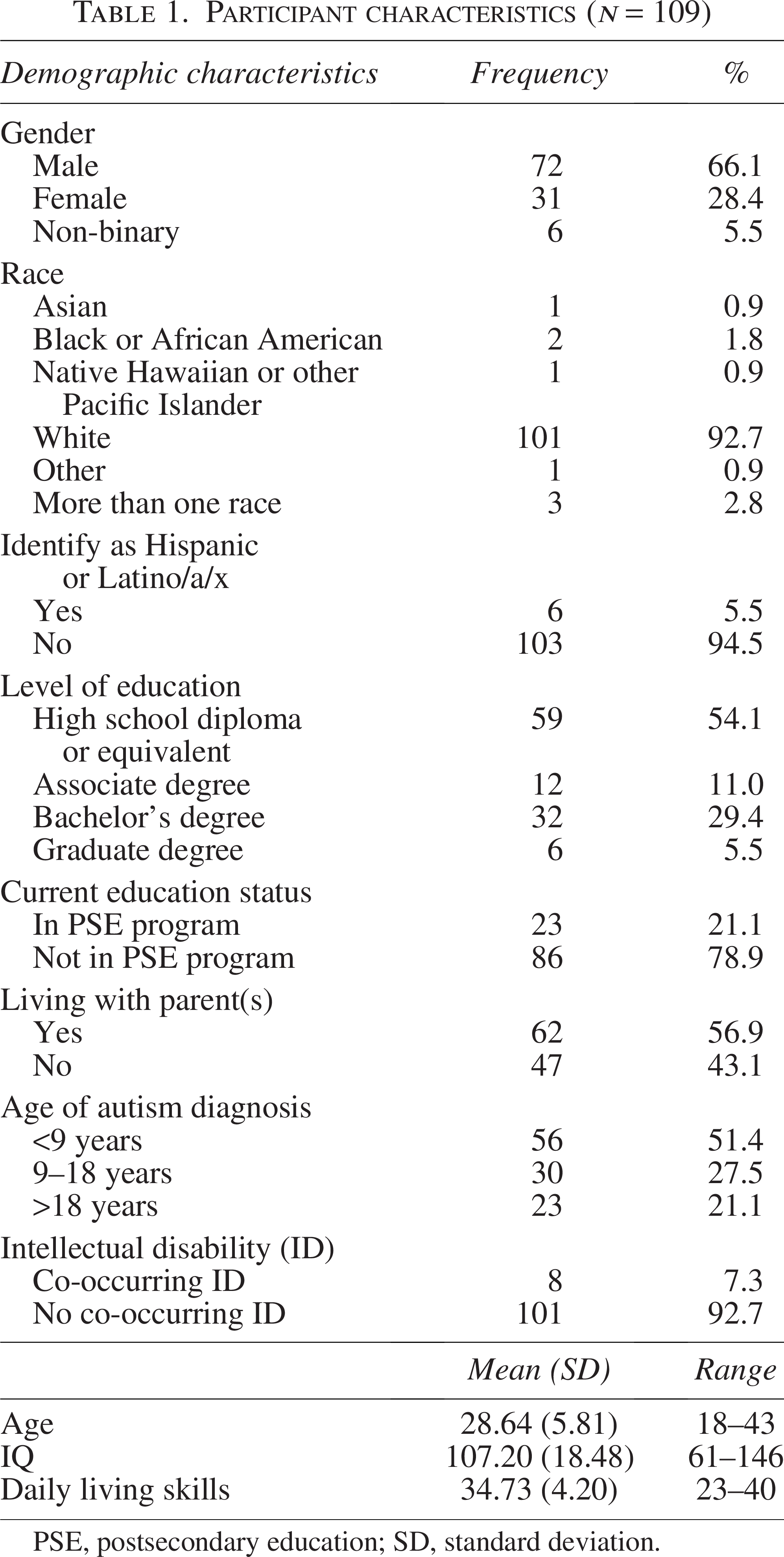
PSE, postsecondary education; SD, standard deviation.
Procedure
Data included in the current analysis were from the baseline time point of the larger longitudinal study; we collected data between May 2021 and March 2023. We recruited participants from the community through research registries, autism and other disability organizations, university newsletters, postings in newspapers, previous studies, mailings and flyers, emails, and word of mouth. If autistic adults and/or informants were interested in participating, we asked them to contact the study team. If an autistic adult contacted the study team and met the eligibility criteria, we asked them to identify an informant who would also be willing to participate. Meanwhile, if an informant contacted the study team, a research assistant asked to schedule a phone or video call with the autistic adult to inquire about their interest in participating and to confirm eligibility. By incorporating adult and informant reports in the larger study, the study team was able to collect and analyze multiple perspectives on adults’ experiences (see below for further details on how informant report was used in this study). 39
After screening, eligible adults and their informants provided verbal assent/consent, and a study team member emailed a link to an electronic consent/assent form or provided them with a paper form. Adults with legally authorized representatives completed an assent (vs. consent) form, and their representative provided consent for the adult’s participation. After signing the electronic consent form, adults and informants completed study surveys using an online survey platform (or mailed a paper version if preferred) and participated in interviews using an online videoconferencing platform. During the interview, adults and informants answered a series of questions about the adults’ current vocational and PSE activities. For adults who had paid employment in the community, we asked them and their informants about employment activities, including the title of the adults’ job(s), a description of their job responsibilities, and the number of hours they worked per week.
The Institutional Review Board (IRB) at Vanderbilt University Medical Center approved the procedures of the current study through a single IRB with two relying sites.
Use of informant report in this study
With the exception of daily living skills (see the Measures section for rationale), we primarily relied on information reported by the autistic adult, using informant report to supplement incomplete or replace missing adult reports. Specifically, every autistic adult in this analysis completed the interview about their current vocational and PSE activities; for variables resulting from this interview (i.e., Occupational Information Network [O*NET] standardized occupations job codes, occupational contact with others, number of hours, whether the adult is in PSE), we used informant information to supplement information provided by the autistic adult, allowing us to generate a more complete picture of vocational/educational activities.
For autistic adults who did not complete the demographic questions used or reported in this analysis (i.e., gender, age, race, ethnicity, living situation, education), we substituted informant report of adult demographics as a best estimate (the number of substituted values ranged from 22% to 24% across these variables; age of autism diagnosis also included review of records and is described further below). Importantly, for measures that reflect internal states (and could be difficult for an informant to accurately report) such as perceived workplace climate, depressive symptoms, and PQOL, we used only the report of the autistic adult and excluded adults from analysis who did not provide that report.
Job coding procedure
We matched each job to a standardized occupation defined by the O*NET 40 . The O*NET is a comprehensive database of occupations and associated characteristics provided by the U.S. Department of Labor. Once an occupation is matched to a participant’s job, the O*NET provides numerous characteristics about the occupation that can be coded in quantitative ways and used in analyses (see the Measures section for a fuller description of the variable that was drawn from O*NET for the present study).
There are over 900 potential O*NET job titles 40 that could be matched to participants’ jobs. The distinctions between many of the codes are highly nuanced, such as statistician versus biostatistician, audiovisual equipment installers and repairers versus telecommunications equipment installers and repairers, and proofreaders and copy markers versus word processors and typists. 40 Given the many possible codes, we used a three-step process to produce reliable O*NET occupation codes. First, two independent coders individually matched each job description provided by the adult (supplemented with information from the informant) to an O*NET occupation. After coding independently, both coders went through each case to determine if there were discrepancies. In 49.5% of cases, both coders applied the exact same code, and thus assigned that code to the participant’s job. Second, for the remaining cases, the independent coders discussed the case until they reached agreement. Third, in cases where there remained a question about the best fitting code, the study principal investigators and research team discussed until reaching consensus. If adults (and their informants) reported having multiple jobs, we coded the job at which the adult worked the most hours. This method of coding participant-reported jobs using occupational information from O*NET has been implemented in prior studies. 41
Measures
Aspects of employment
Occupational Contact with Others
After coding each job, we used occupational information from O*NET 40 to identify each occupation’s typical level of contact with others. The O*NET collected a nationally representative survey administered by the U.S. Department of Labor to determine occupational contact scores. 42 As part of this survey, respondents working in a given occupation were asked the following question: “How much contact with others (by telephone, face-to-face, or otherwise) is required to perform your current job?” Supervisors, human resource professionals, and former employees in a given occupation were also asked the following question: “How much contact with others (by telephone, face-to-face, or otherwise) is required to perform the occupation?” Response options included the following: 1 = no contact with others; 2 = occasional contact with others; 3 = contact with others about half the time; 4 = contact with others most of the time; and 5 = constant contact with others. 40 Contact scores from respondents within the same occupation were averaged by O*NET, and each occupation’s average was standardized on a scale from 0 to 100 (0 = no contact with others, 100 = constant contact with others) to produce an occupational contact score available through the O*NET database.
Part-Time Versus Full-Time Employment
When completing the vocational and educational interview, adults and informants reported the average number of hours per week the autistic adult worked at their job. We dichotomized responses into part-time employment (under 35 hours per week) and full-time employment (35 or more hours per week), as defined by the U.S. Bureau of Labor Statistics. 43
Perceived Workplace Climate
Autistic adults completed three self-report, adapted questionnaires that measured their perceptions of their workplace climate. These questionnaires are commonly used in the general population44–51 and were altered to improve accessibility by adjusting the wording to be at a lower reading level and reducing the number of response options from a 7-point to a 5-point scale, as recommended by Kooijmans and colleagues. 52 The first four-item questionnaire, adapted from a measure used by Edmondson, 53 measured the psychological safety of the adult’s workplace, or the degree to which their thoughts, skills, and ideas were valued at work (e.g., “It is safe for me to speak up at work.”). The second seven-item questionnaire, adapted from measures used by McKay and colleagues 54 and Mor Barak and colleagues, 55 measured the diversity climate of the adult’s workplace, or the degree to which employees from different backgrounds were included and treated fairly at work (e.g., “It is important to my supervisor that all types of people feel welcome and safe at work.”). The final nine-item questionnaire, adapted from measures from Graen and Uhl-Bien 56 and Niehoff and Moorman, 57 measured the leader–member exchange of the adult’s workplace, or the degree to which their supervisor practiced positive communication and leadership skills (e.g., “My supervisor understands my needs at work.”). Respondents rated the degree to which they agreed with each item on a 5-point scale (1 = not at all, 5 = all the time). For each measure, we averaged the items to produce a mean score. Cronbach’s alphas were .63 for psychological safety, .92 for diversity climate, and .92 for leader–member exchange in the current sample. Due to multicollinearity among subscales and a confirmatory factor analysis that indicated the three factors loaded onto a singular second-order factor, we averaged the mean subscale scores to produce a single average of workplace climate for each participant. A complete list of the items and additional information regarding the combination of workplace climate measures into a single score are available in the Supplementary Data.
Psychological health
Depressive Symptoms
Autistic adults completed the Beck Depression Inventory-II (BDI-II 58 ), a self-report 21-item questionnaire that measures the presence and severity of depressive symptoms. Due to the sensitivity of one of the items addressing suicidal thoughts, the study team did not include this item in the questionnaire, and therefore, we used the remaining 20 items to calculate total scores. The BDI-II has been shown to be a valid measure of depressive symptoms in autistic samples.59–60 The current sample had a Cronbach’s alpha of .90.
Psychological Quality of Life
Autistic adults self-reported on their PQOL using the psychological domain of the World Health Organization Quality of Life Scale (WHOQoL-BREF 61 ). The WHOQoL-BREF is a 26-item questionnaire that assesses four quality-of-life domains: physical, psychological, social relationships, and environment. The PQOL subscale consists of six items (e.g., “How much do you enjoy life?”) that measure respondents’ psychological health. We standardized the raw scores on the PQOL subscale into t-scores, which we used in the current study. The PQOL subscale has been shown to be a valid measure of PQOL in autistic samples. 62 A Cronbach’s alpha of .86 was found for the current sample.
Demographic and behavioral characteristics
Demographics
Autistic adults reported on their age, gender identity (male, female, non-binary/other), race, ethnicity, highest education level, whether they lived with their parents, and age of autism diagnosis through the online questionnaire. We coded highest education level into one of five categories (less than high school, high school diploma or equivalent, associate degree, bachelor’s degree, graduate degree). Using data from the vocational and educational interview, we coded adults’ current PSE status (1 = currently in a PSE program; 0 = not currently in a PSE program). As described above, when the adult’s self-report of these variables was unclear or missing, we utilized or supplemented with informant-report.
For age of autism diagnosis, in addition to self- and informant-report, we also had the option to extract age of diagnosis from diagnostic records (i.e., medical, clinical, educational evaluations) provided for the study. In most cases (66.1%) we used adult-reported age of diagnosis. When the adult report was missing or the adult was not sure when they were diagnosed, we used informant report of age of diagnosis (31.2%). If the adult and the informant were both unsure of the adult’s age of diagnosis, or age of diagnosis was unclear based on both reports, we used information extracted from the medical or educational records to determine age of autism diagnosis (2.8%).
We used a case consensus procedure to classify whether the autistic adults had a co-occurring intellectual disability in addition to autism. Two PhD-level psychologists conducted the case consensus, using all available information from adults and informants to classify the adults, including IQ scores, adaptive behavior measures, and background information such as report of intellectual disability diagnosis, the level of inclusion the adult experienced while in high school, and the type of diploma (e.g., regular diploma, occupational diploma) the adult received. We primarily obtained standardized IQ scores by administering the Wechsler Abbreviated Scale of Intelligence, Second Edition (WASI-II 63 ) as part of the larger study. However, when available, we used standardized IQ scores from tests that were previously administered, including from the WASI-II, Wechsler Abbreviated Scale of Intelligence, First Edition (WASI 64 ), the Leiter International Performance Scale, Third Edition, 65 or the Wide Range Intelligence Test (WRIT 66 ).
Daily Living Skills
We measured daily living skills using the Waisman Activities of Daily Living (W-ADL 67 ) scale. The W-ADL is a 20-item measure that assesses adults’ level of independence in completing daily tasks (e.g., “preparing complete meal”). Informants rated the degree to which adults could complete each task independently on a 3-point scale (0 = does not do at all, 1 = with help, 2 = independent). Although there are a few studies that have used the W-ADL as a self-report measure,68,69 it was intended to be an informant-report measure and demonstrates strong psychometric properties when used in this way. 67 Thus, we chose to use informant report in this study. We used adult-report W-ADL scores, which we collected via online survey, if informant-report scores were unavailable (12.8% of the sample only had adult report). Since the adult-report W-ADL omits three items that are included on the informant-report measure (“toileting,” “drinking from a cup,” “eating from a plate”), we increased adult scores by 6 (scores of 2 on each missing item) with the assumption that adults who participated in the study without support would also be able to independently complete these basic activities of daily living. The Cronbach’s alpha was .77 for the current sample.
Analysis
We tested basic assumptions for linear regression before including predictors in the current models. To address the first research question, we implemented linear regression analyses to determine which aspects of employment independently predicted depressive symptoms and PQOL. Predictors of depressive symptoms and PQOL included perceived workplace climate (psychological safety, diversity climate, leader–member exchange), occupational contact, and part-time versus full-time employment. We corrected the p-values for the aspects of employment using the false discovery rate (FDR) method for both models. 70 Psychological health tends to differ across various demographic subgroups, 26 and therefore, gender, age, daily living skills, and PSE enrollment were included as covariates in both the regression models.
We implemented additional linear regression analyses for the second research question, to determine whether the strength of the associations between aspects of employment and psychological health differed across specific demographic and behavioral characteristics. We only entered aspects of employment as predictors in the moderation models that had significant main effects (using corrected p-values) on depressive symptoms and/or PQOL in Research Question 1. If an aspect of employment had a significant main effect on depressive symptoms and/or PQOL, we tested the interaction effects between the aspect of employment and the four demographic/behavioral variables (gender, age, daily living skills, and PSE enrollment) on the respective outcome measure(s). Demographic/behavioral characteristics not included in the interaction term were entered as covariates in the model.
The data used in this study will be available through the National Database for Autism Research. The code used for analyses conducted in R version 4.4.3
71
is available on
Results
Associations between aspects of employment and psychological health
Estimates from regression models examining the independent main effects of aspects of employment predicting depressive symptoms and PQOL are presented in Table 2. Adults who reported more positive workplace climates had significantly higher PQOL. After applying the FDR correction, workplace climate did not significantly predict depressive symptoms. Occupational contact and part-time versus full-time work did not significantly predict depressive symptoms or PQOL.
L
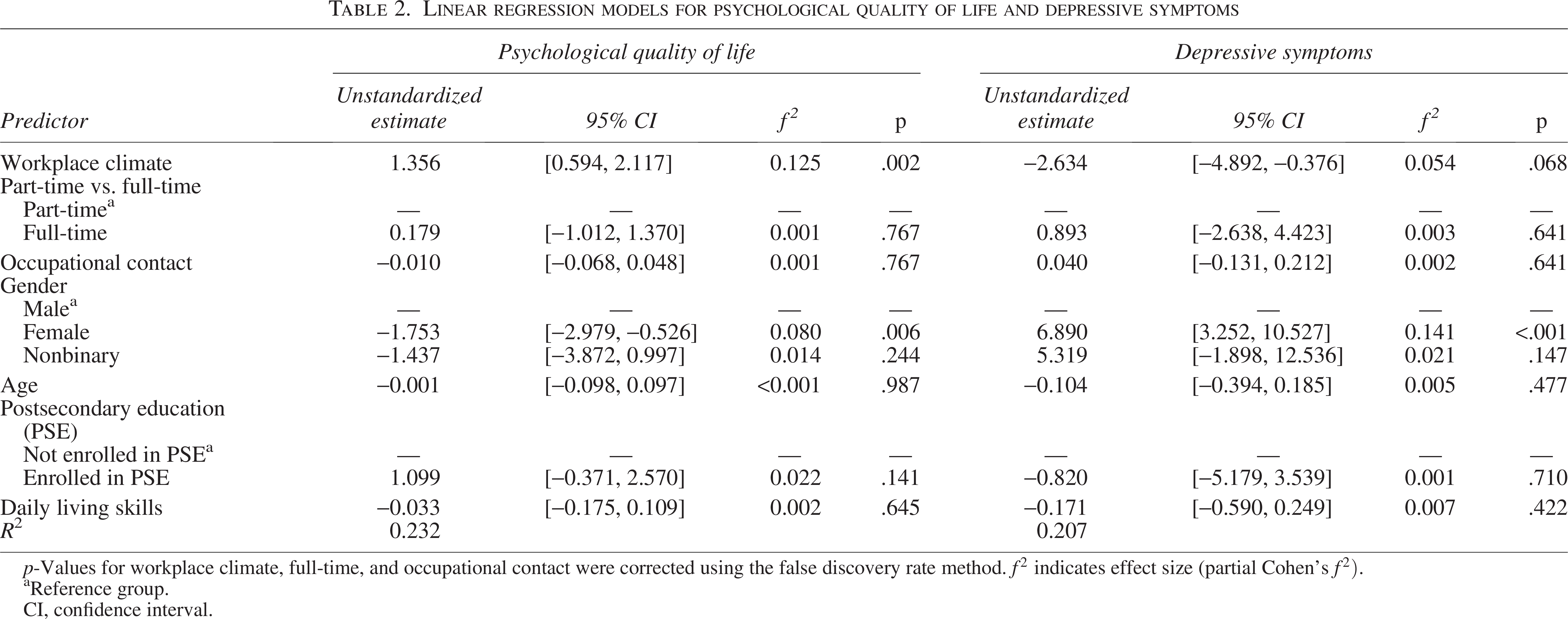
p-Values for workplace climate, full-time, and occupational contact were corrected using the false discovery rate method.
Reference group.
CI, confidence interval.
Effect modification by gender, age, daily living skills, or PSE enrollment
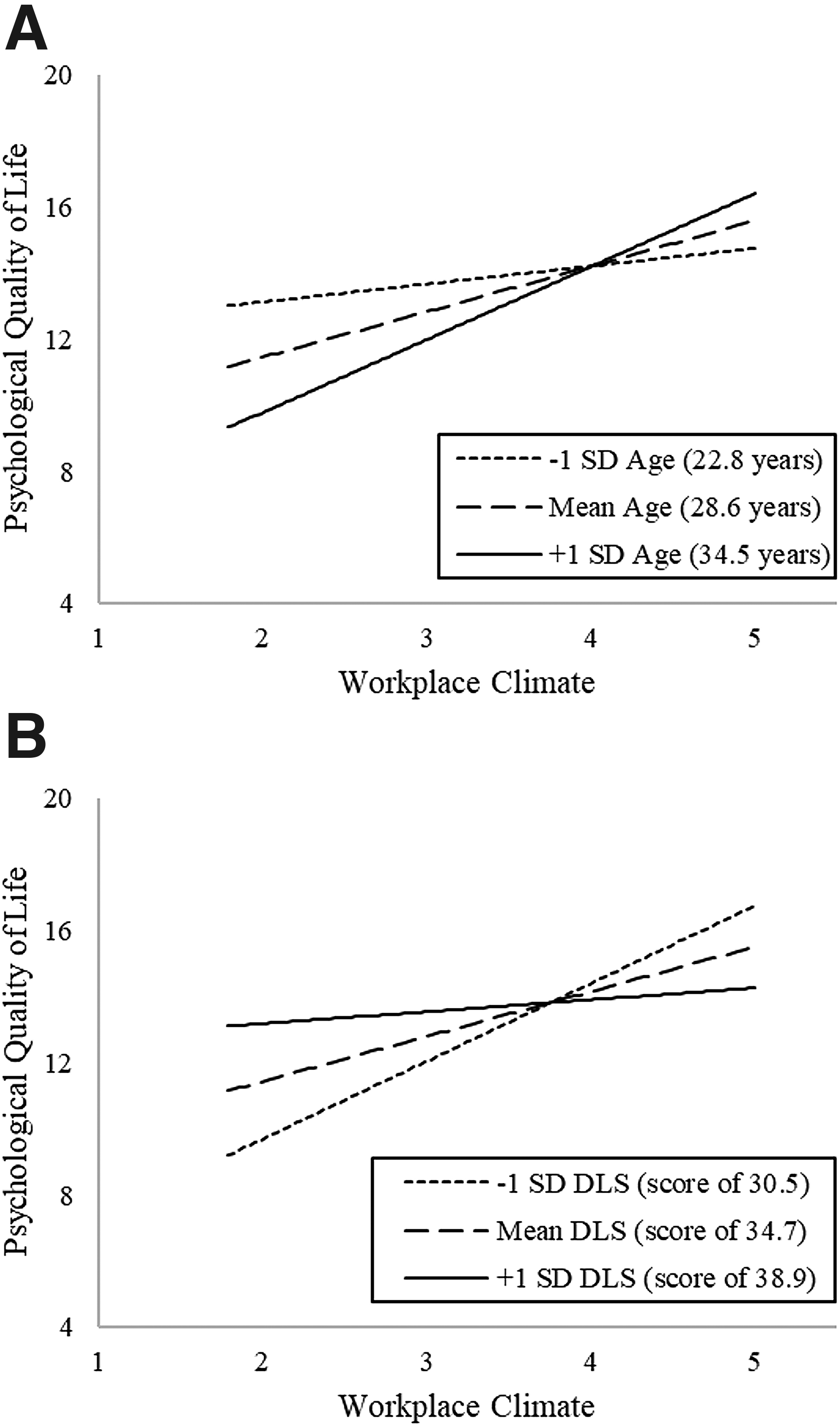
Because workplace climate had a significant main effect on PQOL, we tested the interaction effects between workplace climate and the demographic/behavioral variables (gender, age, daily living skills, and PSE enrollment) on PQOL. As shown in Table 3, the effects of workplace climate on PQOL did not significantly differ across gender or PSE enrollment. We detected a statistically significant interaction between age and workplace climate on PQOL (p = .035), depicted in Figure 1A. Our analyses of the simple slopes suggested that more positive workplace climates were associated with higher PQOL among adults who were at the mean age of the sample (i.e., 28.6 years; b = 1.37, 95% confidence interval [CI: 0.64, 2.11], p < .001); this association was even stronger among adults who were 1 standard deviation older than the mean age (i.e., 34.5 years; b = 2.21, 95% CI: [1.12, 3.30], p < .001). Meanwhile, workplace climate was not associated with PQOL among adults who were 1 standard deviation younger than the mean age of the sample (i.e., 22.8 years; b = 0.54, 95% CI: [−0.50,1.58], p = .304).
M
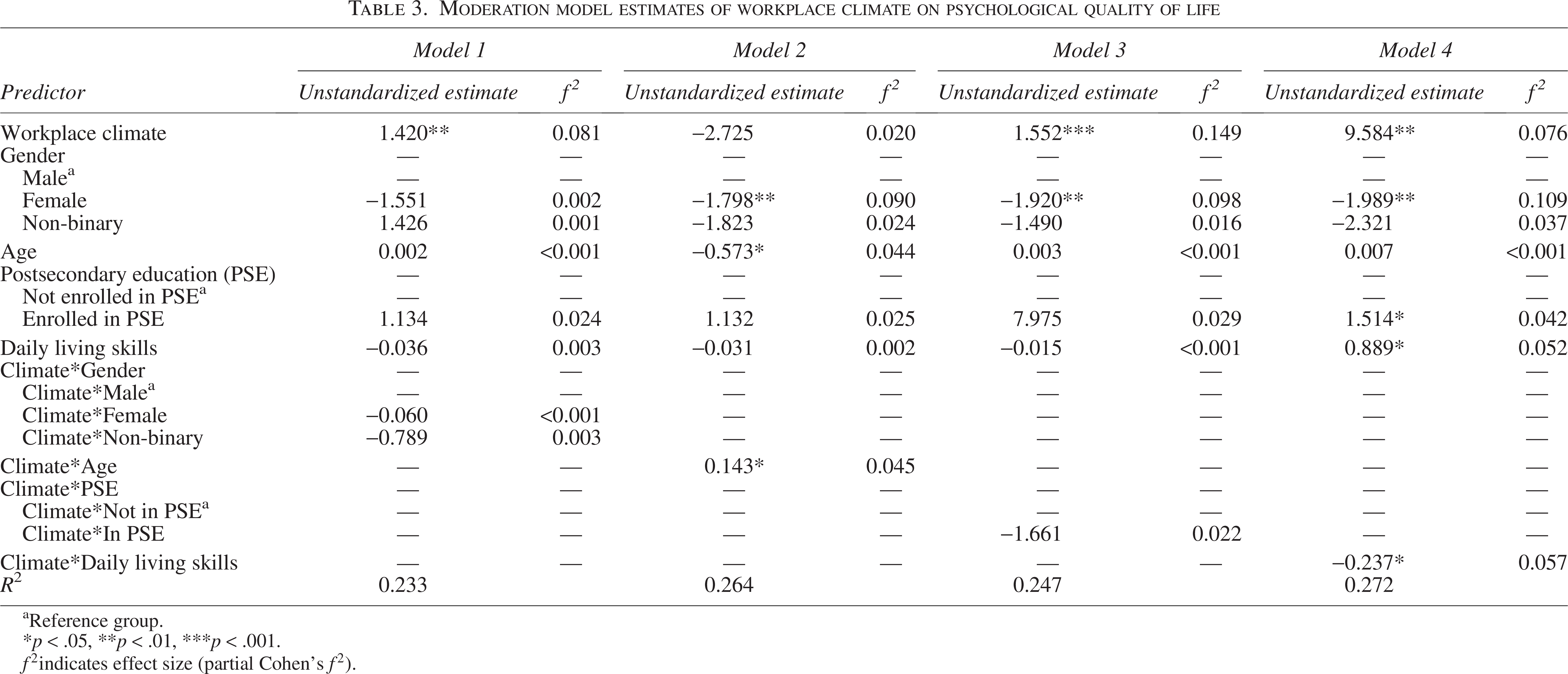
aReference group.
*p < .05, **p < .01, ***p < .001.
As shown in Table 3, we also detected a significant interaction between daily living skills and workplace climate on PQOL (p = .018). Figure 1B depicts this interaction. We analyzed the simple slopes and found that more positive workplace climates were associated with higher PQOL among autistic adults who had daily living skills at the average of the sample (i.e., W-ADL score of 34.7; b = 1.36, 95% CI: [0.63, 2.08], p < .001). The association between climate and PQOL was even stronger for autistic adults 1 standard deviation below the mean score (i.e., W-ADL score of 30.5; b = 2.35, 95% CI: [1.24, 3.46], p < .001). However, workplace climate and PQOL were not significantly associated for autistic adults 1 standard deviation above the average W-ADL score for this sample (i.e., W-ADL score of 38.9; b = 0.36, 95% CI: [−0.73, 1.45], p = .512), suggesting that the effect of workplace climate on PQOL may be stronger for autistic adults with lower (vs. higher) levels of daily living skills. We included CIs and complete p-values for all estimates from Table 3 in Supplementary Table S2 in the Supplementary Data.
Discussion
In the current study, we used the JD-R framework to examine associations between aspects of employment and psychological health in a sample of working autistic adults. Consistent with studies of the general population,1,8 and as hypothesized, autistic adults in the current study who perceived their workplace climate to be more positive reported better PQOL. Prior qualitative research has demonstrated that autistic adults frequently report stressors in the workplace, including stigma and discrimination, 17 negative treatment from coworkers, 2 and lack of support from supervisors. 2 Our findings demonstrate quantitatively that indicators of positive workplace climates (climates perceived as high in psychological safety, leader–member exchange, and valuing of diversity) are associated with higher PQOL among autistic adults, highlighting the importance of safe and supportive workplace climates among autistic employees.
We further found that the effects of perceived workplace climate on psychological health were more pronounced for some subgroups of autistic adults in our sample than others. Specifically, the simple slope analysis suggested that for autistic adults in their late teenage years into their early 20s, workplace climates were not associated with PQOL. However, for adults in their late 20s and early 30s, more positive workplace climates were associated with higher PQOL. This finding supports research from the general population demonstrating that as adults increase in age, their workplace experiences have stronger ties to their psychological health.29–30
Age-related modifications of the association between workplace climate and PQOL can potentially be understood in the context of changing employment status across adulthood. In the current study, autistic adults who were younger than 28.6 (i.e., below the mean age in this sample) were twice as likely to work part-time as full-time (66% vs. 34%), whereas participants who were older than 28.6 were equally likely to work part-time as full-time (51% vs. 49%). Adults who are further into adulthood have also likely spent more time in the workforce than younger adults. 43 As autistic adults spend more time at their workplace and accumulate more work experience, their workplace climates may become increasingly more important to their PQOL. Our finding therefore indicates the need for interventions designed to foster safe, supportive workplace climates for autistic employees, particularly for middle-aged autistic adults.
In addition to age, we also found that for autistic adults with daily living skills at or below the average W-ADL score in our sample, more positive workplace climates were related to higher PQOL. In comparison, for autistic adults with above-average daily living skills in the sample (i.e., 1 standard deviation above the mean), workplace climate and PQOL were not associated. Our results suggest that the effect of positive workplace climates on higher PQOL may be stronger as level of daily living skills decreases. Ample prior research has found that autistic adults with lower (vs. higher) daily living skills experience greater challenges with employment34,72; having supportive coworkers and supervisors may be especially relevant for their PQOL. Overall, these findings indicate the need for interventions designed to foster safe, supportive workplace climates for autistic employees, particularly autistic adults further into adulthood and for those with fewer daily living skills.
The pattern of findings observed in this study suggests that, among autistic adults, the subjective experiences of employment may be more important to psychological health than the structural aspects of employment themselves. Perceived workplace climate was the only aspect of employment significantly associated with psychological health. Alternatively, in the general population, researchers have shown that the number of work hours (part-time vs. full-time) impacts psychological health. 11 Although null findings should be interpreted with caution, this nonsignificant finding suggests that some aspects of employment that optimize psychological health in the general population may not have the same effect among autistic adults. It may be, then, that structural aspects of employment such as part-time versus full-time work might have a stronger association with mental health if autistic adults perceive them as positive or negative.
Similarly, although prior research has demonstrated that autistic adults often report difficulties interacting with others in the workplace, 18 we did not find significant associations between occupational contact and depressive symptoms or PQOL in this sample. However, our analysis did not take into account the variability in the amount and type of contact autistic adults prefer in the workplace73–74 ; for example, many autistic adults find nondirect forms of contact (e.g., email, chat applications) less difficult to navigate than direct forms of contact.75–76 Whereas some autistic employees may prefer jobs with limited social interaction, others may prefer frequent social interaction with perhaps workplace adjustments to the social environment, such as increased clarity in communication or understanding of differences in social preferences. 19 Future research should therefore consider whether autistic adults’ weekly hours and experiences at work (such as level of contact) meet their preferences, and whether discrepancies between their preferences and experiences impact their psychological health.
It is also important to note that an occupation’s contact score in the O*NET (which we used in the present study) represents the level of contact typically experienced by employees in that occupation. This score did not account for the variability of contact within a single occupation or the quality of those interactions. Therefore, in the current study, a participant’s occupational contact code may not have reflected the level of contact they actually experienced at work. Additional research is needed to measure more precise estimates of autistic adults’ contact with others at work, as opposed to using an average based on the general population.
Furthermore, it may be that we cannot understand the impact of these more structural aspects of employment (e.g., number of hours, level of contact) on psychological health without simultaneously considering autism-specific experiences. Differences in social communication and sensory sensitivities77,78 may work in combination with structural aspects of employment to impact psychological health in distinct ways for autistic adults. Regarding weekly hours, for example, it is possible that the effects of working part-time versus full-time on psychological health will differ depending on the sensory environment. If the sensory environment is overwhelming, there may be a negative impact of working more hours on psychological health, whereas working more hours might positively impact psychological health in a sensory environment that is a better fit for the autistic adult. In relation to the level of contact with others in a job, autistic adults may experience heighted pressures to mask or “camouflage” their autistic traits in the workplace. Increased expectations for interaction with others may therefore more negatively impact autistic adults, whereas the amount of social contact may not be related to psychological health if autistic adults feel the need to mask is minimized.
Finally, our analyses focused on associations between aspects of employment and psychological health. However, it is important to understand how or why workplace characteristics are related to psychological health. One potential mechanism in which aspects of employment may lead to negative mental health is through “autistic burnout,” defined as a state of exhaustion from being an autistic person in a neurotypical world.79,80 It may be that certain aspects of employment (e.g., a negative perceived workplace climate) lead to greater feelings of autistic burnout, which then might lead to poor psychological health. The JD-R model has been adapted to understand occupational burnout in autistic employees 6 and could be a promising framework for exploring these processes.
Limitations
There are a few limitations of the current study worth noting. Since the data used in this study were cross-sectional, the current analyses examined associations, not causal relationships, between aspects of employment and psychological health. It may be that poorer psychological health leads to the perception of a less positive workplace climate; adults with greater depressive symptoms are more likely to demonstrate interpretation biases in which they appraise ambiguous situations as negative. 81 Longitudinal studies are needed to determine the direction of effects between aspects of employment and psychological health. In addition, we did not conduct an a priori power analysis for the current analyses.
In terms of our study sample, the sample was primarily White, non-Hispanic/Latinx and was therefore limited in racial/ethnic diversity. It is well-established that employees from underrepresented racial/ethnic groups experience specific stressors in the workplace, including lower wages 82 and heightened discrimination. 83 Therefore, further research is needed because workplace stressors experienced by autistic employees with multiple underrepresented identities may have a particularly negative impact on their psychological health. In addition, the larger study focused on autistic individuals’ experiences during early adulthood. Given that the sample’s age range was 18–43 years, future research should examine how aspects of employment may influence autistic adults’ psychological health later into adulthood. Our analyses also did not include non-autistic adults, which limited our ability to draw comparisons between autistic and non-autistic adults.
Furthermore, all the participants in the current sample were able to self-report, generally had moderate to high daily living skills, and only 7.3% had co-occurring intellectual disability. The underrepresentation of autistic adults with intellectual disability in the current sample may reflect their lower participation in competitive employment.84,85 Consequently, the present findings may not translate to autistic employees who are unable to self-report or who need more substantial support at their jobs. They also may not generalize to adults who identify as autistic but do not have a formal diagnosis (as we required all participants in this study to have an autism diagnosis). Given the barriers to autism diagnosis,86–88 further research is needed to understand how aspects of employment might be related to mental health in adults who have not received a formal diagnosis. While the O*NET classification system is a useful tool for categorizing reported jobs into standardized occupations, this coding system does not account for variability in job responsibilities, work contexts, and preparation requirements across different jobs in a single occupation—all which may contribute to autistic adults’ psychological health.
Finally, the current study focused on a limited number of aspects of employment, drawing from research with autistic adults and the general population. There are many other aspects of employment to consider in future research, some of which may have unique impacts on psychological health for autistic employees. For instance, autistic employees often receive workplace accommodations or supports, such as task reminders, job coaches, or flexible schedules. 89 The availability of desired accommodations and support in the workplace, and their quality may have important influences on mental health. 17 Likewise, autistic adults frequently report desiring accommodations for sensory sensitivities, such as adjustments to workplace lighting and noise levels18,19,90 and acceptance of stimming behaviors. 91 Higher sensory sensitivities in autistic adults have been linked with lower job satisfaction 92 and heightened anxiety. 78 Therefore, future research may want to explore how matches between the sensory environment in the workplace and an adult’s sensory needs impact psychological health.
These limitations are offset by some notable strengths. Incorporation of subjective and objective aspects of employment was an important strength, as it allowed us to limit reporter bias and shed light on the potential importance of differentiating autistic adults’ subjective experiences in the workplace compared with more structural measures used in the general population. Prior studies of employment typically include autistic adults who primarily received their autism diagnosis in adulthood93–94 ; the age of autism diagnosis in this sample is more variable (see Table 1), better reflecting the population of autistic adults who can self-report.
Conclusion
By examining workplace correlates of psychological health among autistic adults, we were able to identify targets for intervention that may promote their psychological health in the workplace and increase their employment success. Our findings also highlight the importance of workplace climates in which autistic employees feel supported and understood by their supervisors and coworkers; positive workplace climates were especially important to the psychological health of adults as they moved from early into middle adulthood and for those with greater challenges in daily living skills.
Footnotes
Acknowledgments
The authors are grateful to the autistic adults and their families and friends who participated in this study.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
This research was supported by the National Institute of Mental Health (R01 MH121438, PIs: L.S.D., J.L.T.), National Institute on Aging (R01 AG08768, PI: Malick), Vanderbilt Undergraduate Summer Research Program, and Littlejohn Family. Core support was provided by the National Institute of Child Health and Human Development (P50 HD103537, PI: Neul; P50 HD105353, PI: Chang), and the National Center for Advancing Translational Sciences (UL1 TR000445).
Authorship Confirmation Statement
S.B.M.: Lead role in conceptualization, data curation, formal analysis, visualization, and writing—original draft and an equal role in methodology and writing—review and editing. N.L., PhD: Lead role in validation, equal role in conceptualization and writing—review and editing, and supporting role in methodology and supervision. V.S.: Supporting role in conceptualization, methodology, supervision, and writing—review and editing. L.S.D., PhD: Lead role in supervision. Equal role in conceptualization, methodology, project administration, resources, and writing—review and editing. J.L.T., PhD: Lead role in supervision. Equal role in conceptualization, methodology, project administration, resources, and writing—review and editing. This article has been given solely to this journal and is not published, in press, or submitted elsewhere.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.