
Abstract
Efforts are intensifying across the United States to better prepare physicians to deliver high-quality, patient-centered care for adults with disabilities such as autism. To address this need, we partnered with autistic adults and their families to develop a training program for resident physicians called Promoting Residents’ Excellence in Patient-centered cARE (PREPARE) for Autistic Adults. Here, we describe an evaluation of the feasibility, acceptability, and appropriateness of PREPARE for Autistic Adults to inform content and format revisions before efficacy pilot testing. We recruited residents (n = 14) at one large academic medical center in the Midwestern U.S. to participate in the 8-week virtual training, which included six pre-recorded lectures, six facilitator-led case studies, and two standardized patient encounters. Participants rated the feasibility, acceptability, and appropriateness of the training and participated in qualitative interviews to identify improvement opportunities. We analyzed quantitative data with descriptive statistics and qualitative interviews with an inductive rapid qualitative analysis. Participants’ median completion rate was 76.9% of training components. Participants rated feasibility, acceptability, and appropriateness highly. We identified four main qualitative themes: (1) flexibility facilitates feasibility, (2) high-value experiences increase acceptability, (3) practicalities affecting participation, and (4) high clinical practice relevance enhances appropriateness. We revised the training based on feedback, including clarifying or adding content, modifying standardized patient encounter logistics, and adding optional components for residency programs to supplement core PREPARE content. These results provide information for continued refinement of the training. Our next steps include pilot testing the efficacy of the revised training at one large academic medical center.
Community Brief
Why was this program developed?
Autistic adults get worse health care than non-autistic peers. It is hard for them to find doctors who know about autistic adults. Doctors often do not learn about autistic people in school. If they do learn about autistic people, it is often about recognizing autism in children, not how to care for autistic adults. We worked with autistic adults and their families to develop a training program on caring for autistic adults.
What does the program do?
The 8-week training program includes recorded presentations and online meetings with instructors and autistic people. It teaches about caring for autistic adults, including new ways to think about disability, working on a team, including patient in the team, improving communication, accommodating patients, and being respectful to patients and supporters.
How did the researchers evaluate the new program?
Fourteen doctors-in-training from one University took the training. We examined how much of the training they completed. Participants rated the training on how easy it is to do, how much they liked it, and how relevant it was. Participants also recommended improvements in qualitative interviews.
What were the early findings?
Participants felt the training was easy to do, likable, and relevant. In our feedback interviews with participants, we identified four main themes. First, participants said having different options to schedule made the training easier for them to participate in. Second, participants said hearing from autistic adults and practicing in a safe environment made the training worthwhile. Third, participants identified ways we could improve the training by providing more information and making it easier to find resources. Fourth, participants said the information was new to them and applied to real-world patient care.
What were the weaknesses of this project?
We conducted this study at one University, which limits how widely our results apply to all doctors-in-training. We do not know whether the people who chose to participate were more interested in working with autistic adults than the people who did not participate or if some people only participated because they were paid. In contrast, participants took this training outside of their regular training hours. If this training was part of the regular curriculum, our findings may have been different. Future studies should test the training when it is part of their regular curriculum.
What are the next steps?
We changed the training based on participants’ feedback by adding information, making it easier to find resources, increasing time for the mock patient appointments, and adding optional training experiences. Next, we will test how the modified training affects participants’ confidence, attitudes and beliefs, and knowledge about providing care for autistic adults. Then, we will make the training materials freely available on our website.
How will this work help autistic adults now or in the future?
In the long term, we expect this work will increase the number of doctors who are willing and able to provide care for autistic adults. We hope that this will improve autistic adults’ access to high-quality care and therefore their health.
Introduction
National organizations recognize the need to better prepare physicians to meet the health care needs of the over 44.1 million Americans with disabilities. 1 In the United States, aspiring physicians must first complete a bachelor’s degree (often about 4 years of coursework) before enrolling in a 4-year, doctorate-granting medical school. 2 Medical school typically includes 2 years of coursework and 2 years of clinical rotations. After medical school, aspiring physicians apply to residency programs, which provide post-doctoral clinical training in a certain specialty. Resident physicians in the United States are post-doctoral physicians who have completed medical school and are training to become specialists. While resident physicians are expected to demonstrate respect and responsiveness to diverse patient populations, including those with disabilities, there is not currently a disability training requirement for residency programs. 3
In a recent letter, 4 the U.S. National Council on Disability advocated all accredited residency programs should “adopt and implement disability cultural competency training to ensure that physicians are prepared to meet the health needs of people with disabilities.” They also suggested disability trainings incorporate the Core Competencies on Disability Health Education, 5 which establish the baseline expertise for providing quality care for patients with disabilities. Organizations are actively addressing the need for disability training, as evidenced by the recent development of the National Roadmap for Disability-Inclusive Healthcare 6 and a 2025 American Council on Graduate Medical Education-sponsored conference on resident education for disability inclusive health care. Given this growing national momentum, residency programs need evidence-informed disability education content that can readily be deployed.
Autistic adults are one population of adults with disabilities requiring particular attention in medical education. Relative to non-autistic peers, autistic adults are twice as likely to have cardiovascular disease or diabetes and three times as likely to have mood or anxiety disorders. 7 These co-occurring health conditions are compounded by autistic adults’ high rates of unmet health care needs 8 due to barriers to accessing quality primary care.9,10 One of the biggest barriers is the scarcity of adult care physicians with training in providing care for autistic adults.11–14 Indeed, physicians frequently encounter autistic adults in their practice, but evidence suggests they have low self-efficacy in delivering care for autistic adults, have limited knowledge about autistic adults, and lack flexibility for accommodating autistic adults’ needs during medical visits.9,10,14
To address this training gap and need for disability-inclusive health care education content, we partnered with autistic adults and family members of autistic adults to develop an autism training for resident physicians, henceforth referred to as “residents,” in internal medicine (IM), family medicine (FM), and combined internal medicine and pediatrics (Med-Peds) programs. 15 The training, called Promoting Residents’ Excellence in Patient-centered cARE (PREPARE) for Autistic Adults, contains six modules aligned with the Core Competencies on Disability in Health Education. 5 Our research team chose to develop this training specifically for residents because (1) we could strategically target residency programs that train specialists and primary care physicians who are likely to encounter autistic adults in their practice and (2) resident physicians have protected didactic time but fully independent practicing physicians (called “attending physicians” in the United States) do not. Researchers have successfully developed autism trainings for resident physicians in developmental and behavioral pediatrics. 16 However, to our knowledge, no adult autism-specific training exists for residents. 14
Existing literature on health care professional-focused interventions17–20 suggests it is important for researchers to develop interventions that participants perceive to be feasible (i.e., can be successfully completed), acceptable (i.e., is aggregable, palatable, or satisfactory), and appropriate (i.e., is relevant, compatible, and fitting of participants’ needs). One way researchers evaluate participants’ perceptions of these attributes is through a “formative evaluation,” 21 which is the evaluation of educational materials (i.e., training content and format) for the purpose of improvement prior to widespread implementation. Weston and colleagues describe formative evaluation as happening in two stages. First, the data collection stage involves trialing the training and collecting feedback. Second, the revision stage involves modifying the training for improvement based on the results of the data collection stage. Formative evaluations have been useful for evaluating and improving medical education curricula 22 and for implementing health care innovations. 23
Our primary objective for this study was to conduct a formative evaluation of PREPARE for Autistic Adults, focused on evaluating residents’ perceptions of the feasibility, acceptability, and appropriateness of the training. Specifically, we sought to use mixed methods to understand which aspects of the training are well-received by participants and identify areas for improvement prior to pilot testing efficacy.
Emerging Practice
Training development
Figure 1 provides an overview of our process for developing PREPARE for Autistic Adults, which is informed by the Design Process for Quality Improvement Interventions. 24 We detailed our initial development process thoroughly in a prior publication. 15 In brief, we developed the training content with a paid advisory board of autistic adults and family members of autistic adults to ensure content aligns with what the autism community feels is the most important for physicians to know (Fig. 1, Step 1). Throughout this process, the research team developed prototypes of training components and distributed these to the board for review. In virtual online (i.e., via Zoom) meetings, the research team solicited suggestions from the advisory board to improve or change the content. The advisory board reviewed each training component at least twice.
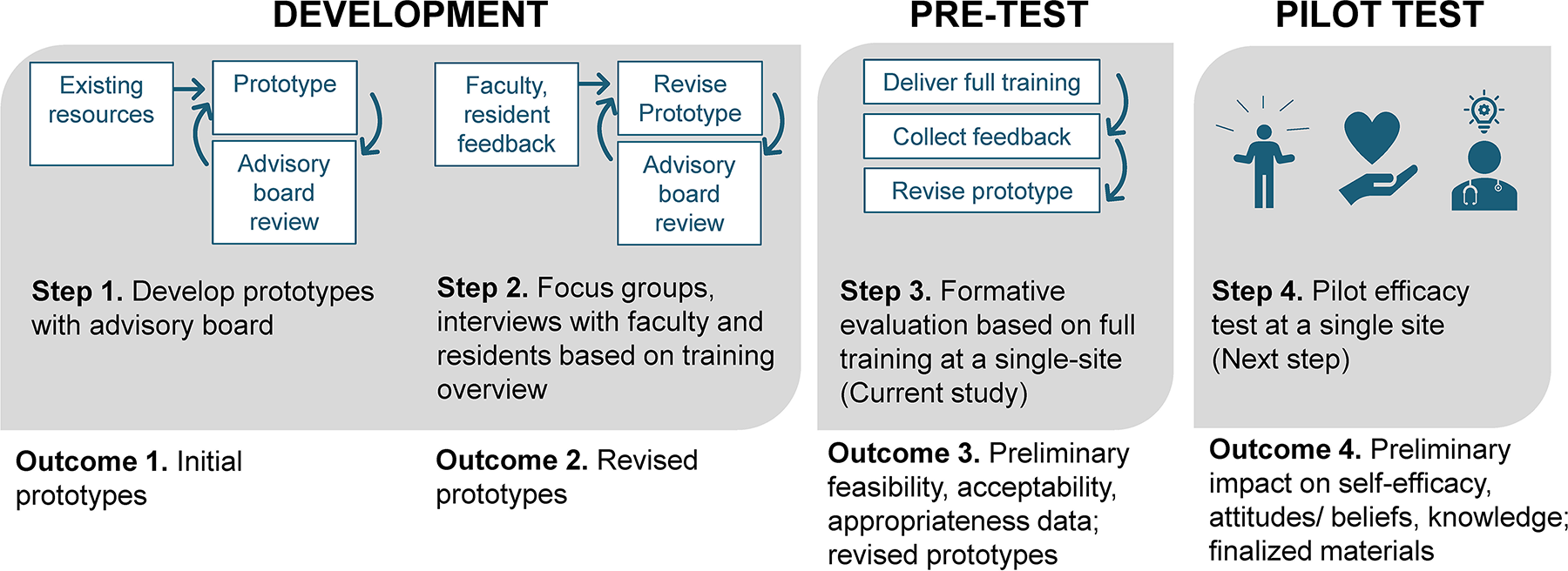
Overview of the development and initial testing of PREPARE for Autistic Adults. We reported Steps 1 and 2 in a prior publication. 15 The present article focuses on Step 3. This figure is informed by the Design Process for Quality Improvement Interventions. 24 PREPARE, Promoting Residents’ Excellence in Patient-centered cARE.
We also sought feedback from residents and faculty who educate residents based on a description of the training and a preview of one module (Fig. 1, Step 2). 15 Twenty-three residents and 14 faculty from 11 different institutions participated. Based on the feedback we received, we made several changes, including decreasing the duration of the prerecorded presentations and case studies, adding “clinical pearls” to the end of each presentation, ensuring the videos can be viewed at >1× speed, and offering a certificate of completion.
Training components
The core components of PREPARE for Autistic Adults are six modules and two standardized patient encounters. The six modules each consist of a 15-minute pre-recorded presentation and a 30-minute live case study with accompanying 2-minute “why is this case important” videos. 15 In the “why is this case important videos,” members of our advisory board share in their own words why a particular case is important to them or reflective of their lived experiences. The six modules parallel the six Core Competencies on Disability Health Education 5 : contextual and conceptual frameworks; clinical assessment; professional, patient-centered care; legal obligations; care over the lifespan and transitions; and team-based practice. The content covered in the pre-recorded presentations and case studies is further described in Supplementary Tables S1 and S2, respectively.
The training also includes two 20-minute standardized patient encounter experiences, where autistic adults are paid actors portraying a mock clinical case. These encounters consist of an interview to obtain information about the patient’s primary concern and establish a brief plan of care. In the first experience, an autistic adult who uses an assistive communication device presents to the clinic with a rash on their arms and hands. We provide photos of a rash on different skin tones for the autistic adult to select from and present to the resident. In this encounter, residents practice interacting with assistive communication device users and modifying care plans to accommodate patients’ sensory sensitivities. In the second experience, an autistic adult presents to the clinic for recurrent worsening migraines and is accompanied by a supporter who provides informal decision supports. In this encounter, residents practice collaborating with the autistic adult and supporter while identifying a care plan. At the end of the encounters, a faculty facilitator and actors provide feedback to the residents.
To maximize representativeness, the case studies and standardized patient encounters characterize autistic adults with heterogeneity pertaining to cognitive processing (i.e., average or above-average intellectual ability; mild, moderate, or profound intellectual disability), verbal communication (i.e., speaking, minimally speaking, and non-speaking), functional independence (i.e., those who live independently and those who live with supporters), and behavioral heterogeneity (e.g., self-injurious behaviors, difficulty transitioning activities, and sensory sensitivities). For example, one case study described addressing an abscess for a non-speaking autistic adult with a co-occurring intellectual disability, whereas another focused on caring for the cardiovascular health of a speaking, college-educated autistic adult with sensory sensitivities and a history of medical trauma. The case studies also reflect heterogeneity across racial groups, sex, gender, and sexual orientation throughout the curriculum.
Training delivery
In this study, we delivered PREPARE for Autistic Adults over 8 weeks (Supplementary Table S3). Since this was a research project, PREPARE for Autistic Adults was not embedded into protected educational time in the residency curriculum. This was a voluntary project that participants could elect to participate in outside of their current residency requirements. We sent weekly reminder emails or text messages to encourage participation in the assigned activities. We posted all materials in an online learning management system course designed with an accessibility expert. Residents viewed pre-recorded presentations asynchronously at their convenience.
Study team members led case studies synchronously via videoconferencing three nights per week to accommodate participants’ variable clinical schedules. Every Tuesday, Wednesday, and Thursday, a faculty facilitator logged onto the videoconferencing platform from 7:00 to 7:30 PM to lead the case study. Residents selected the night that worked best for them each week to attend. The facilitator used the “screen share” feature on the platform to share the case with residents. Residents also had the option of viewing the case study in the Canvas course or downloading it as a word document to follow along. The facilitator provided a brief overview of the case and then led the residents through the case study and discussion questions.
We conducted standardized patient encounters synchronously via videoconferencing with 10 minutes to engage with the standardized patient followed by 10 minutes of feedback. We offered multiple dates and time slots, and participants selected the option that would work best for them. At the selected date and time, a faculty facilitator, the standardized patient, and the participant logged into the videoconferencing platform. The faculty facilitator provided information about the logistics of the encounter and instructed the participant and standardized patients to begin. After 10 minutes, the facilitator indicated the encounter was finished and initiated the feedback portion. Autistic adult members of the PREPARE for Autistic Adults advisory board portrayed the patients in the standardized patient scenarios and were paid for their time ($30/hour).
Evaluation Methods
Study design
We conducted a formative evaluation to get feedback about feasibility, acceptability, and appropriateness from participants about the training content and format (Fig. 1 Step 3) prior to pilot testing efficacy. We used a single-site, single-group, mixed methods design to obtain feedback from participants on feasibility, acceptability, and appropriateness. We also examined participant completion rates as an indicator of feasibility.
Participants
We recruited residents from IM, FM, and Med-Peds programs at The Ohio State University. Collectively, these three programs train approximately 120 residents. Residency program directors or coordinators sent our study flier to residents through internal listservs. We also provided brief recruitment announcements at residency program meetings. Individuals who were interested in participating completed a secure online form providing their contact information and indicating their availability for participating in the training. We invited everyone who expressed interest in participating to participate.
While our long-term goal is to have PREPARE for Autistic Adults integrated into protected didactic time, for this study, residents participated voluntarily on their own time, outside their regular residency program requirements. Due to the time commitment outside of protected didactic time, participants earned an incentive of up to $250 each in the form of Amazon electronic gift codes as well as up to 5 hours of didactic credit from their residency program. We used a tiered incentive structure for this project, such that the more components of the training participants completed, the greater their incentive. We also sent participants a certificate of completion.
Measures
Our primary outcome measures were (1) feasibility, defined as the degree to which residents felt the training can be successfully completed; (2) acceptability, defined as the degree to which residents found the training agreeable, palatable, or satisfactory; and (3) appropriateness, defined as the degree to which residents found the training relevant, compatible, and fitting given their needs. We measured feasibility, acceptability, and appropriateness with the feasibility of intervention measure (FIM), acceptability of intervention measure (AIM), and intervention appropriateness measure (IAM), respectively. 25 The FIM, AIM, and IAM consist of four items each. Participants rated items 1–5, where median scores ≥4 generally indicate that an intervention is perceived to be feasible, acceptable, and appropriate.20,26,27 Previously established Cronbach’s alphas for the FIM, AIM, and IAM ranged from 0.85 to 0.91, indicating strong internal consistency, and test–retest reliability coefficients ranged from 0.73 to 0.88, indicating stability over time. 25 Researchers widely use the FIM, AIM, and IAM to evaluate health care professionals’ perceptions of the feasibility, acceptability, and appropriateness of interventions.17–20 We also examined participant completion rates, measured as percentage of each training component completed, as an additional indicator of feasibility.
Participants also completed a bespoke 17-item knowledge assessment we developed with our advisory board, 15 to further refine this measure. The knowledge assessment contains information from all six modules and is scored as percent correct. Consistent with other trainings for residents, 16 the knowledge assessment is comprised of multiple choice questions developed based on the goals, objectives, and key content from each module. Supplementary Data contains all measures.
Data collection procedures
Before the training, participants completed demographic questions and the knowledge assessment. During the training, we tracked completion rates by recording the percentage of pre-recorded presentations viewed, case studies attended, and standardized patient encounters completed by each participant. After the training, participants completed the FIM, AIM, and IAM to rate their perceptions of PREPARE for Autistic Adults as a whole and each training component and repeated the knowledge assessment. We invited all participants to complete a 15–35-minute (mean = 22.9 minutes) post-training interview via videoconferencing. Semi-structured qualitative interviews, conducted by authors BH or DG, were recorded and later transcribed. Interview guides (Supplementary Data) included primary questions, probing follow-up questions, and prompts. Our questions elicited additional information from participants about feasibility, acceptability, and appropriateness to add context and depth to our quantitative findings (e.g., “How feasible do you think [this training] is?”; “How difficult was it to participate in this training?”; “How well do you think this training would meet the needs of residents?”; “What could be done to make the training more feasible to do?”).
Data analysis
We analyzed quantitative data with descriptive statistics to characterize the participants, evaluate responses to the knowledge assessment, and summarize FIM, AIM, and IAM ratings. We analyzed qualitative interview data with a semantic-level, inductive rapid qualitative analysis using a postpositivist paradigm. This approach focuses on obtaining actionable, targeted qualitative data to inform understanding of facilitators and barriers of an intervention. 28 After prolonged engagement, BH and DG developed an initial codebook. Three coders (DG, DR, and HD) reviewed one transcript to assign segments of text to initial codes and considered the need for new codes. Coders met to discuss any new codes and update the codebook as needed. The coders independently used the updated codebook to revise previously coded transcripts as needed and code 1 to 2 new transcripts. The coders repeated this process until they coded all transcripts. Next, we evaluated cross-connections between codes to identify themes that bridged across our initial framework of codes as well as any relevant sub-themes. Last, we reviewed findings with the advisory board members to obtain their feedback on the changes proposed based on the interview findings.
Ethical approval
This study was reviewed and approved by the Institutional Review Board at The Ohio State University (#2022B0030).
Results and Lessons Learned
Table 1 contains information about participants’ demographic characteristics. Of the 35 participants who expressed interest in participating, 14 consented. Participants’ median completion rate was 76.9% of all training components (Table 1). Participants’ median completion rates were highest for standardized patient encounters (100.0%), followed by case studies (75.0%). Participants’ median completion rates were lowest for the pre-recorded presentations (58.3%), suggesting synchronous viewing, for example, prior to the corresponding case study, may yield greater completion of this component. Table 2 contains participants’ ratings of feasibility, appropriateness, and acceptability. The median participant rating on most FIM, IAM, and AIM items was 5 (highest possible score) for the training as a whole and for each of the individual components.
Participant Demographic Characteristics, Training Completion Rates, and Knowledge Assessment Scores
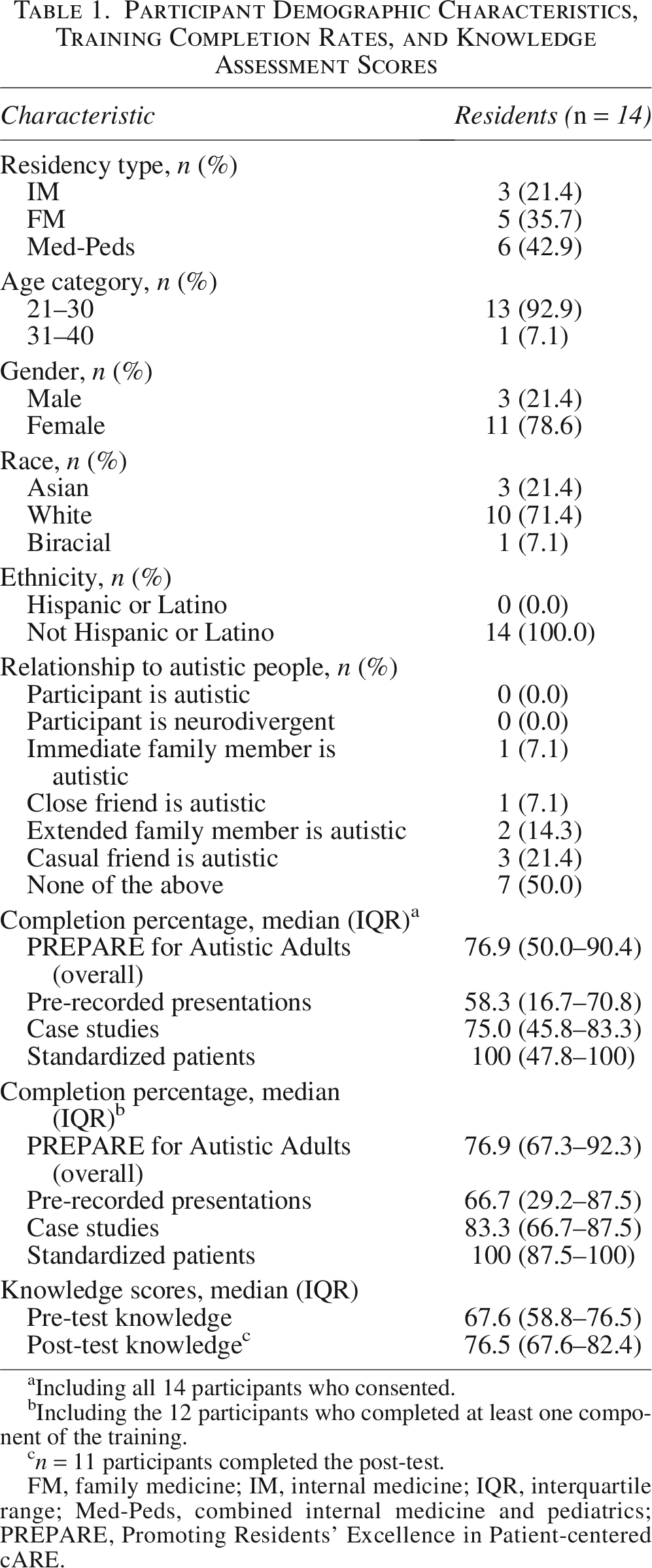
Including all 14 participants who consented.
Including the 12 participants who completed at least one component of the training.
n = 11 participants completed the post-test.
FM, family medicine; IM, internal medicine; IQR, interquartile range; Med-Peds, combined internal medicine and pediatrics; PREPARE, Promoting Residents’ Excellence in Patient-centered cARE.
Feasibility, Appropriateness, and Acceptability of the Training as a Whole and Individual Components Reported as Median (Interquartile Range)
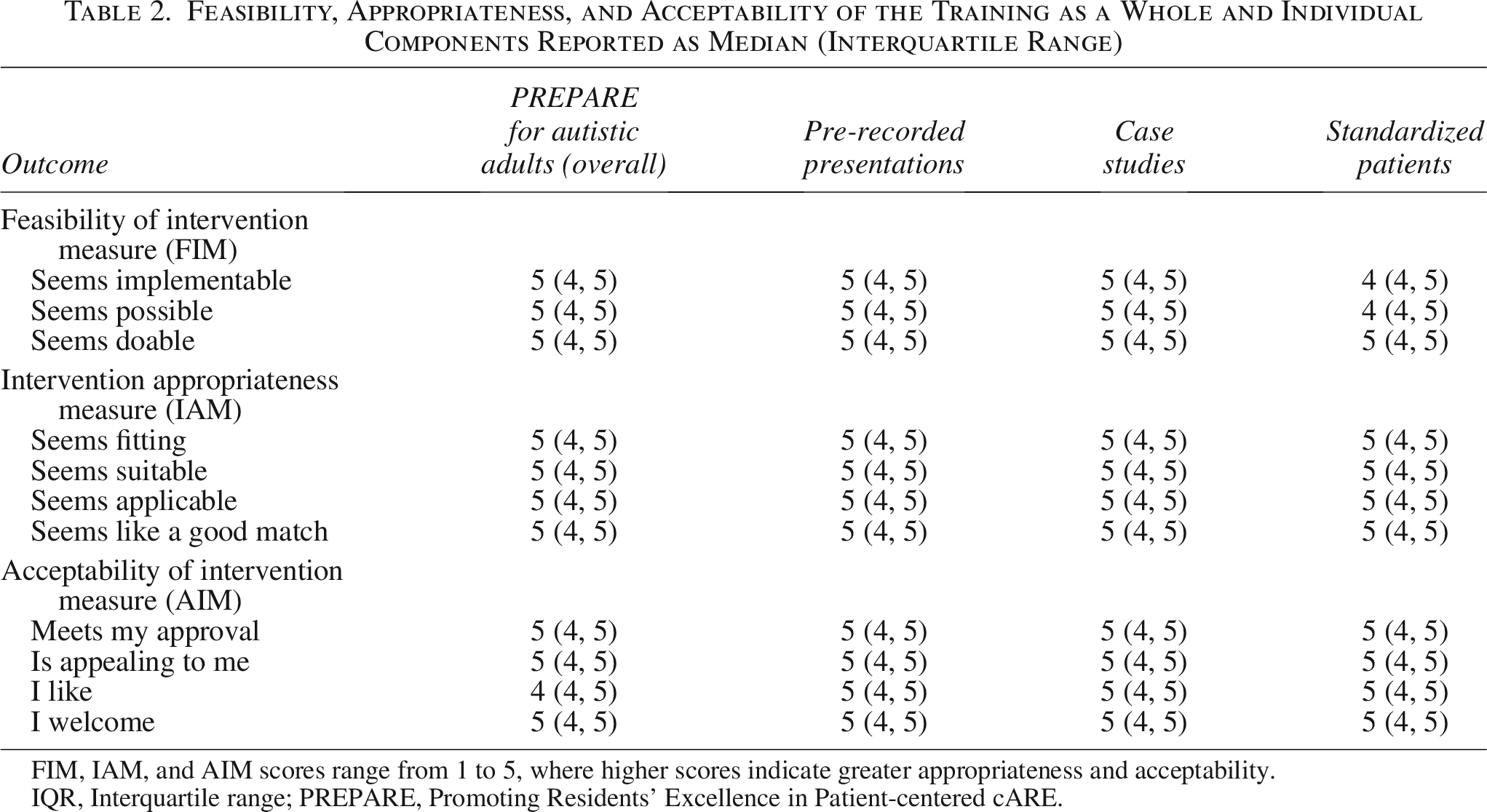
FIM, IAM, and AIM scores range from 1 to 5, where higher scores indicate greater appropriateness and acceptability.
IQR, Interquartile range; PREPARE, Promoting Residents’ Excellence in Patient-centered cARE.
When we examined responses to our knowledge assessment, we identified six questions that less than 55% of residents answered correctly at the post-test (Supplementary Table S4). As a result, we worked with our advisory board to review the wording of these items and identify changes that would improve clarity and/or to make content revisions to the training where needed.
We conducted semi-structured interviews with 11 of the 14 participants. Our qualitative analysis revealed four overarching themes and four sub-themes, described below. We summarize these themes in Table 3, along with resultant changes we made to the training.
Themes Summarizing Participants’ Experiences with PREPARE for Autistic Adults
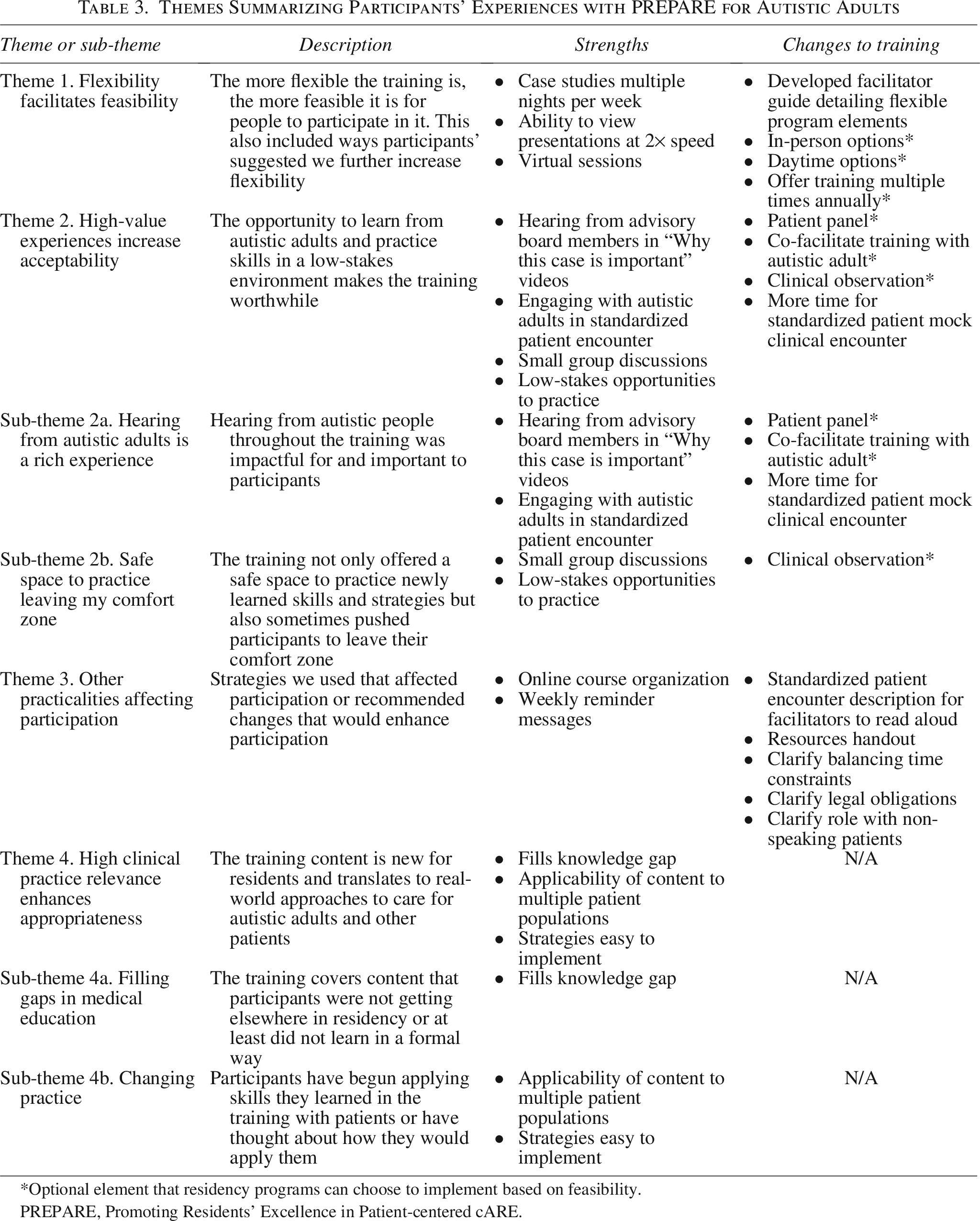
Optional element that residency programs can choose to implement based on feasibility.
PREPARE, Promoting Residents’ Excellence in Patient-centered cARE.
Flexibility facilitates feasibility
Participants can engage more easily when the training is flexible. Participants appreciated having multiple evenings per week as options for the case studies. One participant said, “I think you definitely provided plenty of times or options for times, which was, I think, crucial.” Additionally, although completion rates were lowest for the pre-recorded presentations, residents described appreciating the option to watch pre-recorded presentations asynchronously at up to 2× speed. Some participants wished for in-person sessions, but most felt keeping the synchronous components virtual would maximize feasibility. One participant said, “In terms of accessibility and […] making it easy for everyone to do, keeping it virtual is probably the best way to accomplish all of those things.” Participants also recommended having daytime options available to accommodate night shift schedules and offering the training multiple times annually to accommodate block schedules.
High-value experiences increase acceptability
Participants felt the opportunity to learn from autistic adults and practice skills in a low-stakes environment made the training worthwhile. This theme had two sub-themes, which we describe below.
Hearing from autistic adults is a rich experience
Participants said it was impactful to hear from autistic people throughout the training via standardized patients’ feedback and “why this case is important” pre-recorded videos. One participant recommended we “keep the personal touch of the patients with autism adding their perspective.” Regarding the “why this case is important” videos, one participant said, “I felt like I really liked those one or two minutes of, ‘This is why the thing that you’re learning about is really important when it comes to me and my life,’ because it provided insight.” In regard to the standardized patient encounter, one participant said, “It’s such a rich experience to work with someone on the spectrum who is willing and able [to provide feedback].” Pertaining to the duration of the mock clinical encounter, one participant said,
“In real patient rooms, we’re probably […] in a room for at least 15 minutes, minimum. And I know in med school, a lot of our encounters are 15 to 20 minutes with the patients and then 5 to 10 minutes of feedback. So I think you could probably extend the visit time […] and then shortening some of the feedback time. Because I feel like in my encounters at least, I don’t think feedback ever went the full 15 minutes.”
This indicated participants would welcome a longer duration of the mock visit time in the standardized patient encounter and that the duration of the feedback portion could be slightly reduced to accommodate this. One participant recommended adding a patient panel and another recommended more standardized patient encounters.
Safe space to practice leaving my comfort zone
Participants not only felt the training was a safe space to discuss and practice newly learned skills but also sometimes pushed them to leave their comfort zone. One participant said,
“I think the case studies offered an opportunity for implementation of […] those principles that had been discussed in the [pre-recorded presentations]. And I think that it was really valuable to be able to have a forum to sit down and talk through how we would [apply those principles], if and when they would come up in real life situations and patient scenarios.”
Another participant appreciated the small-group nature of the case studies and felt this contributed to their willingness to actively participate. Participants also frequently discussed the standardized patient scenarios in this sub-theme, describing them as “uncomfortable but definitely a good opportunity for growth.” Participants shared that most of their past experiences with standardized patient encounters were in the context of high-stakes medical licensing exams. They appreciated that this experience, in contrast, was meant to be a low-stakes opportunity to practice new skills and receive feedback.
Other practicalities affecting participation
Participants appreciated the online course organization and weekly reminder messages. They recommended adding a brief description of the encounter goals for facilitators to read at the start of each standardized patient encounter, with one participant suggesting,
“You could [say], “The primary goal is to observe your patient interaction, but also the expectation is to provide a brief assessment and plan proposal to the patient […] at the end.” So that people know it’s brief, and […] are focusing more on the patient interaction, but also recognizing that they’re supposed to treat this like a real clinic visit.”
Participants also recommended adding a handout of resources. Participants felt some topics or strategies were still unclear at the end of the training, and they recommended more information. For example, participants wanted more information on balancing time constraints in a busy clinic with patient-centered care, guardianship and capacity, and non-speaking patients.
High clinical practice relevance enhances appropriateness
Participants felt the training content was new to them and was relevant to their clinical practice, sharing how they have already applied the content in real-world care for autistic adults and other patients. This theme had two sub-themes, described below.
Filling gaps in medical education
Participants felt the training covered content they were not getting elsewhere in their education or did not learn in a formalized way. One participant said,
“We don’t learn a lot about caring for patients with autism […] in medical school. Sometimes our resident clinics don’t end up seeing very many autistic adults, so I think [residency] prepares us less. So, I do think everyone should do [PREPARE for Autistic Adults] […] I do think it would meet the residents’ needs really well.”
Another participant commented that they do not often see autistic adult patients in the resident clinic, but they feel this training will help them “address [autistic adults’] needs […] or accommodations they might need. And I probably didn’t know how to approach that before, especially with adult patients,” indicating content and skills taught in PREPARE for Autistic Adults had not already been covered in their education to-date.
Changing practice
Participants reported applying their new skills in their clinical practice or have thought about how they would apply them. One participant said, “I was able to draw parallels with the two patients that I have in mind that I see regularly in the clinic, and that is directly helpful to me to be able to address their health issues in a better way, in ways that I hadn’t thought about beforehand.” Another participant discussed how training content changed her approach to encountering autistic adult patients, saying, “I think having a controlled setting to practice […] asking questions to make sure I’m being sensitive to their needs first, and then starting your normal visit. I feel like it’s been incorporated into my introductory spiel when I first walk into a room.” Another participant said, “Generally I think it’s made me a better doctor as well, but a more sensitive, more patient-centered physician, regardless of which […] patient I’m taking care of.” Other participants noted the skills they have learned in PREPARE for Autistic Adults also apply to other patient populations, such as patients with dementia or other health conditions that affect their communication.
Discussion
In our prior work, we detailed the initial development of PREPARE for Autistic Adults based on: (1) our partnership with an advisory board of autistic adults and family members (Fig. 1, Step 1) and (2) feedback from residents and faculty across multiple institutions based on an overview of the training (Fig. 1, Step 2). 15 This study builds upon our prior work by delivering the entire training to residents at a single site and obtaining feedback to inform continued refinement of the training materials and format (Fig. 1, Step 3). Our results showed preliminary evidence that participants perceived PREPARE for Autistic Adults to be feasible, acceptable, and appropriate.26,27 Additionally, our findings highlighted important opportunities for improving this training to optimize residents’ learning experiences. While preliminary in nature, our findings also have some implications for contributions to the disability medical education literature.
Given that participants felt “hearing from autistic adults is a rich experience,” our findings illustrate the importance of hearing directly from patients in disability medical education. In other contexts, researchers have reported that learning from patients through patient panels,29,30 virtual encounters, 31 or recorded videos 32 has improved learner confidence, identification of additional training needs, and sensitivity to patients’ needs. Additionally, researchers have found that positive educational experiences may increase learners’ interest in pursuing FM 33 and improve attitudes about patients with disabilities. 34 PREPARE for Autistic Adults creates opportunities for residents to have positive experiences caring for and interacting with autistic adults. Findings from the theme “high clinical practice relevance enhances appropriateness” indicate these positive experiences may contribute to greater personal relevance of the training content for participants. As such, residency programs offering residents educational experiences where they can hear directly from autistic adults may ultimately foster a workforce of physicians who are willing and prepared to care for autistic adult patients in their future practice.
Our findings, particularly the sub-theme “safe space to practice leaving my comfort zone,” may illustrate the benefit of productive discomfort. House et al. assert that productive discomfort “cultivates an environment that challenges participants in a way that supports learning and personal growth.” 35 Productive discomfort has been shown to benefit medical trainees in other educational contexts, such as in anti-racism training 36 and developing adaptive communication skills. 37 While preliminary, our findings suggest that productive discomfort may also be beneficial in disability medical education.
Implications: changes to PREPARE for Autistic Adults
We made several content changes to PREPARE for Autistic Adults based on the results presented here. We developed a handout of resources for participants’ ongoing use even after completion of the training. We also clarified points in the pre-recorded presentations regarding the role of primary care providers in determining a patient’s need for guardianship. We added content to one case study to address how to balance time constraints with patient-centered care. Additionally, we developed a curriculum guide for faculty facilitators detailing core PREPARE for Autistic Adults elements and highlighting flexible options for implementation based on residency program needs (e.g., total number of sessions; virtual or in-person learning; synchronous or asynchronous options).
We also changed some standardized patient encounter logistics. For example, we wrote a brief description of the encounter goals and duration for facilitators to read to residents at the start of each standardized patient encounter. We also altered the distribution of time, increasing the mock clinical scenario from 10 to 15 minutes and decreasing feedback from 10 minutes to 5 minutes.
Finally, we added optional elements or learning activities that residency programs can offer to supplement the core PREPARE for Autistic Adults training components to increase the representation from autistic adults. These optional elements include (1) hosting a panel discussion with autistic adults and family members of autistic adults; (2) arranging observation of an experienced clinician caring for an autistic adult patient in the clinic (with patient permission); and (3) partnering with an autistic adult to deliver the training. These components are optional due to added logistical considerations that we felt were best left up to individual programs to evaluate for feasibility.
Limitations and next steps
The generalizability of our results to other residency educational contexts is attenuated by several key factors. We completed this study at a single institution with a small sample size. Participants in this study volunteered to participate in this research project outside of their protected educational time, introducing self-selection bias. The self-selected nature of participation and use of incentives may overestimate participation in other contexts. For example, residents with an established interest in working with this population may have been more likely to participate. However, our completion rates may also be conservative estimates, as participation in this study was outside of residents’ protected educational time rather than being an embedded component of the curriculum. Future research is needed to test the feasibility, acceptability, and appropriateness of PREPARE for Autistic Adults when it is embedded into protected educational time.
Recognizing the limited scope of this study, future studies are warranted. First, we recognize that efficacy testing was beyond the scope of this study but is an important next step. We are conducting an efficacy pilot study with IM, FM, and Med-Peds residents at The Ohio State University to evaluate the effects of PREPARE for Autistic Adults on residents’ self-efficacy, attitudes and beliefs, and knowledge about providing care for autistic adults (Fig. 1, Step 4). Additionally, multi-site trials of this training are also an important, necessary future direction to robustly evaluate the efficacy and effectiveness of PREPARE for Autistic Adults on residents’ outcomes. Second, having autistic physicians or residents evaluate PREPARE for Autistic Adults was beyond the scope of this study but would provide valuable insights to training content or delivery. Finally, we recognize this training is specific to autistic adults and does not address medical education for other populations with disabilities. Given the need for disability medical education more broadly, researchers may wish to explore developing new or adapting existing disability curricula to focus on adults with other conditions or disabilities in the future.
Conclusions
We are developing PREPARE for Autistic Adults to meet the U.S. national priority to improve U.S. physicians’ preparedness to deliver disability-informed health care.4,38 In this study, we reported participants’ favorable perceptions of the feasibility, acceptability, and appropriateness of this novel training, which we developed in partnership with autistic adults and family members of autistic adults. We conducted a formative evaluation of this training at a single site, focused on obtaining feedback from participants to improve the training content and format. Ultimately, we expect that these changes will increase the feasibility of residency programs using this training in the future, after efficacy and effectiveness testing is completed and the training is further refined.
Footnotes
The authors wish to acknowledge the incredibly valuable contributions of our advisory board members: Gyasi Burks-Abbott; Carolyn Harper-Munnerlyn; Ace Patrick Unruh; Jennifer Strobel; Amy Hwa Frechette, BA; Cindy Molloy; Nicole LeBlanc; Jennifer Samuel; Sal Silinonte, Consulting Autistic. We also wish to acknowledge Anne Longo for her assistance with a literature review for this article and Janet Childerhose, PhD for reviewing a draft of this article. A preprint of an earlier version of this article is available at ![]() .
.
Author Disclosure Statement
B.H. receives consulting fees for a federally funded project to improve treatment of attention deficit hyperactivity disorder for autistic people, receives payment and travel reimbursement as a programmatic panel member for the Congressionally Directed Medical Research Program (CDMRP) Autism Research Program, and has received travel reimbursement from the National Down Syndrome Society. The authors report grants from CDMRP, the National Institutes of Health, and the Patient-Centered Outcomes Research Institute.
Funding Information
This project was supported by grant number #W81XWH-22-1-0248 from the Department of Defense and the National Center for Advancing Translational Sciences of the National Institutes of Health under Grant Number UM1TR004548. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Department of Defense or National Institutes of Health.
Authorship Confirmation Statement
B.H.: Conceptualization, investigation, writing—original draft, project administration, and funding acquisition. D.G.: Investigation, formal analysis, and writing—review and editing. J.M.H.: Conceptualization, formal analysis, and writing—review and editing. D.R. and H.D.: Formal analysis and writing—review and editing. PREPARE for Autistic Adults Advisory Board: Conceptualization and investigation. L.J.: Conceptualization and writing—review and editing. C.H.: Conceptualization, investigation, and writing—review and editing. S.M.H. and D.C.: Conceptualization, investigation, and writing—review and editing
Prior Presentations
We presented preliminary findings at the International Society for Autism Research, Gatlinburg Conference, Society for General Internal Medicine, North American Primary Care Research Group Annual Meeting, Health care Transition Research Consortium Annual Conference, and the Association of Program Directors in Internal Medicine Fall Meeting.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.