
Abstract
Community Brief
Why is this an important issue?
Research shows that autistic people experience poorer mental health than non-autistic people. Autistic people have reported feeling they must mask or hide that they are autistic which is connected to poorer mental health. Autistic people also state that masking can make it difficult for them to feel comfortable being themselves. This study explores if negative mental health issues may be because masking makes it harder for autistic people to have or form a steady and comfortable identity.
What was the purpose of the study?
This study aims to learn whether autistic people or non-autistic people had more fear or confusion around their identity and whether they felt able to be themselves. It explores how negative emotions around identity may increase the number of autistic people who face mental health issues.
What did the researcher do?
The researcher used an online survey that asked people about masking, identity distress, identity conflict, and mental health. In total, 139 autistic people and 133 non-autistic people completed the survey. The researcher used three kinds of analysis as follows: analysis of covariance (ANCOVA) to learn which group had more identity distress, conflict, and poorer mental health; mediation analysis to see if identity distress explains the relationship between masking and mental health; and moderation analysis to see if identity conflict increases or decreases the relationship between masking and mental health.
What were the results of the study?
The researcher found that autistic people had more distress and conflict around their identity and poorer mental health than non-autistic people. In autistic people, masking only had a relationship with poorer mental health through its relationship with identity distress. In non-autistic people, identity distress and masking both led to poorer mental health independently. Finally, identity conflict relates to more identity distress, more masking, and worse mental health, but it does not make the connections between them stronger.
What do these findings add to what was already known?
These findings show that identity has a big impact on the lives of autistic people and that increased issues with identity may be causing mental health challenges. Autistic people are not always able to stop masking because it is often used to protect themselves from stigma and discrimination; as a result, learning more about the relationship between masking and identity may help us better support autistic people.
What are potential weaknesses in the study?
The participants in both groups were mainly White, meaning some findings may not represent the experiences of people of color and the impact of race and ethnicity on identity. It would be helpful to have more diverse participants and a larger number of participants.
How will these findings help autistic adults now or in the future?
This study shows that identity is very important in helping to understand mental well-being in autistic people. This study supports moving away from teaching autistic individuals to hide their autistic characteristics and toward humanizing approaches that encourage them to explore their identity as autistic people.
Introduction
Most autism research has been oriented through the medical lens, 1 which frames autism as a series of deficits to be corrected or cured. 2 This approach has perpetuated assumptions that autistic people lack social interest 3 or empathy, 4 and, as a result, poor mental health,5,6 unemployment, 7 and suicidality 8 are often treated as inherent features of autism, rather than outcomes shaped by societal factors. 9 Scholars working from the social model of disability contest this, highlighting autism as a natural variation of human diversity and emphasizing that many challenges autistic people face are the product of systemic exclusion.10,11 How autism is defined, diagnosed, and treated all remain heavily shaped by social forces and medicalized perspectives of disability.12,13
These forces are deeply informed by neuro-normativity, best defined as a set of standards or norms that are regarded as the benchmark for functioning and have become synonymous with neurotypical ways of thinking, behaving, and communicating.14,15 Individuals who do not meet these very particular expectations are widely ostracized, pathologized, and dehumanized. Milton 16 argues that the perceived majority defines and constructs our idea of “normal,” which fails to capture diversity. Normativity becomes an ideal that inaccurately labels those who fall outside the standards and norms of society as defective rather than different. 17 Neurodivergence is then regarded as innately wrong and maladaptive rather than socially constructed. 17 This prioritization of neurotypical standards creates pressure for autistic individuals to suppress their authentic selves, potentially contributing to significant psychological distress—mainly through the process of masking.
Masking is a phrase used by the autistic community to encompass the various conscious and unconscious strategies used by autistic people to conceal autistic traits and fit in. 1 Although clinical literature often uses the term “camouflaging,” many reject this language due to its pathologizing implications. 18 Hull et al. 19 found that autistic people reported using masking to assimilate into social groups, make interpersonal connections, and avoid social exclusion or discrimination. Autistic people report that masking strategies are a survival mechanism used to protect themselves against disproportionate exposure to victimization. 20 It serves as a social survival strategy, especially in environments where neurotypical norms dominate, wherein autistic people modify behavioral presentation temporarily, which results in dissonance between their outward presentation and internal experience. 21 While masking can help navigate immediate social situations, it is associated with longer-term psychological costs. 18
Pearson and Rose 18 found that while masking can help autistic people navigate external threats such as bullying or discrimination, it can also lead to an increased risk of internal threats such as adverse mental health, burnout, and the internalization of stigma. 22 The external social cost of continued marginalization compounds this internal toll. For many autistic people, masking is not optional but necessary, creating a persistent disconnect between how they feel internally and how they are perceived externally. 21 This disconnect may not only exacerbate mental health challenges but also interfere with identity development, particularly when one’s sense of self must be suppressed to be accepted.
Psychological distress is significantly more common in autistic people compared with non-autistic people. 22 Cassidy et al. 8 identify suicide as the leading cause of premature death in the autistic community, and earlier studies have reported that 35% of autistic individuals report making plans or attempting suicide. 23 Autistic people are placed in a precarious position in which the stigma they face within society shapes not only how they view themselves but also their masking, exacerbating mental health difficulties. While research has demonstrated that stigma correlates with concealment of autistic traits, 22 little is known about how this concealment may shape the development and experience of identity over time.
Emerging qualitative research highlights the potentially disruptive nature of masking on identity formation. Participants in the study by Miller et al. 24 report feeling alienated from themselves, grieving a version of themselves they were never able to explore. One participant expressed, “I think I am very good at masking, so good I’m struggling to tell what’s mask and what’s not.” 24 This confusion underscores how prolonged masking may not simply alter behavior, but potentially distort self-perception and identity cohesion. Masking requires autistic people to shift away from their sense of self for safety, social connection, and acceptance. Autistic people report feeling pressured, expected, or forced to meet neuro-normative standards, inevitably impacting the way they seem to experience and understand their own identity. 18
In developmental psychology, identity formation is a critical process typically occurring during adolescence and early adulthood, but continuing throughout life. 25 It requires both exploration of possible selves (identity exploration) and eventual commitment to an integrated identity (identity commitment). 26 When this process is interrupted—by emotional distress, environmental rejection, or internalized stigma—it can lead to prolonged identity confusion, disengagement, and adverse mental health outcomes. 27 These mental health difficulties are strikingly similar to the adverse mental health outcomes associated with masking in the autistic community.
Two constructs commonly used to study disrupted identity are identity distress and identity conflict. Identity distress refers to psychological discomfort due to uncertainty or instability in one’s identity.28,29 Identity conflict refers to perceived incompatibility between aspects of the self—such as between one’s internal identity and the socially acceptable version of oneself performed in public. 30 These constructs are especially relevant in the context of autism, where masking requires constant shifts between social presentation and authentic experience. This repeated divergence may compound conflict and distress, especially when social feedback invalidates one’s identity.
Identity formation relies on contextualizing identity within close relationships, needing the consistency of the self and the meaning of one’s identity in relation to family and friends. 27 Autistic people frequently report masking across multiple contexts—including with friends, family, and in professional and academic settings.1,18 The continual suppression of meaningful traits across these environments can inhibit authentic identity development, especially in the absence of affirming relationships or safe spaces to explore who they are. Given that identity is shaped in relation to others, 27 autistic people who consistently experience social rejection or must hide parts of themselves may face particular difficulty in forming a stable personal identity.
While much of the current literature of autistic identity focuses on autistic social identity 31 —understanding autism in relation to group belonging—there remains limited research on personal identity development. Social identity seems to buffer against poor mental health outcomes. For instance, individuals with a strong sense of autistic identity report greater well-being and reduced social anxiety.6,31 However, the role of personal identity—the internal stable sense of self across time—has received comparatively little attention despite its importance in understanding distress and resilience. 27
Autism is not external to identity; for many, it is a foundational part of who they are. 17 If autistic people are denied the opportunity to explore and express this identity, mainly due to masking, the process of identity formation may be undermined. This is especially concerning given the links between identity disruption and outcomes such as low self-esteem, future uncertainty, 32 and suicidality.8,33
Understanding how masking interacts with identity development—particularly the constructs of identity distress and conflict—provides a critical next step in exploring the mental health disparities observed in the autistic population. Identity may not only be shaped by masking but may also be a key mechanism through which masking contributes to psychological distress. As such, exploring these interrelated factors offers insight into how to support autistic people better and affirm their identity development throughout their lifespan.
Aims
This study aims to center identity cohesion as a key component in the conversation around societal factors, masking, and mental health disparities in the autistic community. These concepts are examined through identity distress and identity conflict. Identity distress looks at the multifaceted nature of identity by exploring social (e.g., friendships, group loyalties) and personal (e.g., long-term goals, career choice) facets and the distress associated with them. Identity conflict explores how aligned individuals feel with their ideal selves and society’s expectations. Investigating the prevalence and interconnection of identity distress, masking, psychological distress, and identity conflict may help identify key factors driving elevated mental health challenges and suicidality and further assess whether masking disrupts identity formation in autistic people.
This study asks the following: (1) Do autistic people experience higher levels of identity distress, identity conflict, and psychological distress than non-autistic people? (2) Is the relationship between masking and psychological distress mediated by identity distress in the autistic or non-autistic samples? (3) Does identity conflict moderate the relationships between masking, identity distress, and psychological distress in the autistic or non-autistic samples? Identity distress was conceptualized as an internal psychological experience that may explain how masking leads to psychological distress, while identity conflict was treated as a contextual factor shaping the strength of this pathway. Identity distress reflects difficulty maintaining coherence and clarity in one’s identity,28,29 while identity conflict captures misalignment—between the self and one’s ideal self or societal expectations. 30 Given this distinction, identity conflict was hypothesized to moderate, not mediate, the relationship between masking and distress. This approach reflects the idea that autistic and non-autistic people may experience identity-related dynamics differently, allowing for meaningful comparisons.
Hypotheses
Based on the research questions outlined above, four hypotheses were formed to reflect the aims of this study as follows:
Autistic people will experience higher levels of identity distress, identity conflict, and psychological distress than non-autistic people. Identity distress will mediate the relationship between masking traits and psychological distress in autistic people, but not non-autistic people. Identity conflict will moderate the relationship in the autistic cohort, with higher levels of identity conflict predicting a stronger relationship between masking and identity distress. Identity conflict will moderate the relationship between masking and identity distress, between identity distress and psychological distress, and between masking and psychological distress with higher levels of identity conflict predicting a stronger relationship between the variables.
Methods
Community involvement
Autistic people were involved in all parts of this study, including a lay autistic consultant who reviewed the background research and completed the full survey to provide feedback. Their input led to a more inclusive range of gender and sexual identity options and improved clarity of survey language for accessibility. They also emphasized that identity and masking are shaped by intersecting identities and that future research could build on this study to explore how multiple forms of marginalization affect identity conflict and distress. These variables were noted as personally relevant and aligned with autistic community priorities. This feedback shaped both the demographic design and the study’s framing, supporting a more inclusive and community-centered approach.
Participants
We conducted an a priori power analysis using G*Power (3.1.9.7) to determine the minimum sample size (power = 0.80, α = 0.05, with a medium effect) to achieve statistical significance with independent-samples t tests between the autistic and non-autistic sample (N = 80). Initial demographic analysis revealed significant differences between autistic and non-autistic groups in gender, identity, and age. To account for these, an analysis of covariance (ANCOVA) was used to control for their potential influence on outcome measures. Power analysis (Cohen’s f = 0.25, power = 0.80, α = 0.05) indicated a minimum total sample of 158 and our analytic sample exceeded this (N = 272; autistic n = 139, non-autistic n = 133). Previous research that utilized complex models recommended a minimum sample size of 100 participants to achieve significance for moderated-mediation analysis. 34 Thus, 125 autistic and 125 non-autistic participants, totaling 250 participants, were established as the minimum sample size to conduct t tests and moderated-mediation analysis effectively, and it was also adequate in post hoc tests, as analysis shifted.
A total of 305 participants initially accessed the survey, and 279 completed it, yielding a response completion rate of 91.5%. We collected data from 279 autistic and non-autistic participants. Participants had to be over 18 years old and proficient in English. Participants could be clinically diagnosed (N = 72), self-identified (N = 53), on a waiting list for a clinical diagnosis (N = 14), or non-autistic (N = 133). Four participants selected “prefer not to say” regarding their autistic identity and were removed from the data, leaving 275 participants total (N = 275).
The autistic cohort reported an age range between 18 years and 63 years (M = 38.02, SD = 11.59), whereas the age range reported by the non-autistic sample was between 18 years and 85 years (M = 44.62, SD = 16.18). In addition to gender, ethnicity/race, sexuality, autistic identity, and income, the autistic cohort was also asked at what age they were diagnosed/self-identified as autistic and the recency of their diagnosis/self-identification. The age range for diagnosis/self-identification was reported to be between 3 years and 68 years (M = 32.49, SD = 13.05) (diagnosed in adulthood).
There was no limitation on a participant’s current geographical location to avoid restricting the sample; however, most participants were White and from North America and Europe. Demographic information, including gender, ethnicity/race, sexuality, autistic identity, recency of diagnosis, and income, is shown in Table 1.
Demographics
A dash (—) is used to indicate no responses (0) for this variable.
Participants were able to select multiple sexual identities; percentage does not add up to 100%.
Due to the increase of “bots” disrupting research, we took steps to counteract interference, 35 and a system to detect potential “bots” was created. The system included two flags: one that noted any improbable survey completion times (5 minutes) and the other that noted any unique identification codes that did not match the requested parameters. This system flagged 3 participants meeting both criteria who were removed, leaving 272 participants in total. Participant responses were reviewed for obvious patterns of inattention or low effort responding, and no concerns were identified.
Measures
Identity distress
We used the 10-item Identity Distress Scale (IDS), 28 which asks how recently participants have been distressed by issues like long-term goals, friendships, or values. Items are rated on a five-point scale (“not at all” to “very severely”), with higher scores reflecting greater identity distress (range: 9–45). A 10th item assesses duration of distress. Participants meeting the clinical threshold (≥21 on items 1–9 and ≥3 on item 10) were considered to have significant identity distress. Internal consistency was excellent for both autistic (α = 0.81) and non-autistic participants (α = 0.86). While the IDS has demonstrated strong psychometric properties in adolescent and adult populations, it has not been specifically validated for use with autistic adults. 28
Masking
The Camouflaging of Autistic Traits Questionnaire (CAT-Q) is a 25-item scale that measures social masking behaviors in autistic adults across three subcategories: compensation, masking, and assimilation strategies on a seven-point scale from “strongly disagree” to “strongly agree.” 36 Questions include items like “When I am interacting with someone, I deliberately copy their body language or facial expressions.” Scores can range from 25 to 175; while an official cutoff has not been published, Hull et al. 37 have recommended a threshold of 125. We used a composite score for the analysis, with subscales used to demonstrate between self-identified and clinically diagnosed participants. Internal consistency of the CAT-Q was excellent for the autistic participants (total: α = 0.90, compensation: α = 0.86, masking: α = 0.83, and assimilation: α = 0.81) and non-autistic participants (total: α = 0.92, compensation: α = 0.85, masking: α = 0.79, and assimilation: α = 0.90). The CAT-Q has demonstrated strong psychometric properties and has been validated for use with autistic adults. 36
Psychological distress
The Kessler-6 Non-Specific Distress Scale (K6) is a six-item scale that illustrates participants’ nonspecific distress and is used to assess the severity of mental health disorders by being particularly sensitive to relevant thresholds for clinical diagnosis. 38 The scale consists of six questions as follows: “During the past 30 days, about how often did you feel… nervous?… hopeless?… restless?” It utilizes a five-point response scale ranging from “none of the time” to “all of the time.” Higher scores on this test represent higher levels of psychological distress, with potential scores ranging from 6 to 24. 38 A score of 13 or more demonstrates the threshold for the existence of severe mental health concerns. Internal consistency for the K6 was excellent for the autistic cohort (α = 0.82) and the non-autistic cohort (α = 0.88). The K6 is widely used and has demonstrated validity in general adult populations, including some evidence for use in autistic samples. 22
Identity conflict
The Inclusion of Other in the Self Scale (IOS) 39 is a two-item visual scale used to assess perceived closeness. For this study, it was adapted to assess identity conflict, comparing “who I am” to “who I want to be” and to “who I think society wants me to be.” Participants chose from eight overlapping circle pairs (1 = no overlap to 8 = complete overlap). A composite score (range: 2–14) indicated identity conflict, with lower scores reflecting greater conflict. Cronbach’s alpha was acceptable for non-autistic participants (α = 0.74), but low for autistic participants (α = 0.42), suggesting possible differences in item interpretation. Although the IOS is widely used for relational closeness, its adaptation for this purpose has not been validated in autistic adults.
Procedure
We hosted the survey on Jisc Online Surveys (2024). A snowball recruitment method was used where advertisements for the survey were shared on social media platforms (Twitter, Instagram, LinkedIn, and Facebook), and participants were encouraged to share the advertisements with others who met the inclusion criteria.
We gave participants accessible information about the survey contents and then provided them with a consent form. To anonymize data, participants were asked to create seven-digit unique identification codes. Identification codes were used to find data should a participant wish to withdraw their data. The survey consisted of demographic information, including current age, race/ethnicity, gender, sexuality, income, autism diagnosis, age at the time of autism diagnosis, and recency of autism diagnosis. Participants were asked to complete the above four scales in the following order: IDS, CAT-Q, K6, followed by the IOS. We formatted the survey this way to reduce any potential emotional discomfort by placing the least potentially distressing scales first and last. The order of the measures was selected based on face validity and perceived emotional load. The IDS offers a structured but nondiagnostic way to assess identity-related distress, making it a suitable opening measure. The IOS, a brief and visually based item, was chosen as a less demanding closing item to help minimize participant fatigue or emotional strain. Upon completing the survey, participants were provided with support options such as mental health and crisis resources. Ethical approval was granted by the University of Stirling General University Ethics Panel.
Data analysis
The data were prepared and analyzed using R v4.4.1 (2024) by the lead author (T.M.B.), with guidance from the senior author (M.B.). Relevant statistical assumptions were tested prior to analysis. While minor deviations from normality were noted in some variables, visual inspection of Q-Q plots and histograms suggested that these were within acceptable limits. Given the relatively large sample size and the robustness of ANCOVA and t tests to moderate violations of normality, all planned analyses were conducted as intended. Total scores were calculated across identity distress (IDS), masking (CAT-Q), psychological distress (K6), and identity conflict (IOS) for the autistic cohort (includes all autistic identifying participants), the non-autistic cohort, the clinically diagnosed autistic cohort, and the self-identified autistic cohort (includes participants on a waiting list). No outliers were identified within the data. Removal of missing data was selected as best practice for this study due to the infrequency of missed responses (data missing completely at random-0.34% missed response rate). 40 Thus, cases were dropped where they were missing for particular analysis only. The minimum sample size was retained for each test, despite this.
Independent-samples t tests were used to determine if any differences existed between the self-reported clinically diagnosed autistic participants and the self-identified autistic participants across all four questionnaires to ensure consistency and reliability as one analysis group. The difference in identity distress, masking, psychological distress, and identity conflict between the autistic participants and non-autistic participants was then examined using ANCOVA across the total scores for the IDS, CAT-Q, K6, and IOS, as well as across all nine of the IDS independent identity domains and both of the IOS subscales. ANCOVA analyses were used to control for variation in age and gender between the cohorts.
To test the moderated-mediation model, we first assessed whether identity distress mediated the relationship between masking and psychological distress using Model 4 in PROCESS v4.2. 41 Separate analyses were conducted for autistic and non-autistic groups to allow for group-specific interpretation. This decision was both theoretical and methodological as follows: combining groups could obscure differences and increase the risk of Type II error. Mediation tested direct and indirect effects, followed by Model 59 to assess whether identity conflict moderated these pathways (see Fig. 1).
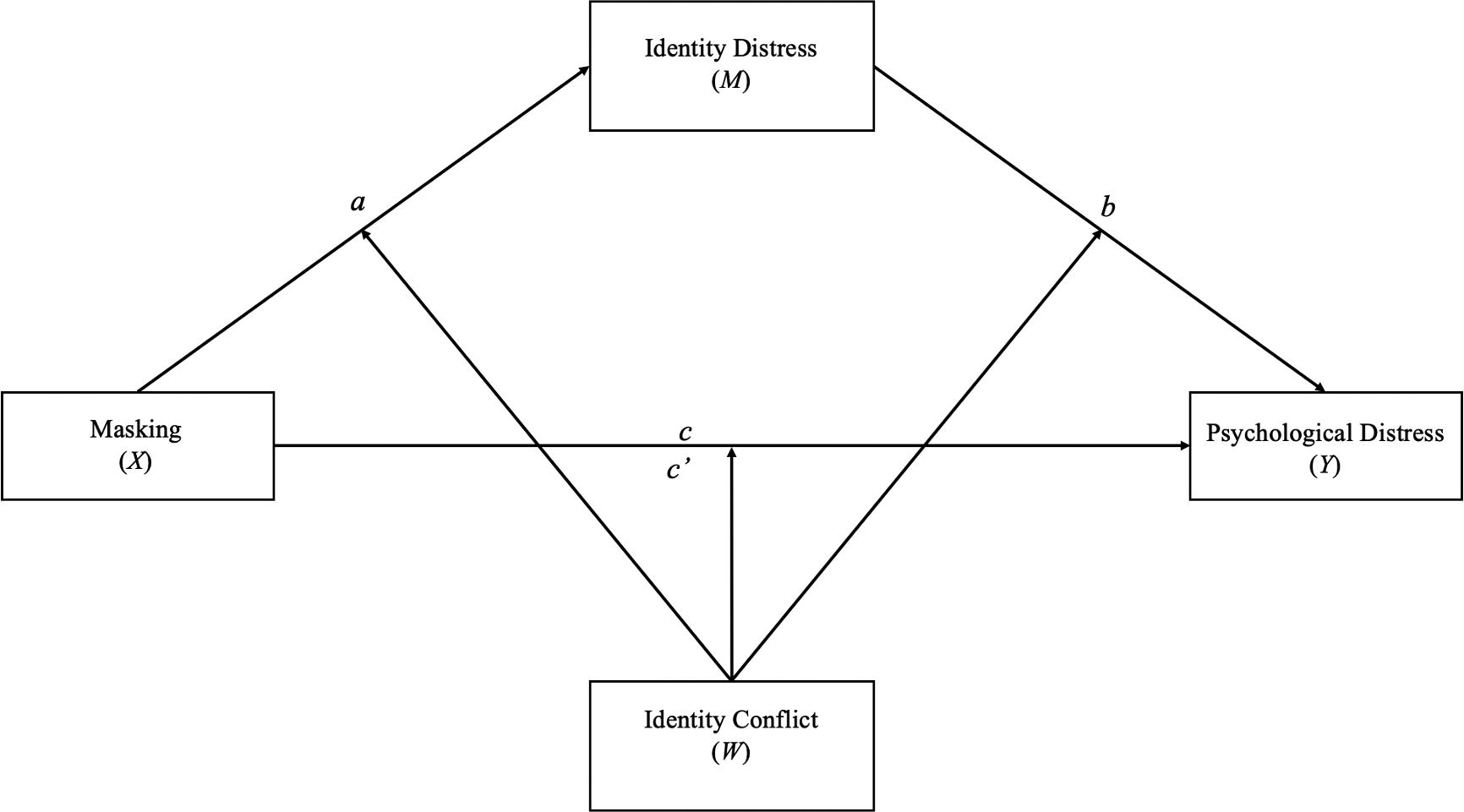
Moderated-mediation model (Model 59).
Results
Descriptive statistics
We calculated descriptive statistics for each of the scales. (Table 2). To better understand how prevalent severe levels of identity distress, masking, and psychological distress were within each cohort, thresholds and the number of participants that met the clinical or recommended thresholds for each variable were calculated. Of the autistic participants, 64 (46%) met the threshold (≥21) for severe identity distress, whereas only 17 (13%) of non-autistic participants met this threshold. In total, 122 (88%) of the autistic cohort met the threshold (≥125) for high-masking traits, while only 5 (4%) of non-autistic participants did. Finally, 117 (84%) of autistic participants met the cutoff (≥13) for psychological distress on the K6, indicating a higher likelihood of diagnosable mental illness compared with 56 (42%) of non-autistic participants.
Descriptive Statistics
We examined demographic differences between groups. An independent samples t test found significant differences between age; non-autistic participants (M = 44.62, SD = 16.81) were found to be significantly older than autistic participants ([M = 38.02, SD = 11.58], t(267) = −3.73, p < 0.001), while a chi-square test of independence found a significant difference in gender representation with more autistic people being gender diverse χ2(2) = 97.58, p < 0.001.
Preparation for ANCOVA: Autistic clinically diagnosed cohort and self-identified cohort
While previous research has demonstrated that there are typically no significant differences in autistic traits or characteristics between autistic people who are clinically diagnosed and those who are self-identified,14,42,43 we conducted t tests to ensure that there were no meaningful differences between the diagnosed (N = 72) and self-diagnosed autistic cohorts (N = 67). No differences were found between these cohorts across any of the variables. The results for these tests can be found in Table 3.
t Tests Between Clinically Diagnosed and Self-Diagnosed Cohorts
ANCOVA
Are there differences between autistic and non-autistic participants on identity distress, identity conflict, masking, and psychological distress?
ANCOVA was used to control for variation in age and gender between the autistic identifying participants (N = 139) and the non-autistic identifying participants (N = 133) across identity distress, masking, psychological distress, and identity conflict. We hypothesized that autistic participants would experience higher identity distress, identity conflict, masking, and psychological distress. These hypotheses were supported as autistic participants scored significantly higher than non-autistic participants on all major variables as follows: identity distress (F(1, 255) = 75.92, p < 0.001, η2 = 0.40), psychological distress (F(1, 260) = 88.87, p < 0.001, η2 = 0.36), masking (F(1, 257) = 249.53, p < 0.001, η2 = 0.20), and identity conflict (F(1, 261) = 90.11, p < 0.001, η2 = 0.27). These large effects highlight substantial group differences in masking-related experiences and their psychological impacts (see Table 4). While age was found to be a significant covariate across each ANCOVA, differences between the autistic and non-autistic population across identity distress, identity conflict, masking, and psychological distress remained significant, while controlling for age. Gender was not statistically significant in any of the models.
Analysis of Covariance Between Autistic and Non-Autistic Cohorts
p < 0.05.
p < 0.01.
p < 0.001.
Does identity distress mediate the relationship between masking and psychological distress?
Two mediation analyses were carried out to assess whether identity distress mediated the relationship between masking and psychological distress. The first model was conducted for the autistic cohort (N = 139), and the second was conducted for the non-autistic cohort (N = 133). The proposed relationships between each of these variables are illustrated in Figure 2.
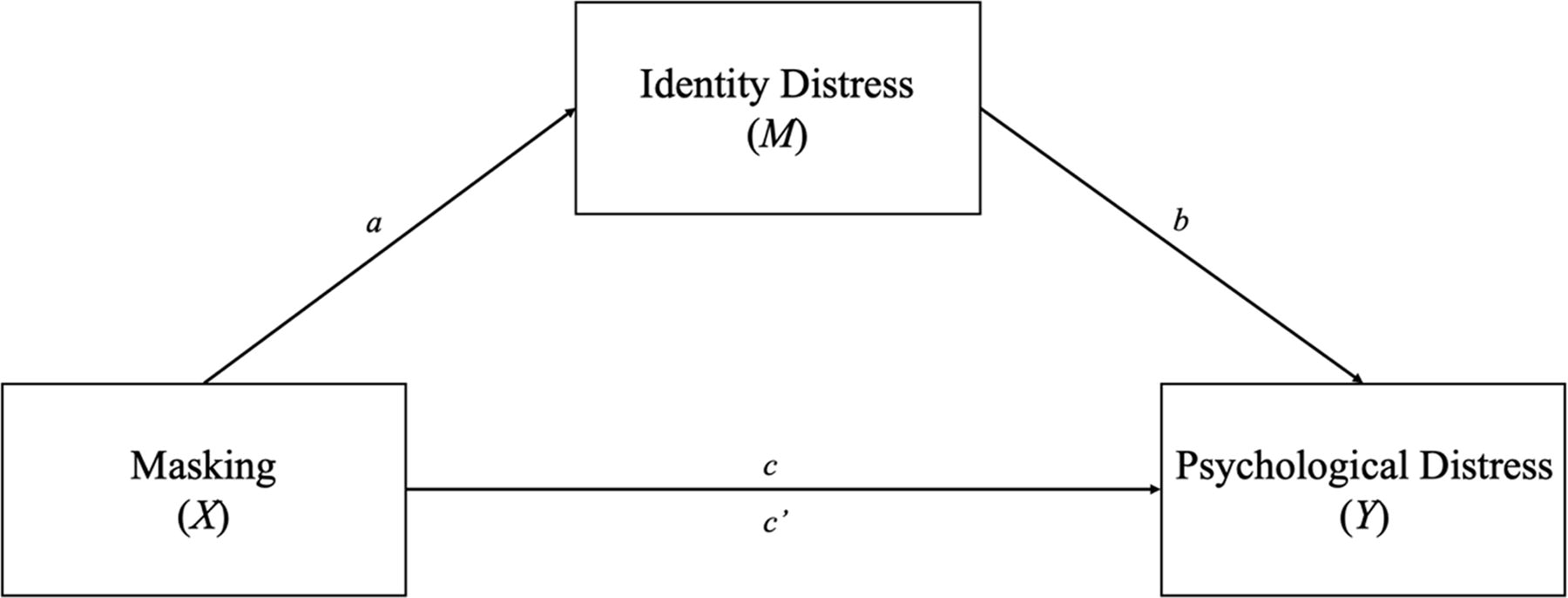
Mediation model.
In the first model, as hypothesized, the effect of masking on psychological distress was mediated by identity distress in the autistic population. When including identity distress in the model, the effect of masking on psychological distress decreased to non-significance (β = 0.06, p = 0.410). In the autistic cohort, mediation analysis revealed a significant indirect effect of identity distress on the relationship between masking and psychological distress (mean bootstrapped indirect effect = 0.18, 95% CI [0.08, 0.28], k2 = 0.18, indicating a moderate mediation effect). Identity distress represents a full mediation of the relationship between masking and psychological distress for the autistic cohort, such that the relationship between masking and psychological distress is no longer significant when accounting for identity distress. Figure 3 illustrates these pathways.
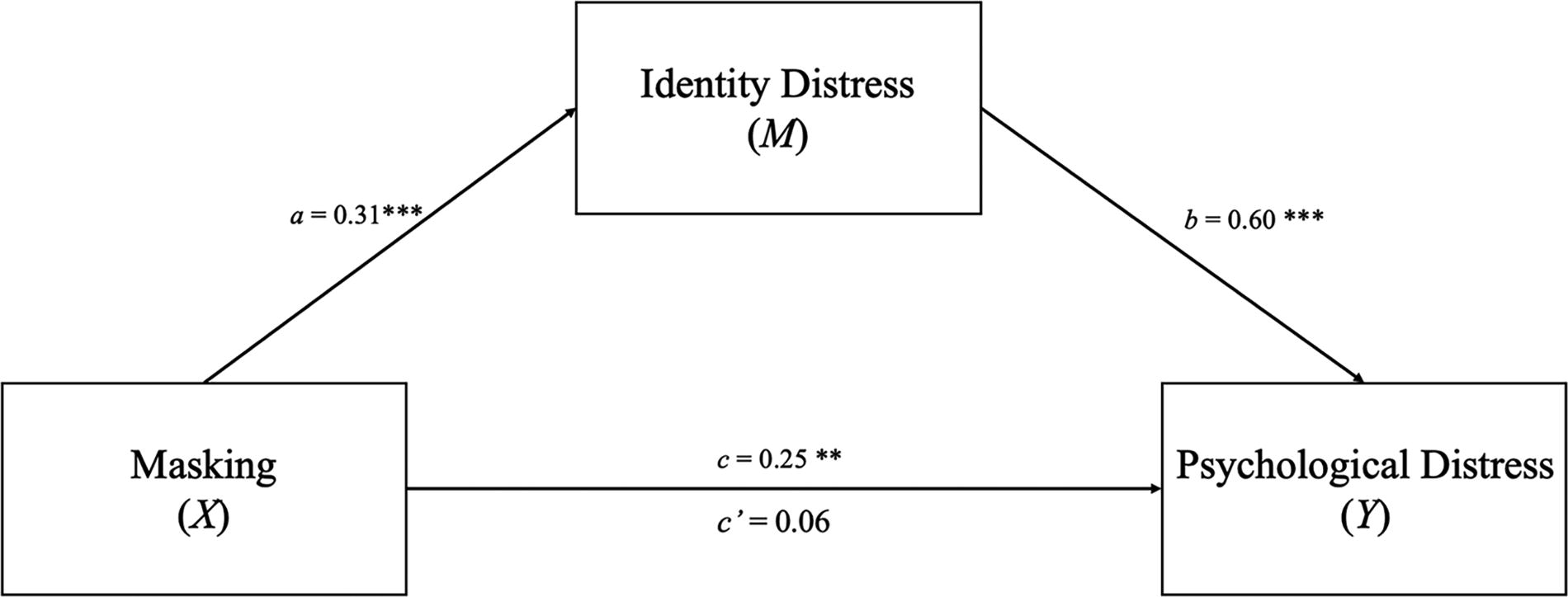
Autistic cohort mediation of identity distress on relationship between masking and psychological distress. ***p < 0.001, **p < 0.01.
In the model with non-autistic participants, the effect of masking on psychological distress was mediated by identity distress in the non-autistic population. In the model in which masking predicted psychological distress, the effect of masking was significant (β = 0.61, p < 0.001). When including identity distress in the model, the effect of masking on psychological distress decreased but remained significant (β = 0.31, p < 0.001). In the non-autistic cohort, identity distress partially mediated the relationship between masking and psychological distress (mean bootstrapped indirect effect = 0.30, 95% CI [0.21, 0.39], k2 = 0.50, indicating a moderate mediation effect). Identity distress represents a partial mediation of the relationship between masking and psychological distress for the non-autistic cohort. Figure 4 illustrates these pathways.
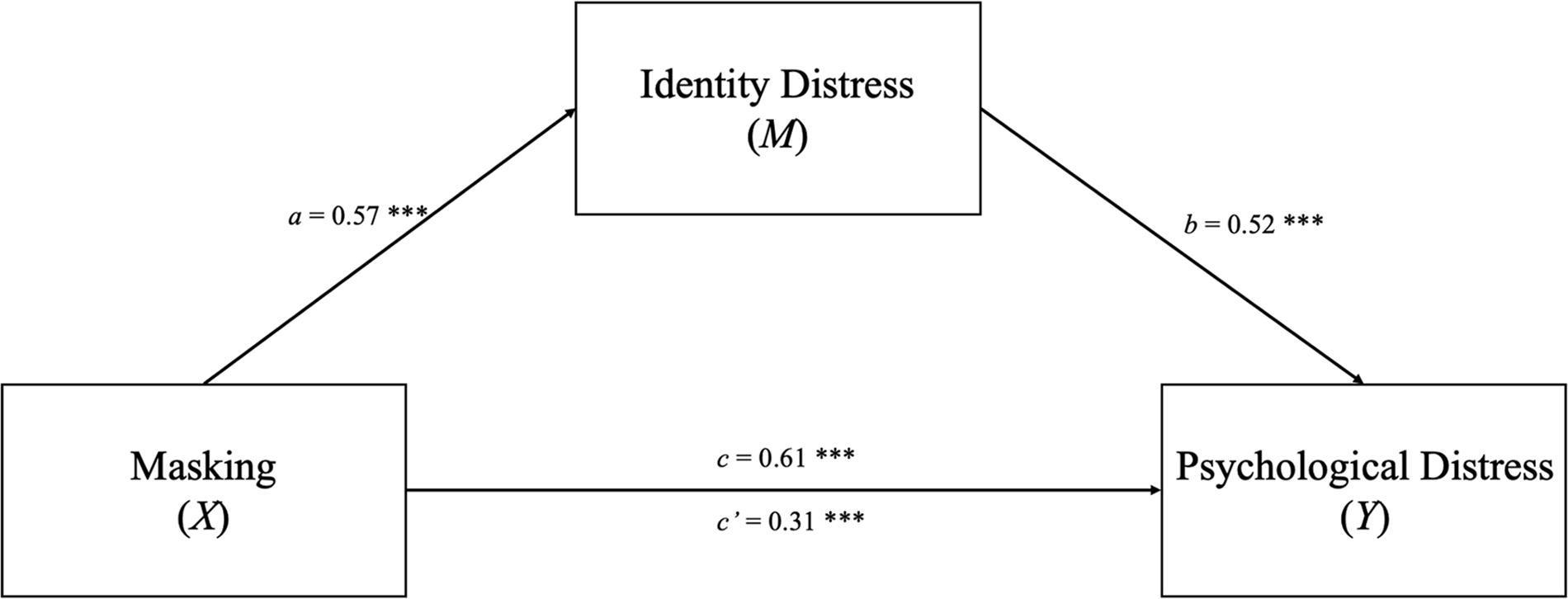
Non-autistic cohort mediation of identity distress on relationship between masking and psychological distress. ***p < 0.001.
Does identity conflict moderate the relationships between identity distress, masking, and psychological distress?
A moderated-mediation model was used to assess each part of the moderated-mediation models. The pathways being tested are illustrated in Figure 5. The models were run for the autistic participants and non-autistic participants separately. Identity conflict was not found to moderate any of the pathways in either cohort, but there were significant direct effects. The results are on display in Table 5 for the autistic cohort and Table 6 for the non-autistic cohort.
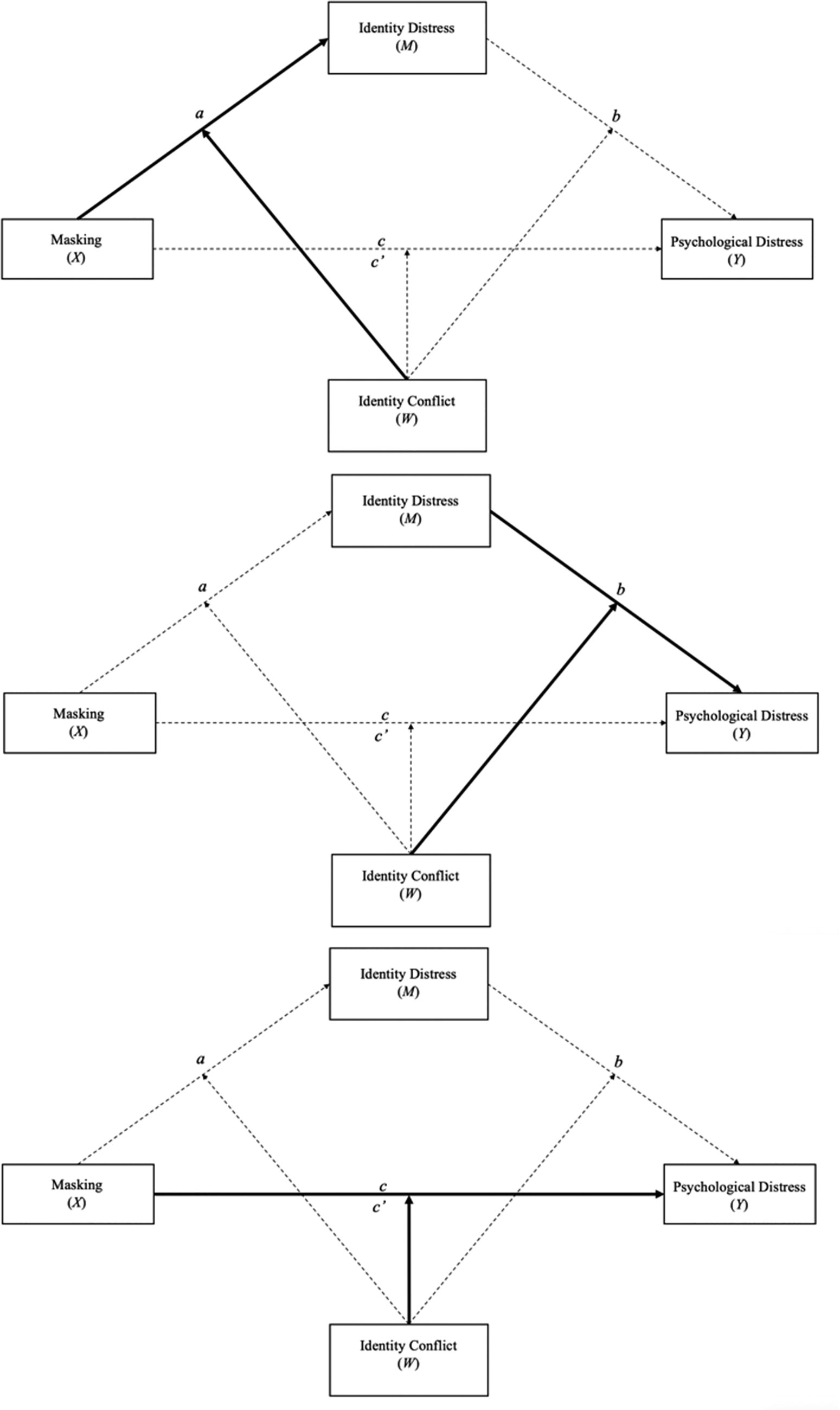
Moderated mediation model exploring moderation on each pathway. Note. Moderation of pathway a between masking and identity distress. Moderation of pathway b between identity distress and psychological distress. Moderation of pathway c between masking and psychological distress.
Autistic Participants
p < 0.01.
p < 0.001.
Non-Autistic Participants
p < 0.05.
p < 0.01.
p < 0.001.
Discussion
This study aimed to investigate the effect of identity distress on mental health outcomes and its role as a potential mediator between masking and psychological distress in autistic and non-autistic people. As predicted, autistic people were found to have significantly higher levels of identity distress, identity conflict, and psychological distress than non-autistic people. In addition, identity distress was found to represent a full mediation of the relationship between masking and psychological distress in the autistic cohort. However, identity distress was also found to partially mediate the relationship between masking and psychological distress in the non-autistic cohort. In addition, there was no moderating effect of identity conflict on any of the relationships between masking, identity distress, and psychological distress for either cohort. However, identity conflict had significant positive relationships with each variable, suggesting that it interacts differently with the model than we proposed.
Identity conflict and distress in autistic people as playing a role in poor mental health
Autistic people were found to have significantly higher levels of psychological distress compared with non-autistic participants. These findings are supported by a growing body of literature that indicates not only the prevalence of mental health difficulties in the autistic community but also the increased severity.8,22,44 In line with hypothesis one, autistic people were found to have significantly higher levels of identity distress than non-autistic participants demonstrating that identity distress is both more common and more severe for autistic people across both personal identity domains, as well as interpersonal or social domains. Autistic people also had less overlap between who they felt they were compared with who they would like to be, as well as who they felt they were compared with who they felt society would like them to be. This is further supported by findings that autistic people also experience higher levels of masking of autistic traits. These findings may show that despite feeling as though they are not meeting society’s expectations, many autistic people still feel unable to be themselves. This shows a potential double-bind where autistic people are losing authenticity through masking at significantly higher rates for the sake of acceptance, but feeling continually rejected by society.
Specific to hypothesis two, the direct effect between masking and psychological distress was no longer significant when identity distress was included in the autistic model. This suggests that masking is associated with psychological distress through its relationship with identity distress. Prior research has emphasized the impact of masking, including each of its subscales (compensation, masking, and assimilation), directly on negative mental health outcomes.1,8,19 This finding suggests that autistic people are experiencing more adverse mental health implications due to the relationship that exists between increased masking and increased identity distress rather than masking independently. This is a novel finding that may reframe our understanding of the issues that truly underpin the disproportionate rates of poor mental health in the autistic community. Despite being novel, this finding is supported tangentially by what is known about both the impact of masking on identity through qualitative research18,24 and the implications for identity distress and disturbance in the non-autistic population.28,45
This finding is significant and provides foundational knowledge for future research into thwarted belongingness. Cassidy et al. 8 found that assimilation-based masking strategies (adapting to try to fit in) were more widely associated with increased markers for suicidality; many autistic people found that assimilating increased their sense of otherness and resulted in disingenuous relationships, which contribute to feelings of thwarted belonging. Collectively, these findings suggest that there is a potential disturbance in the process of cohesive identity development for autistic people that is yet to be explored within literature and that it might contribute to mental illness. Future research should explore the factors that are maintaining this conflict as it may shed light on burnout, thwarted belonging, and suicidality. Specifically, the relationship between masking, identity, and belonging to better elucidate the complexities of only finding “belonging” when masking.
Similarly, the direct effect of masking on psychological distress remained significant when identity distress was added to the non-autistic model. However, identity distress increased the indirect effect of masking on psychological distress, representing a partial mediation of this relationship. This finding was contrary to the researcher’s hypothesis, but can likely be best understood through the concepts of identity salience and the role of masking in the lives of non-autistic people. Identity salience is the theory that facets of a person’s identity (race, religion) will become active in particular settings, and based on the relevance of those identity facets, there is a hierarchy of a person’s identities. 46 Within marginalized communities, the salience of identity is much more profound as “othered” identities put them at increased risk of discrimination and ostracization. Autistic identity permeates an individual’s entire life as they are often required to mask across almost all domains of their lives. 22 However, individuals who do not have facets of their identity that require constant vigilance likely are simply engaging in short-term impression management (pretending to be in a good mood at work on a difficult day). 47 Thus, short-term impression management may be less psychologically troubling for social majorities.
Finally, contrary to hypotheses three and four identity conflict did not moderate the relationship between masking and psychological distress mediated by identity distress, the relationship between masking and identity distress, or the relationship between identity distress and psychological distress for either cohort. However, identity conflict was found to have significant direct positive relationships with masking, identity distress, and psychological distress, which suggests it influences this model perhaps through mediation, explaining these relationships rather than influencing them which should be explored in further research.
Strengths and limitations
This study is the first, to our knowledge, to examine how masking disrupts identity formation in autistic people using the constructs of identity distress and identity conflict, contributing to research on identity and mental health outcomes in autism. A key strength was the involvement of an autistic community member and inclusion of both self-identified and formally diagnosed participants, supporting alignment with community priorities and the validity of self-identification.
However, limitations include the use of measures not formally validated in autistic populations and the low reliability of the adapted two-item IOS, particularly for autistic participants. The cross-sectional online design also limits causal interpretation and experimental control. Future studies should validate identity measures for autistic groups and build on these findings using more diverse longitudinal approaches.
Future directions
Intersectionality should be at the forefront of autism research to ensure that generalizable and accurate research is being conducted for the autistic community. 2 In the case of identity, the salience of identity, 46 the increased likelihood of identifying as more than one marginalized community for autistic people (based on gender, race, and sexuality), 21 and compounding minority stress 22 make intersectionality even more critical in this particular area of research. The impact of multiple minority identities and the compounding effects of normativity across multiple domains of identity make this an essential topic for appropriately supporting all autistic people with cohesive identity formation. Most strikingly, these findings align with what is already known about loneliness and thwarted belongingness and may provide an essential bridge between loneliness and suicidality. These findings provide insight into how vital recognizing personal and social identity is in the lives of autistic people, but further research is needed to tease apart how this knowledge can best be applied to supporting autistic people.
Conclusion
In conclusion, these findings have important clinical implications for mental health support that centers on cohesive identity development for the overall well-being and quality of life of autistic people. Understanding the far-reaching impact of difficulties with identity formation and the influence of masking on this process can help to continue to demonstrate just how dangerous the concept of neuro-normativity is in the lives of autistic people. Future research into loneliness and thwarted belonging, as well as the variation in both personal and social identity in this neuro-minority, may highlight essential avenues for not only clinical mental health support but also a much deeper understanding of why masking has such a significant negative impact on mental health. This research highlights that deficit-focused research continues to miss vital nuance that provides necessary avenues for societal change by working toward a missing link in how we discuss the complexities of masking. Masking remains both necessary for survival and dangerous for well-being, yet relevant due to the biased and harmful views perpetuated through research and retained within society.
Footnotes
Authorship Confirmation Statement
T.M.B.: Conceptualization, methodology, formal analysis, and writing—original draft. M.B.: Supervision, methodology, and writing—review and editing.
Author Disclosure Statement
No interests to disclose.
Funding Information
No funding was received for this article.