
Abstract
Background
The prevalence of Alzheimer's disease (AD) is rising in China. Although disease-modifying treatments are available, their efficacy is mostly seen in the early stage. Timely and accurate diagnosis is crucial for AD management.
Objective
This study aimed to describe the diagnostic trajectory, current treatments, and care burden for mild cognitive impairment (MCI)/AD in China.
Methods
Data were derived from the Adelphi Real World Dementia Disease Specific Programme™, a cross-sectional survey of neurologists, patients with MCI/AD dementia and their care partners, conducted in China from February–May 2024. Patient characteristics, diagnoses, treatments, and care were reported by neurologists and supplemented by self-reports from patients and care partners.
Results
Overall, 93 neurologists reported on 774 patients. Of patients with a Mini-Mental State Examination (MMSE) score at the time of survey (n = 699), mean (standard deviation) age was 69.3 (8.2) years, 49.6% (n = 347) female and most had MCI/mild AD (MMSE 20–28) at survey (52.5%, n = 367). Over one-third of patients presented with moderate to severe disease at initial consultation (34.7%, n = 203) and at diagnosis (36.2%, n = 265). Biomarker testing was infrequently used in diagnosis, with cerebrospinal fluid being the most used (11.2%, n = 81) and physician-reported challenges including cost, patient reluctance, and availability. Most patients received only non-professional care primarily from a partner/spouse and/or children, who spent up to 47.0 (45.8) hours per week caring.
Conclusions
Challenges in early and biomarker-based diagnosis were identified and care partners continued to experience a substantial burden. Continued efforts are needed to ensure the healthcare system's preparedness for the AD epidemic.
Keywords
Introduction
Alzheimer's disease (AD) is a progressive, neurodegenerative disorder, with the disease spectrum ranging from an asymptomatic phase at one end, through to mild cognitive impairment (MCI) and finally to mild, moderate, or severe dementia due to AD at the other end. 1 With an increasingly aging population, AD is becoming a greater issue in China, with the estimated age-standardized prevalence of AD and related dementias in 2019 being 788.3/100,000. 2
The diagnosis of AD has historically been based on routine neuropsychological assessments. Biomarker testing is increasingly being used to positively identify AD in patients. Testing is aimed at the putative causative elements of AD, amyloid-β and tau proteins, or other associated markers, and can be done in cerebrospinal fluid (CSF) or blood, or through positron emission tomography (PET). 3 However, barriers remain in real-world clinical practice to implement biomarker-based diagnostic testing for AD.4–6
In China, memory clinics serve as key specialized centers that identify patients at early stages of cognitive disorders (including MCI and mild dementia due to AD), offer timely treatment, and provide training and education for care partners and families. 2 Nevertheless, the number of memory clinics remains limited across China, with patients in the western region and rural areas facing greater barriers to access. 7 China's healthcare system employs a three-tier and three-grade hospital classification based on service provision, institutional size, medical technology, equipment, and quality of medical care.8–10 Tertiary grade-A hospitals represent the top of this hierarchy, characterized by the most advanced medical resources, infrastructure, and capability to provide cutting-edge clinical care. 10 Almost all memory clinics are established within tertiary hospitals, 11 which are the highest tier of hospitals in China 9 and where AD is predominantly diagnosed. 12 Yet, fewer than 10% of tertiary hospitals have a memory clinic. Among the tertiary hospitals with one, 75% can provide biomarker testing in CSF, but only 35% have the capacity to perform fluorodeoxyglucose-PET and less than 15% can conduct amyloid-β or tau PET. 13 Moreover, most biomarker testing (e.g., CSF and amyloid or tau PET) scans are not covered by public health insurance in China, and the high costs associated with PET scans may further hinder their use in clinical practice.
Although treatment of AD has historically been focused on managing symptoms only, disease-modifying treatments are now being approved for treating MCI due to AD and mild AD dementia.14,15 However, their use may be limited due to challenges in early diagnosis of AD, which is crucial for efficacious use of these treatments. The requirement for AD diagnosis to be confirmed through biomarker testing further limits the usage of disease-modifying treatments.
Lack of timely diagnosis and progression to more severe forms of AD may also increase the already substantial burden experienced by patients’ care partners. Barriers to timely diagnosis and effective use of biomarker testing in China, including patient fear of stigmatization, have been previously described. 16 However, no comprehensive study of the real-world diagnostic trajectory of Chinese patients with MCI or AD has been undertaken to date. In addition, knowledge about the impact on the quality of life of Chinese care partners of patients with AD, stratified by disease severity, is limited. 17 Therefore, this analysis aimed to describe the diagnostic journey of patients with MCI and AD dementia, use of biomarkers and treatments, and the burden on care partners in China by evaluating real-world data reported by physicians, patients, and care partners.
Methods
Study design
This study used data from the Adelphi Dementia Disease Specific Programme (DSP)™, a cross-sectional survey of patients with mild cognitive impairment or dementia, their care partners and treating physicians conducted in China between February and May 2024. The DSP methodology has been previously described,18,19 validated, 20 and demonstrated to be representative and consistent over time. 21
Eligible physicians were recruited from publicly available information by local agencies, and, following confirmation of eligibility, completed an attitudinal survey on AD treatment and diagnosis. Physicians were then requested to return demographic and clinical information for up to their next nine consecutively consulting eligible patients. Patients and their care partners were then invited to complete voluntary surveys on the impact of their AD. Care partners additionally completed standardized outcome measures.
Eligibility criteria
Physicians were eligible for inclusion in this study if they were neurologists, made treatment decisions for patients with cognitive impairment or explicit dementia/AD, and saw at least ten of these patients in a typical week who had not been admitted to a nursing home for an extended stay (defined as a period of three months or longer).
Patients were eligible for inclusion if they were ≥50 years of age, were not involved in a clinical trial at the time of survey and had a physician-confirmed diagnosis of MCI or dementia (excluding patients with purely vascular dementia or dementia caused by environmental factors). Care partners of patients included in the study were eligible for inclusion if they accompanied the patient to the consultation and were ≥18 years of age.
This paper focuses on patients with a diagnosis of MCI (encompassing amnestic/non-amnestic MCI due to either suspected AD or undetermined etiology, prodromal AD and predementia) or AD (AD, early AD, mixed dementia) at the time of survey.
Study measures
In addition to reporting their attitudes on AD diagnosis and treatment, physicians reported patients’ demographic and clinical characteristics. Clinical characteristics included symptoms, Mini-Mental State Examination scores (MMSE) at first consultation, diagnosis and time of survey, and concomitant conditions. Physicians also reported on patients’ diagnostic trajectory, including physicians involved, time to diagnosis, diagnostic tests used and the use of genetic and biomarker testing, in addition to treatments and care received by patients and time spent caregiving at time of survey.
Patients with an MMSE score of >10 to <28 at time of survey reported their reasons delaying their first consultation. Care partners reported their demographic characteristics, their own health conditions and completed the EQ Visual Analogue Scale (VAS). The EQ-VAS assesses the respondent's health state on a scale of 0 to 100, with 100 being optimal health. 22
Ethical approval
Data collection was undertaken in line with European Pharmaceutical Marketing Research Association guidelines 23 and the Declaration of Helsinki of 1964 and subsequent revisions. This study was granted exemption from ethical approval by the Pearl Institutional Review Board (#22-ADRW-172, #22-ADRW-173). Using a check box, patients and care partners provided informed consent to take part in the study. All data were aggregated and de-identified before receipt for analysis.
Data analysis
Data were stratified by disease severity defined by MMSE scores, as MCI/mild dementia due to AD (MMSE score ≥20 to ≤28), moderate dementia due to AD (MMSE score ≥10 to ≤19), or severe dementia due to AD (MMSE score <10). Only patients with available MMSE scores were included. Patients were stratified by MMSE at initial consultation, diagnosis, or time of survey as appropriate, see Figure 1 for groupings.

Study design and group sizes. AD: Alzheimer's disease; EQ-5D VAS: EQ Visual Analogue Scale; MMSE: Mini-Mental State Examination.
All data were analyzed descriptively. Mean and standard deviation (SD) or median and interquartile range (IQR) were calculated for continuous variables as appropriate, and frequency counts and percentages for categorical variables. All analyses were conducted in Stata v16 (StataCorp 2019). Missing data were not imputed; therefore, the base of patients for analysis could vary from variable to variable and was reported separately for each analysis.
Results
The analysis populations included in this study are shown in Figure 1. Of the 93 neurologists included, 68.8% (n = 64) were specialists in memory disorders/dementia (Supplemental Table 1). Physicians worked in nine different provinces or municipalities (Figure 2); all were from tertiary grade-A hospitals and 53.8% (n = 50) were working at a memory clinic. A total of 774 patients were included, with 584 patients having available MMSE at time of first consultation, 733 patients at time of diagnosis and 699 patients at time of survey (Figure 1).

Geographic spread of participating neurologists. Location data were available for 90 neurologists.
Patient demographic and clinical characteristics
At the time of survey, patients had a mean age of 69.3 (8.2) years, and 49.6% (n = 347) of patients were female (Table 1). Patients most commonly had completed middle school, except for those with MCI/mild dementia due to AD, who had most commonly completed high school. Most patients (71.8%, n = 501) lived with their partner or spouse. A considerable portion (41.7%, n = 287) of the patients were attending a memory clinic.
Patient demographic and clinical characteristics stratified by disease severity at time of survey.

AD: Alzheimer's disease; MCI: mild cognitive impairment; MMSE: Mini-Mental State Examination; SD: standard deviation.
Items reported by neurologists for >30% of patients are shown.
Items reported by neurologists for >10% of patients are shown.
Most patients had loss of short-term memory and difficulties in concentration/attention (80.7%, n = 564 and 51.5%, n = 360 respectively). The majority of patients with severe dementia due to AD at time of survey also had confusion with time or place, difficulties in recall of names/words and loss of long-term memory. The most recorded comorbid conditions across severity groups were arterial hypertension (23.3%, n = 163), anxiety (15.5%, n = 108) and hyperlipidemia (14.6%, n = 102). Median (IQR) MMSE score for the overall patient population was 21.0 (18.0–24.0) at the time of initial consultation, 21.0 (17.0–24.0) at the time of diagnosis, and 20.0 (15.0–23.0) at the time of survey (Figure 3).

Mean MMSE score, with median, interquartile range and min-max range, at initial consultation, diagnosis and time of survey stratified by disease severity at those timepoints. AD: Alzheimer's disease; MCI: mild cognitive impairment; MMSE: Mini-Mental State Examination.
Patient consultation history
Among patients with an MMSE score at initial consultation, other than with neurologists (74.3%, n = 434), patients most frequently first consulted with an internist or geriatrician (8.9%, n = 52 for both) or general practitioner (6.0%, n = 35), with loss of short-term memory being the most common symptom prompting initial consultation (72.5%, n = 420, Table 2). The patient's spouse or partner (48.7%, n = 284) was often the first to notice their cognitive decline and prompt the initial consultation. The median (IQR) time between first symptoms and first consultation was 17.6 (7.2, 39.0) weeks in the overall cohort.
Patient consultation history, stratified by disease severity at first consultation. Data are physician-reported unless noted otherwise.

AD: Alzheimer's disease; IQR: interquartile range; SD: standard deviation.
Items reported for/by >20% of patients are shown.
Includes grandson, granddaughter, sibling, other relative, friend or neighbor, professional caregiver, a healthcare professional during a consultation for a different health issue, the patient raised their concerns after being asked by a healthcare professional whether anything was worrying them during a consultation for a different health issue and other.
Of 148 patients across disease severities who self-reported data, 89.2% (n = 132) reported delaying their initial consultation, with the most commonly reported reasons included the belief that their memory problems were a normal part of ageing (58.3%, n = 77) and fear of what the diagnosis might be (48.5%, n = 64). Worries about losing independence (29.5%, n = 39) and other people's opinions (26.5%, n = 35) were also commonly reported reasons.
Diagnostic trajectory
Of those with an MMSE score at the point of diagnosis, only 19.5% (n = 140) of patients were diagnosed with AD at first consultation, and for those who were not, median time to diagnosis was 4.4 (1.7, 12.9) weeks (Table 3). Nearly all patients (99.9%, n = 723) underwent behavioral/cognitive assessments. as part of their diagnosis, followed by non-AD specific blood tests (87.8%, n = 636), feedback from patient/family (85.6%, n = 620), patient's family history (73.6%, n = 533), electroencephalography/ magnetoencephalography (59.8%, n = 433) and magnetic resonance imaging (MRI) (59.7%, n = 432) (Figure 4(a)). Few patients received fluorodeoxyglucose positron emission tomography (FDG-PET) scans to aid diagnosis (8.7%, n = 63).

Diagnostic tests and biomarkers used during diagnosis, stratified by disease severity at time of diagnosis. a) Types of tests used during diagnostic process. b) Type of biomarker testing used as part of diagnostic process. AD: Alzheimer's disease; CSF: cerebrospinal fluid; CT: computed tomography; EEG: electroencephalogram; FDG: fluorodeoxyglucose; MEG: magnetoencephalogram; MCI: mild cognitive impairment; MRI: magnetic resonance imaging; PET: positron emission tomography.
Patient diagnostic trajectory stratified by disease severity at initial diagnosis. Data are physician-reported unless noted otherwise.

AD: Alzheimer's disease; IQR: interquartile range; MEG: magnetoencephalogram; MCI: mild cognitive impairment; SD: standard deviation.
Excluding patients who were diagnosed at first consultation.
Genetic testing was conducted in 12.1% (n = 88) of all patients, with apolipoprotein E being the most tested gene (11.3%, n = 82) (Table 3). Genetic testing was offered but declined in a further 47.0% (n = 341) of patients. Notably, in those diagnosed with severe dementia due to AD, genetic testing was performed in only 2.7% (n = 2) of patients, and not offered to 64.9% (n = 48) of patients.
At initial diagnosis, diagnosis was confirmed with biomarkers in 19.1% (n = 138) of the overall patient cohort, though this ranged from 16.7% (n = 77) of those with a diagnosis of MCI/mild dementia due to AD to 31.2% (n = 24) of patients diagnosed with severe dementia due to AD. Of patients with biomarker-confirmed diagnosis, CSF testing alone (51.9%, n = 40) was predominantly used in the diagnosis of MCI/mild dementia due to AD, whereas PET imaging alone was most commonly used in AD with moderate or severe dementia diagnoses (40.5%, n = 15 and 83.3%, n = 20, respectively, Figure 4(b)).
Detailed data for all blood, CSF, and imaging biomarker testing were available for a limited subsample of patients and are reported in Supplemental Table 2. Briefly, the most common biomarkers used were total-tau and p-tau in both blood and CSF. Among patients with available data, abnormal amyloid signal based on amyloid PET scans was detected mostly in temporal and frontal regions and mostly bilateral. Reduced glucose metabolism based on FDG-PET scans was mostly located in the temporal regions.
As part of the attitudinal survey, physicians were also asked to report the proportion of patients for whom they perform biomarker testing as part of their diagnostic testing procedures. Of the 93 physicians surveyed, CSF testing was performed in a mean (SD) of 19.3% (20.5%) of their patients who present with symptoms of MCI/AD, and blood-based biomarker testing in a mean (SD) of 9.9% (18.8%) of patients (Supplemental Table 3). Amyloid or tau PET scanning was performed in 12.9% (17.1%) and 8.0% (13.5%) of patients who present with symptoms of MCI/AD, respectively. The most commonly reported challenges to implementing CSF biomarker testing were patient reluctance (68.8%, n = 64) and the low likelihood of routine availability (49.5%, n = 46), while commonly cited challenges to routine use of PET testing were cost to the patient (74.2%, n = 69) or healthcare system (38.7%, n = 36) and availability issues (35.5%, n = 33). Cost to patient (36.6%, n = 34) or healthcare system (20.4%, n = 19) and lack of accuracy (25.8%, n = 24) were the most commonly cited challenges in use of blood biomarkers.
Disease management
Of patients with an MMSE score at the time of survey, median number of neurologist visits in the 12 months prior to time of survey were 4.0 (3.0, 6.0, n = 699), and, in those prescribed treatment at time of survey (n = 627), patients were receiving a median (IQR) of 2.0 (1.0, 3.0) treatments (Table 4).
Healthcare resource utilization and treatment at time of survey, stratified by MMSE at time of survey.
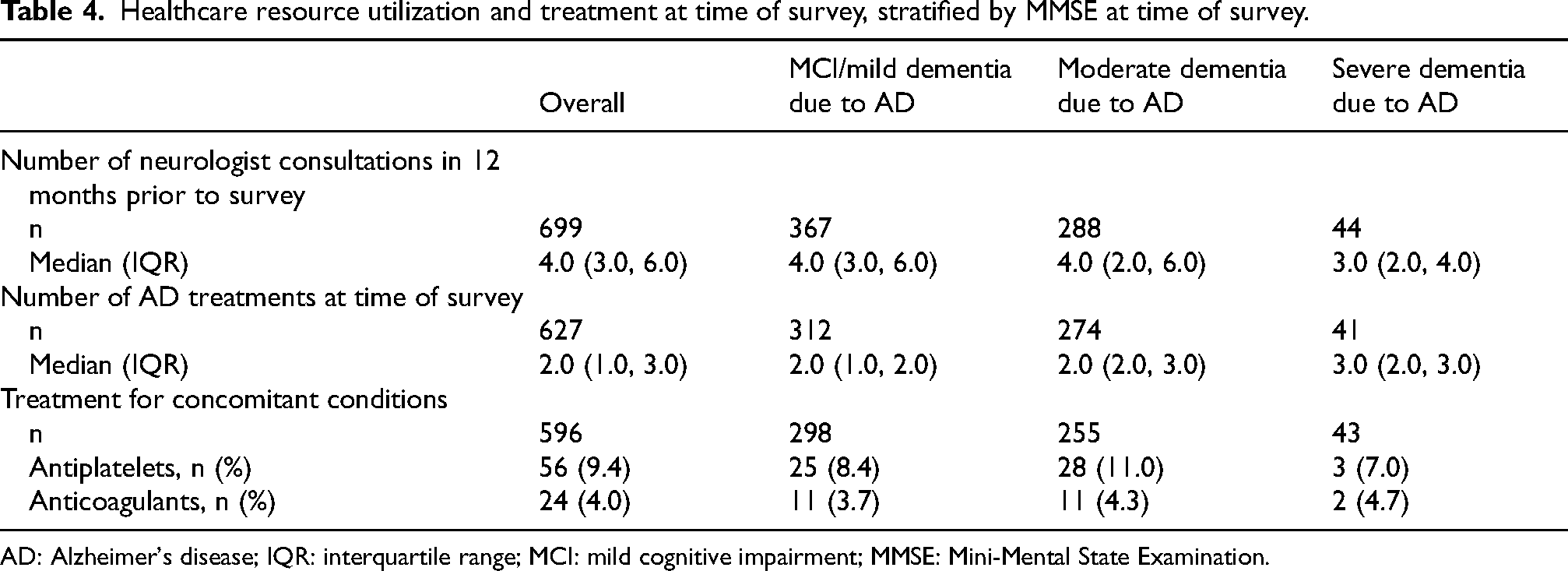
AD: Alzheimer's disease; IQR: interquartile range; MCI: mild cognitive impairment; MMSE: Mini-Mental State Examination.
Most patients (69.4%, n = 485) received acetylcholinesterase inhibitors, with use seen across severity categories. Other frequent treatment classes were N-methyl-D-aspartate (NMDA) antagonists (36.2%, n = 253) and nootropics (27.8%, n = 194). Use of NDMA antagonists and benzodiazepines were notably high in patients with severe dementia due to AD, at 61.4% (n = 27) and 52.3% (n = 23), respectively. Of note, 10.3% (n = 72) patients remained untreated at time of survey (Figure 5).

Treatments received at time of survey, stratified by disease severity at time of survey. AD: Alzheimer's disease; MCI: mild cognitive impairment; MMSE: Mini-Mental State Examination.
When asked to articulate their understanding of the term “disease modifying” in the context of treatment (Supplemental Table 4), physicians most commonly indicated that a disease-modifying treatment slows disease/symptom progression (81.7%, n = 76), improves patient quality of life (58.1%, n = 54), treats underlying cause of disease (55.9%, n = 52) or stops or reverses disease/symptom progression (57.0%, n = 53 and 53.8%, n = 50, respectively). The attributes most desired from a disease-modifying treatment by physicians were slowing or stopping disease/symptom progression (67.7%, n = 63 and 46.2%, n = 43, respectively), proven safety in long-term use (41.9%, n = 39) and long-term efficacy (40.9%, n = 38). Most physicians mostly or fully agreed with the statements that the amyloid and tau hypotheses are key to successful treatments (71.0%, n = 66 and 76.3%, n = 71, respectively).
Care partner characteristics and quality of life
The majority of patients, regardless of disease severity at the time of survey, received only non-professional care (Table 5). However, the proportion of patients receiving professional care in addition to informal care ranged from 0.8% (n = 3) in those with MCI/mild dementia due to AD to 31.8% (n = 14) in those with severe dementia due to AD, at the time of survey. Professional care was most commonly non-medical home help (56.5%, n = 35 of overall cohort).
Care received stratified by disease severity at time of survey.

AD: Alzheimer's disease; MCI: mild cognitive impairment; SD: standard deviation.
Non-professional care partners were most commonly the patient's partner/spouse (74.0%, n = 447) according to physician's reports, who spent 47.0 (45.8) hours per week for caregiving. Among non-professional care partners who completed a survey, mean age was 54.4 (10.0) years old and 53.7% (n = 261) were female (Supplemental Table 5).
Care partners’ mean EQ-VAS scores ranged from 80.6 (9.8) for those caring for patients with MCI/mild dementia due to AD to 75.9 (12.0) in those caring for patients with severe dementia due to AD. The majority of care partners reported health conditions of their own. Conditions most frequently reported have been brought on or worsened by caregiving included high blood pressure in those caring for patients with MCI/mild dementia due to AD (22.5%, n = 54) and sleeping problems in those caring for patients with moderate or severe dementia due to AD (23.0%, n = 50 and 31.0%, n = 9, respectively). Other conditions frequently reported to have been brought on, or worsened, by caregiving included stress, anxiety, depression, sleeping problems, and back pain (Supplemental Table 5).
Discussion
This nation-wide analysis provides a comprehensive assessment of the entire patient journey in MCI and AD in China, from the initial clinical presentation and consultation through diagnosis to treatment, and care partner impact. While previous studies in China have examined isolated aspects of AD management such as prevalence, 2 diagnostic capabilities, 19 or care partner burden, 11 our study uniquely integrates perspectives from physicians, patients, and care partners across the complete care continuum. With broad geographic regions covered and large sample sizes, the current study provided insights from the clinical practice landscape in China.
The mean age in our cohort was 69.3 years. This compared to a mean age of 76.5 in a large recent study in Europe and the US using similar methodology, 24 suggesting the Chinese patient population may be younger than those in Western countries. Most patients in this cohort (63.8%, n = 468) were diagnosed with MCI/mild dementia due to AD, which compares to 56% of patients in Europe and the US, scored using the same MMSE cutoffs. 24 A recent national survey in China with data collected during 2022–2023 reported that, among patients with cognitive impairment, about 41% had MCI or mild dementia (clinical dementia rating of 0.5 or 1) at consultation. 13 Differences in the scales used (Clinical Dementia Rating scale and MMSE), as well as in the sampling methods, prevent a direct comparison against the 65.2% (n = 381) having MCI/mild dementia due to AD at consultation in the current study. However, recent national initiatives in advancing early identification of AD, the evolving treatment landscape, and the current study's recruitment of a specialized sample of physicians may have contributed to difference.
Overall, most patients in our cohort consulted within the first year of noticing symptoms, with a median time of 17.6 weeks (4 months) to first consultation. This compares favorably to a mean time to first consultation of 6.1 months in Australia 25 and up to 35.4 months in France, 26 and contrasts with reports from a patient survey in China showing 39% of patients sought help in the second year after noticing symptoms. 12 However, these relatively short times to consultation may reflect recall bias and likely represent the time from recognition of more troublesome symptoms rather than earliest subtle changes.
Median time from first consultation to diagnosis in our cohort was approximately a month, substantially shorter than the 21.6 weeks reported in Europe and US, 24 while times of over a year have previously been reported in China. 27 Our population may have been biased by the fact that participating physicians were all neurologists based in tertiary hospitals, which may be more proactive in diagnosis than the general physician population.
Despite this quick diagnostic pathway, over one-third of patients presented with moderate to severe disease at initial diagnosis, suggesting significant delays in recognition of early symptoms, clinical consultation seeking and ultimately resulting in delayed diagnosis. Patients commonly reported delaying their first consultation due to believing their symptoms were part of normal aging, were afraid of the outcome of the consultation and were concerned about stigmatization. These barriers appear consistent with earlier reports in both China and Western countries. Misattributing forgetfulness as a normal part of aging and fear of stigmatization has consistently acknowledged by patients in China 28 and the US. 29 In a global survey, 70.2% of the general public considered dementia as part of normal aging. 30 In Europe and the US, physicians reported that lack of awareness/stigma and lack of understanding of what is part of normal aging were key barriers to diagnosis in 59.9% and 43.0% of cases. 24 Additionally, genetic testing was offered to most patients in our cohort but declined by almost half, potentially reflecting stigma concerns. These findings suggest that educational interventions addressing misconceptions and reducing stigma could substantially improve early diagnosis rates in China.
Early diagnosis, particularly when biomarker-confirmed, enables timely intervention with disease-modifying therapies to maximize clinical benefits. 31 CSF and blood amyloid-β and p-tau tests are recommended in Chinese guidelines to aid in AD screening and diagnosis.32,33 Genetic testing, including apolipoprotein E, is also recommended for risk stratification or identification of early-onset familial AD. 32 In our cohort, 19.1% of patients had a biomarker-confirmed diagnosis, while in a large study in the US and Europe, 15.2% of patients underwent any form of biomarker testing for diagnosis. 24 In our cohort, 11.2% received CSF testing, 8.0% received amyloid PET, and 4.7% received AD-specific blood tests. In Western countries, CSF testing proportion ranged from 2.7 to 27.3% of patients,24,34,35 amyloid PET from 5.1 to 22.3%24,34 and 6.6% of patients received AD-specific blood tests. 24 Although biomarker utilization in China appears to be broadly similar to that in Western countries, our findings should be interpreted with caution given that the current study was restricted to tertiary grade-A hospitals.
Our findings reveal a significant gap between physician attitudes and clinical practice. While most neurologists indicated they were either already using or likely to use biomarker testing, yet only a minority of patients received such testing, suggesting important practical challenges around biomarker testing. Patient reluctance, cost and limited testing availability have been identified among barriers to routine biomarker testing in our study, as well as in previous studies. 13 A recent survey of 2721 hospitals found that only 41.2% had the capacity to measure Aβ/tau in biofluids (CSF and plasma). Among hospitals with dementia-specific clinics or a dementia-specific inpatient department (n = 245), 13.7% could perform Aβ PET and 75.1% could perform CSF biomarker tests. 13 Despite these possible capacity limitations, a recent study estimated projected expansion in PET capacity in China would be sufficient for widespread biomarker testing under most scenarios. 36 Wider uptake of CSF-based screening is likely hindered by its lack of availability in outpatient clinics 2 and its invasive nature, with physicians commonly indicating patient reluctance as a barrier.
Patients in our cohort received mostly informal care, with 80.0% receiving exclusively informal care and 8.9% receiving any form of formal care. This contrasts with data from Europe and the US, where the proportion of patients not receiving formal care ranges from as low as 40% to up to 90%, depending on factors such as education and living circumstances. 37 This may suggest a greater reliance on informal care in China. Existing data have also shown that patients who live alone are at particular risk of not receiving any care. 37 Cultural differences are reflected in such living arrangements, with only 2.9% of Chinese patients living alone compared to 28.6–42.2% in Western cohorts. 37
Our findings revealed cultural differences in caregiving patterns, with spouses being the primary informal care partners in our cohort at 74.0%, while a previous study in China reported this to be 51.9%, 38 and in Western studies this proportion ranged from 15.7% to 21.8%, with the most common care partner being son/daughter (52.2% to 68.7%),39,40 once again suggesting possible cultural differences regarding major caregiving population between China and Western countries. The definition of caregiving time varied across studies.41,42 In our study, the time spent on caring was assessed without distinguishing between active care and supervision. Mean number of hours spent caring per week in our cohort of informal care partners ranged from 27.2 for sons to 47.0 for spouses. Estimates for Europe and North America range from 24.5 to 30.8 h per week,41,42 suggesting care burden in China is comparable, if not greater, than that in Western countries. This is further substantiated by older studies, showing AD care partners in China may spend up to 20 h per day giving care,43,44 a burden that impacts caregiver health, particularly for those supporting patients with severe dementia due to AD, underscoring the need for improved diagnostic, therapeutic and holistic management approaches despite current disease management efforts.
Our study has several strengths, including employing a large geographically diverse sample of physicians, patients and care partners, and requiring a consecutive series of patients to reduce selection bias. However, we must acknowledge several limitations. Our results may be biased by the relatively higher hospital level and physician selection criteria. While neurologists act as the principal specialists in the diagnosis and management of AD in China, geriatricians and psychiatrists may also be involved, especially for the management of comorbidities and behavioral and psychological symptoms of dementia. 12 The exclusive inclusion of neurologists in this study may have prevented the generalizability of our findings to multidisciplinary clinical settings. Participating patients may not reflect the general Alzheimer's disease population, since the DSP only includes patients who are consulting with their physician. This means that patients who consult more frequently have a higher likelihood of being included. Patient eligibility was based on physician judgement rather than a standardized diagnostic checklist; however, this approach reflects the physician's real-world classification of their patients. Recall bias, inherent in survey methodologies, may have affected responses of both physicians and patients. However, physicians did have the ability to refer to the patients’ records while returning data, thus minimizing the possibility of recall bias.
Conclusion
Our study provides a comprehensive overview of the diagnostic journey, biomarker testing, treatment and care partner burden in patients with mild cognitive impairment and AD dementia in China. Real-world gaps and hurdles in early AD diagnosis and biomarker-based screening exist, including stigmatization and lack of patient awareness, inadequate testing availability, patient reluctance and cost, and significant burden for care partners remains. Our data highlight the need for continued efforts to improve readiness of the healthcare system for the optimal management of AD.
Supplemental Material
sj-docx-1-alr-10.1177_25424823261447853 - Supplemental material for Diagnostic journey, biomarker testing, treatment, and care partner burden in patients with mild cognitive impairment and Alzheimer's disease dementia in China: A real-world survey
Supplemental material, sj-docx-1-alr-10.1177_25424823261447853 for Diagnostic journey, biomarker testing, treatment, and care partner burden in patients with mild cognitive impairment and Alzheimer's disease dementia in China: A real-world survey by Jiawei Xin, Hanxi Zhang, Shuang Cai, Jinnan Li, Guanshen Dou, Brenda Botello Estrada, Chloe Walker, Rebecca Storm and Xiaochun Chen in Journal of Alzheimer's Disease Reports
Footnotes
Acknowledgements
The authors thank Niels Haan (Adelphi Real World), Poh Sien Ooi and Molly Yu, PhD (Parexel Int.) for assistance with manuscript writing.
Ethical considerations
Data collection was undertaken in line with European Pharmaceutical Marketing Research Association guidelines 23 and the Declaration of Helsinki of 1964 and subsequent revisions. This study was granted exemption from ethical approval by the Pearl Institutional Review Board (#22-ADRW-172, #22-ADRW-173).
Consent to participate
Patients and care partners provided informed consent to take part in the study.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The analysis used data from Adelphi Real World Dementia Disease Specific Programme, a survey conducted independently by Adelphi Real World. The DSP is a wholly owned Adelphi Real World product. Eli Lilly is one of multiple subscribers to the DSP. Publication of survey results was not contingent on the subscriber's approval or censorship of the publication.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CW and RS are employees of Adelphi Real World. HZ, SC, JL, GD and BBE are employees and minor shareholders of Eli Lilly & Company. All other authors declared no conflict of interest.
Data availability statement
All data, i.e., methodology, materials, data and data analysis, that support the findings of this survey are the intellectual property of Adelphi Real World. All requests for access should be addressed directly to Chloe Walker at chloe.walker@omc.com. Chloe Walker is an employee of Adelphi Real World.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.