
Abstract
Background
Despite the growing evidence on the modifiable and genetic factors associated with cognitive health, little is known about the role of the apolipoprotein E (APOE) gene ε4 allele in the associations between productive or leisure activities and cognitive health.
Objective
This study fills a gap of knowledge by examining the associations among employment, civic engagement, and leisure activities and cognitive health by the presence of APOE ε4 allele, an established risk factor of Alzheimer's disease (AD).
Methods
Using pooled data from the Health and Retirement Study (HRS) Psychosocial and Lifestyle Questionnaires (2010–2016) and the HRS data on APOE ε4 alleles, linear regression models with a lagged dependent variable were performed to examine associations between productive or leisure activities and cognitive functioning at the follow-up time point, as well as the role of APOE ε4 in these associations.
Results
Among all participants, employment, low or high-intensity volunteering, and cognitive/social leisure activities were associated with higher levels of cognitive functioning. The presence of at least one ε4 allele was related to poorer cognitive functioning at the follow-up time point. Among people without the APOE ε4 allele, employment, high-intensity volunteering, and cognitive/social leisure activities were significantly associated with cognitive functioning. Among people with at least one APOE ε4 allele, low-intensity volunteering and cognitive/physical leisure activities were significantly associated with better cognitive functioning.
Conclusions
We found that employment, civic engagement, and leisure activities all contribute to cognitive health, although the benefits may be restricted to low-intensity volunteering and cognitive/physical leisure activities among individuals with at least one APOE ε4 allele, who are known to be inherently at a greater risk of AD, highlighting an avenue to a relatively easily implementable strategy to promote cognitive health in this subpopulation.
Introduction
Alzheimer's disease (AD) is one of the leading causes of death in the United States. 1 Age is the biggest risk factor for AD, and more Americans are living into old age. With an increasing number of individuals living longer, research is needed to identify modifiable health behaviors to delay the onset and severity of cognitive decline. 2 Productive activities, employment, and civic engagement are associated with healthy brain structure and cognitive health benefits.3–6 In addition, there is growing evidence regarding the cognitive health benefits of leisure activities.7–9 Yet, important gaps in knowledge still remain, notably evidence regarding the role of genetic predisposition, such as the presence of the apolipoprotein E (APOE) gene ε4 allele, an established risk factor for AD, 10 in the association between productive activities and cognitive functioning.
Theory and empirical evidence
The environmental complexity hypothesis suggests that healthy brain development can occur due to exposure to complex environments, including occupational environments.11–13 Importantly, this theoretical framework suggests that cognitive health and functioning can be maintained across the lifespan through continuous complex interactions with the environment. Although advanced older age is associated with cognitive decline, this perspective argues that the absence of complex activities, not age alone, is a risk factor for cognitive decline. Productive activities, such as paid work and civic engagement that contribute to the greater society, can offer cognitively challenging and stimulating environments.3,5 Among the many health benefits of volunteering,14,15 longitudinal and experimental studies reveal that civic activities are associated with executive function, memory, enhanced speed of processing, and neurocognitive plasticity.16–19 In addition, some leisure activities are also associated with cognitive health benefits. For instance, among older adults in Colombia, leisure activities were found to be associated with a decreased risk of cognitive impairment without dementia and a lower risk of dementia altogether, independent of educational attainment and literacy, when examined cross-sectionally. 20 Similar findings are evident among older Chinese and Swedish adults.21,22 Shin and colleagues (2021) found that the number of hours spent reading books and using a computer was positively associated with crystallized intelligence score, which is one of the proxies for cognitive functioning that is focused on learned knowledge and language. In addition to reading books, their study revealed that engaging in hobbies, attending movies and the theater, attending study circles, and visiting and/or being visited by friends and/or relatives were associated with better cognition. Another study focusing on Chinese older adults found that frequent engagement in social activities (e.g., playing cards and visiting cinemas) and physical activities (e.g., walking and active sports) were associated with lower odds of cognitive decline. 23 Interventions that focus on leisure activity are important domains for interventions because they can be performed until the end of life. 7 Thus, engaging in various activities, both productive and non-productive, may help maintain and protect brain health in later life. To summarize, productive activities are paid or unpaid activities performed by older adults that can bring social benefits distinguishable from leisure activities. The present study explores how productive and leisure activities are associated with cognitive health while considering important covariates.
There are important genetic factors that affect the onset of AD, other age-related cognitive impairments, and cardiovascular conditions.2,24,25 One of the well-known genes that are associated with increased risk for AD is the allele 4 variant of the apolipoprotein E gene (APOE ε4). Compared to those with one or no APOE ε4 alleles; those with two APOE ε4 are at higher risk of developing AD.25–27 The reason why APOE ε4 increases the risk of AD is still unclear, but research indicates that it may be associated with the function of apolipoprotein E (ApoE) in helping carry cholesterol and fat in the bloodstream. 28 ApoE operates as a lipid transport protein. 29 When lipids are not regulated properly, they could be associated with neurodegenerative diseases. 29 One recent study found that APOE ε4 had a negative effect on the association between lifestyle activities and cognitive reserve in women only, concluding that sex and APOE ε4 carrier status are important factors to consider in these associations. 30 Despite the importance of incorporating APOE ε4 into cognitive health research, existing studies in productive and leisure scholarly discourses have not examined the effect of APOE ε4.
The present study
The present study examined the associations between productive or leisure activities and cognitive functioning among older adults in the United States (U.S.) with four waves (2010, 2012, 2014, and 2016) from the Health and Retirement Study (HRS). This study was guided by the following research question: Are there associations between activities and the maintenance of cognition? Are the associations between activities and maintenance of cognition different for those without APOE ε4 than for those with APOE ε4? We hypothesized that productive and leisure activities would be associated with higher cognitive functioning on follow-up for older adults both with or without the APOE ε4 allele overall, but that there will be a difference by APOE ε4 status. This would mean that those with APOE ε4, who are at a higher risk of AD, could benefit from the modifiable factors of productive and leisure activities. To the best of the authors’ knowledge, this is the first study to examine how both productive and leisure activities are associated with cognitive functioning among diverse older adults in the U.S. while considering the presence of APOE ε4.
Methods
Sample
Data come from the HRS: the longitudinal HRS core data, the Research and Development (RAND) HRS data, the Psychosocial Lifestyle Questionnaires (also called Leave-Behind Questionnaires [LBQ], which contain leisure activity information), and the HRS APOE and Serotonin Transporter Alleles. The HRS is a longitudinal, nationally-representative, population-based study of older adults aged 51 + years, sponsored by the National Institute on Aging (NIA U01AG009740) and conducted by the University of Michigan.31–33 Beginning in 1992, participants have responded to the HRS core survey every two years. The sample is replenished every six years. Most variables come from the RAND HRS data files from the RAND Center for the Study of Aging. The RAND HRS variables are harmonized across waves and are imputed if they would otherwise have a high number of missing cases (e.g., cognition) in the raw data set. 31 The LBQ is collected in each biennial wave from a rotating 50% of the core panel respondents. 33 For instance, data from the randomly selected half of Group A were collected in 2006, 2010, and 2014, whereas the data from the remaining half of Group B were collected in 2008, 2012, and 2016. Sociodemographic characteristics, health characteristics, and cognitive health variables were selected from the RAND HRS. Some measurements changed over time. Thus, to select consistent measures, the present study used the data from 2010 to 2016 (4 waves: waves 2–4 are follow-ups).
Following the recommended representative ages based on the birth cohorts from HRS, the sample was restricted to participants aged 51+ . The HRS employs a steady-state design, where the sample is replenished every six years with a younger cohort. Thus, the minimum age among cohort-eligible participants in follow-up waves may vary, requiring the limiting of the ages of the respondents for each wave. 34 Pooled together, after matching the HRS LBQ respondents with the APOE data respondents, there were 12,542 participants with cognitive functioning measures at Time 1 (T1, pooled 2010 and 2012) and 10,291 participants at Time 2 (T2, pooled 2014 and 2016). If the responses were provided by a proxy in either wave, they were excluded (resulting in 12,542 participants with cognitive functioning measures in T1 and 10,281 in T2). We excluded those with cognitive functioning below a normal range, indicating a ‘demented’ state at T1 (e.g., cognitive functioning score six or less), resulting in 12,117 participants with cognitive measures in T1 and 10,120 in T2. There were 8,744 participants who did not miss the cognitive measure in both T1 and T2. We included a final analytic sample of 7,605 participants who had the study variables. Sensitivity analyses indicated that participants included in the listwise deletion models were younger, better educated, and had slightly more female representation compared to the participants excluded from the listwise deletion process. The multiple imputation results were similar in the direction and significance of the major predictors (i.e., work, volunteering, and leisure activity variables). However, in the multiple imputation models, having two and one APOE ε4 alleles compared to no APOE ε4 allele was associated with lower cognitive functioning at T2 across models.
Measures
Cognitive functioning (dependent variable at T2)
Total cognitive functioning scores ranged from 0 to 27, with higher scores representing better cognitive functioning.35,36 The measure assesses three major areas of cognitive functioning: episodic memory (i.e., immediate word recall test, scored: 0–10, and delayed word recall test, scored: 0–10), 37 working memory (serial sevens test, scored: 0–5), and attention/processing speed (backward counting, scored: 0–2). Cognitive functioning as a continuous variable was used.
Productive activities (employment and volunteering; independent variables at T1)
Employment status was categorized into the following four groups: employed full-time, employed part-time/partly retired, retired, and unemployed/disabled/not in the labor force. Formal volunteering was asked as the following: ‘These next questions ask about volunteer work and helping activities. Have you spent any time in the past 12 months doing volunteer work for religious, educational, health-related or other charitable organizations?’ Volunteering in the past 12 months was categorized into the following three groups: no volunteering, low-intensity volunteers (less than 100 h), moderate-intensity (100 h to 200 h), and high-intensity volunteers (more than 200 h).
Leisure activities (independent variables at T1)
Cognitive, social, and physical leisure activity variables and classifications were selected based on previous research.38–41 For cognitive, social, and physical leisure activities, the responses were categorized into the following three categories: no engagement (never/not in the last month), monthly engagement (once a month/several times a month), and weekly engagement (once a week/several times a week/daily). Categorization based on the count was informed by the study by Bone and colleagues. 39 Using continuous variables resulted in the same significant leisure activity variables.
Cognitive leisure activity used the following ten 7-point scale items (1 = daily, 2 = several times a week, 3 = once a week, 4 = several times a month, 5 = at least once a month, 6 = not in the last month, 7 = never/not relevant): (1) Attend an educational or training course; (2) Pray privately in places other than a church or synagogue; (3) Read books, magazines, or newspapers?; (4) Do word games such as crossword puzzles or Scrabble; (5) Play cards or games such as chess; (6) Write (such as letters, stories, or journal entries); (7) Use a computer for e-mail, Internet or other tasks; (8) Bake or cook something special; (9) Make clothes, knit, embroider, etc.; and (10) Work on a hobby or project.
Social leisure activity used the average of the following three 7-point scale items: (1) Do activities with grandchildren, nieces/nephews, or neighborhood children; (2) Go to a sport, social, or other club; (3) Attend meetings of non-religious organizations, such as political, community, or other interest groups.
Physical leisure activity used the following two 7-point scale items: (1) Play sports or exercise and (2) Walk for 20 min or more.
Covariates (T1)
Sociodemographic characteristics include age (years), gender (1 = male, 0 = female), education (1 = high school or lower, 2 = some college, 3 = college degree and above), race/ethnicity (1 = non-Hispanic White, 2 = non-Hispanic Black, 3 = Hispanic), marital status (1 = married/partnered, 2 = separated/divorced, 3 = widowed, 4 = never married), and log-transformed income. The following health-related factors were included, given evidence of their association with cognitive performance: T1 cognitive functioning, CESD depressive symptoms (0–8, this is a continuous variable where a higher score indicates a higher level of depressive symptoms), self-rated health (The original variable ranged from 1 = excellent, 2 = very good, 3 = good, 4 = fair, and to 5 = poor; this measure was reverse-coded for interpretation: 1 = poor to 5 = excellent), diabetes (1 = yes, have the condition; 0 = no, do not have the condition), 2 and smoking status (1 = never, 2 = previous smoker, and 3 = current smoker).
Statistical analysis
Descriptive statistics with weights were conducted to describe the sample characteristics. Next, lagged dependent variable regression models were performed controlling for cognitive functioning at T1 to answer the proposed research questions. In Table 2, all participants (n = 7605) were included to examine the following set of models: Model 1a focused on employment and key predictors of cognitive health; Model 1b focused on formal volunteering and key predictors; Model 1c-1 focused on cognitive leisure activities and key predictors; Model 1c-2 focused on social leisure activities and key predictors; and Model 1c-3 focused on physical leisure activities and key predictors. In Table 3, the same models were examined among participants without the APOE ε4 allele (n = 5630). In Table 4, the same models were examined among participants with at least one APOE ε4 allele (n = 1975). Analyses were conducted in Stata MP version 17. 42 The complex survey design and weighting were applied following previous studies.43,44
The associations between leisure activities and cognitive functioning among older adults (n = 7605).
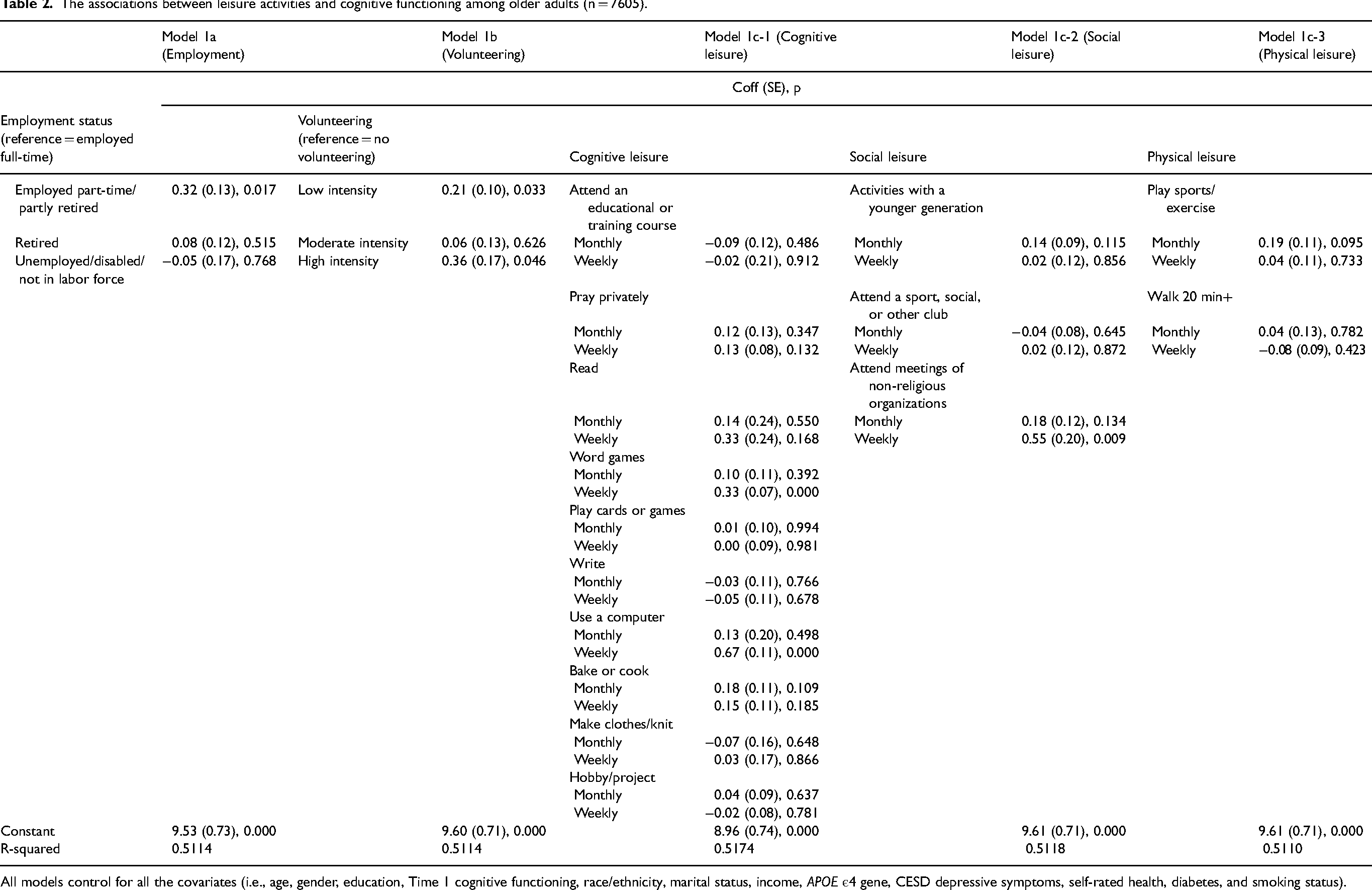
All models control for all the covariates (i.e., age, gender, education, Time 1 cognitive functioning, race/ethnicity, marital status, income, APOE ε4 gene, CESD depressive symptoms, self-rated health, diabetes, and smoking status).
The associations between leisure activities and cognitive functioning among participants without the APOE ε4 allele (n = 5630).
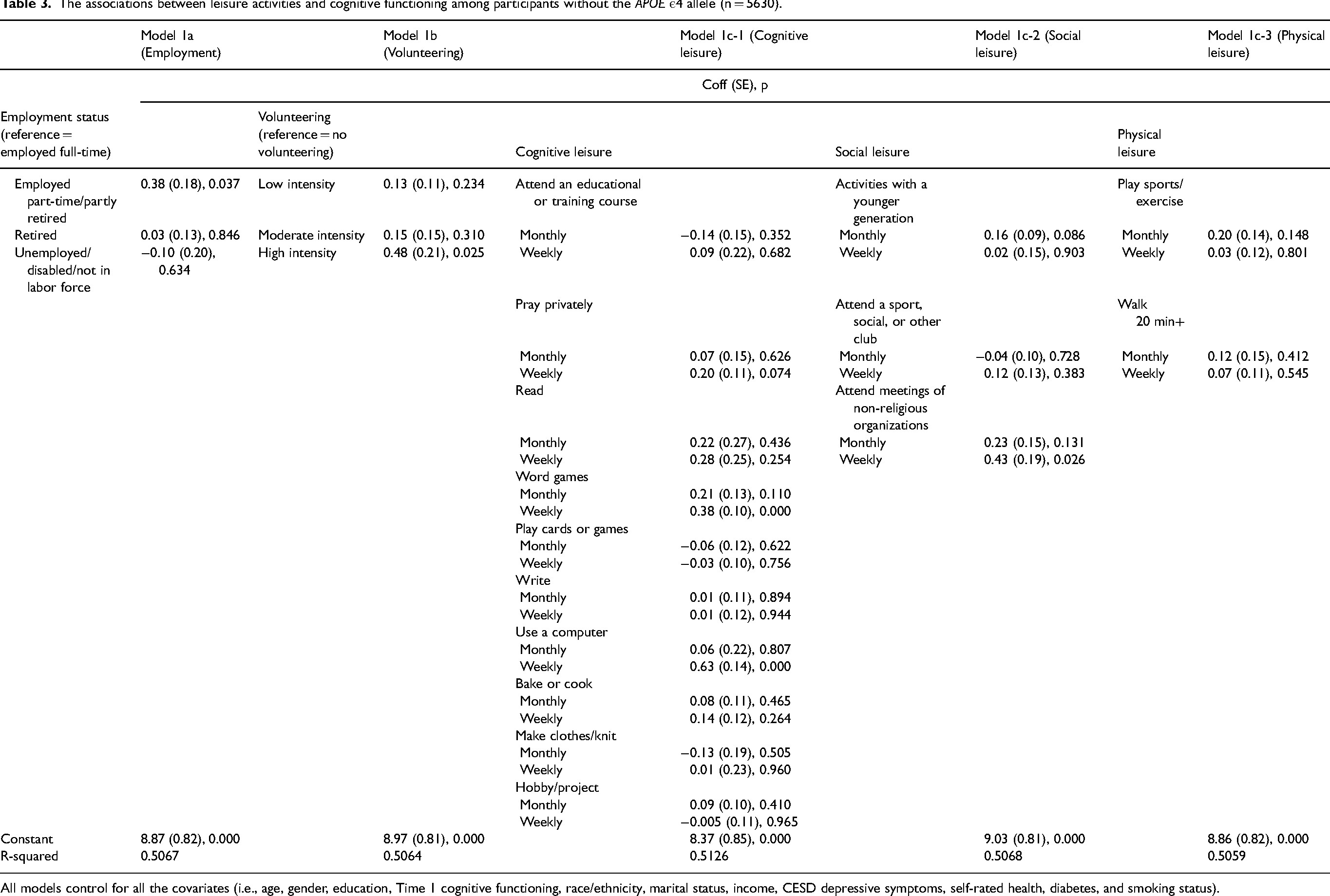
All models control for all the covariates (i.e., age, gender, education, Time 1 cognitive functioning, race/ethnicity, marital status, income, CESD depressive symptoms, self-rated health, diabetes, and smoking status).
The associations between leisure activities and cognitive functioning among participants with at least one APOE ε4 allele (n = 1975).
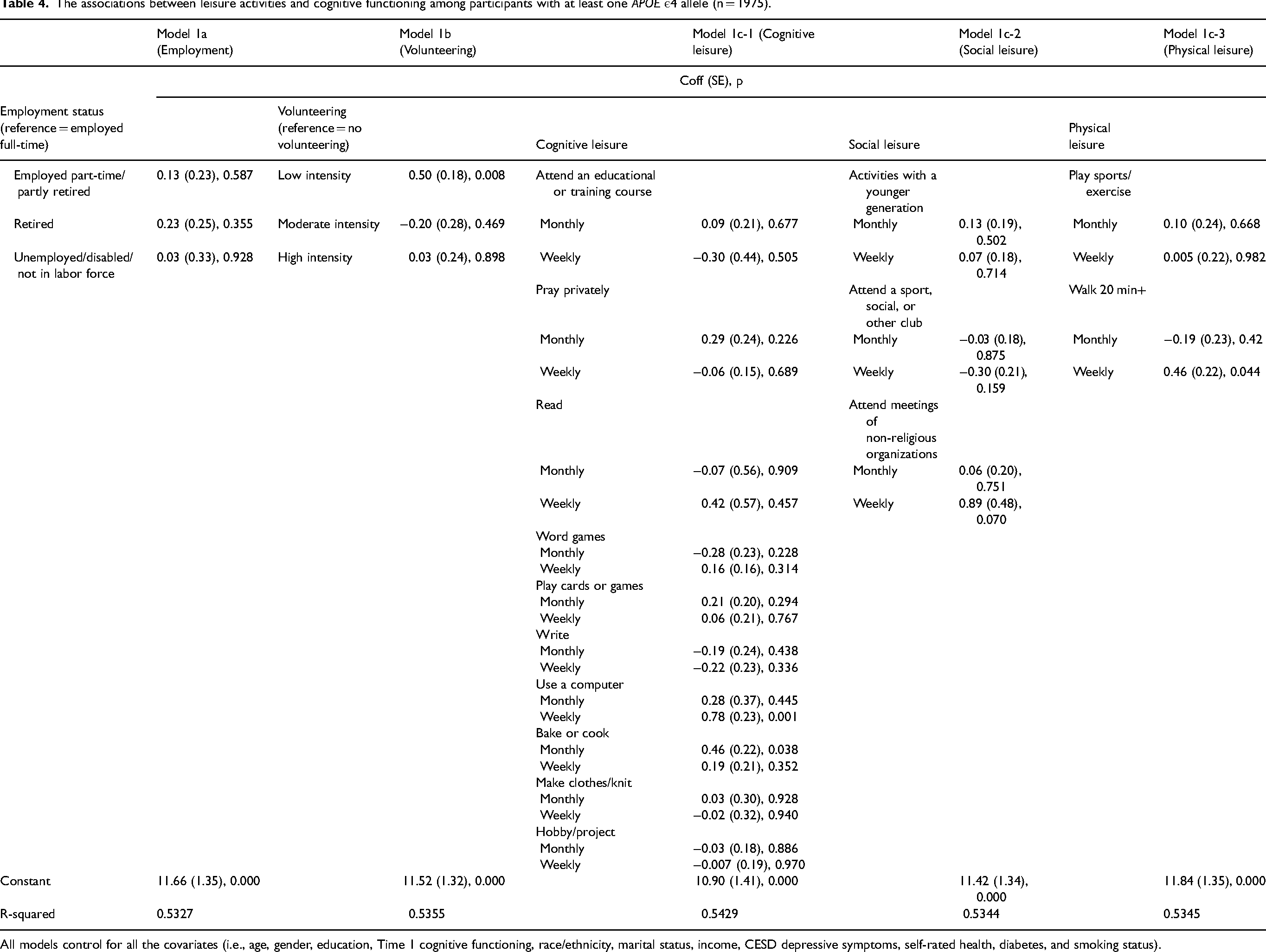
All models control for all the covariates (i.e., age, gender, education, Time 1 cognitive functioning, race/ethnicity, marital status, income, CESD depressive symptoms, self-rated health, diabetes, and smoking status).
Results
The sample characteristics are presented in Table 1. Focusing on the weighted distribution, the mean age of respondents was 64 years (SE = 0.26). More than half of the respondents were female (54%), with almost 43% having a high school or lower education level. The majority of the participants were non-Hispanic White (85%), and 70% were married. The mean log-transformed income was 10.87 (SE = 0.03). In terms of health, the mean score of cognitive functioning at T1 was 16 (SE = 0.07, range: 7–27). Over 74% of participants had no ε4 allele, and 26% had one or two ε4 alleles. On average, respondents had a score of 1.15 (SE = 0.03) for depressive symptoms (10.76% of having depressive symptoms), which indicates a lower frequency of depressive symptoms. They had a mean self-reported health of 3.40 (SE = 0.02), indicating good self-rated health. About 19% had diabetes, and 12% were current smokers. Among the productive activities, 34% worked full-time, and 55% did not volunteer. The frequency of leisure engagement varied across cognitive, social, and physical leisure activities. Cognitive functioning at T2 had a mean score of 16.03 (SE = 0.08).
Descriptive statistics.
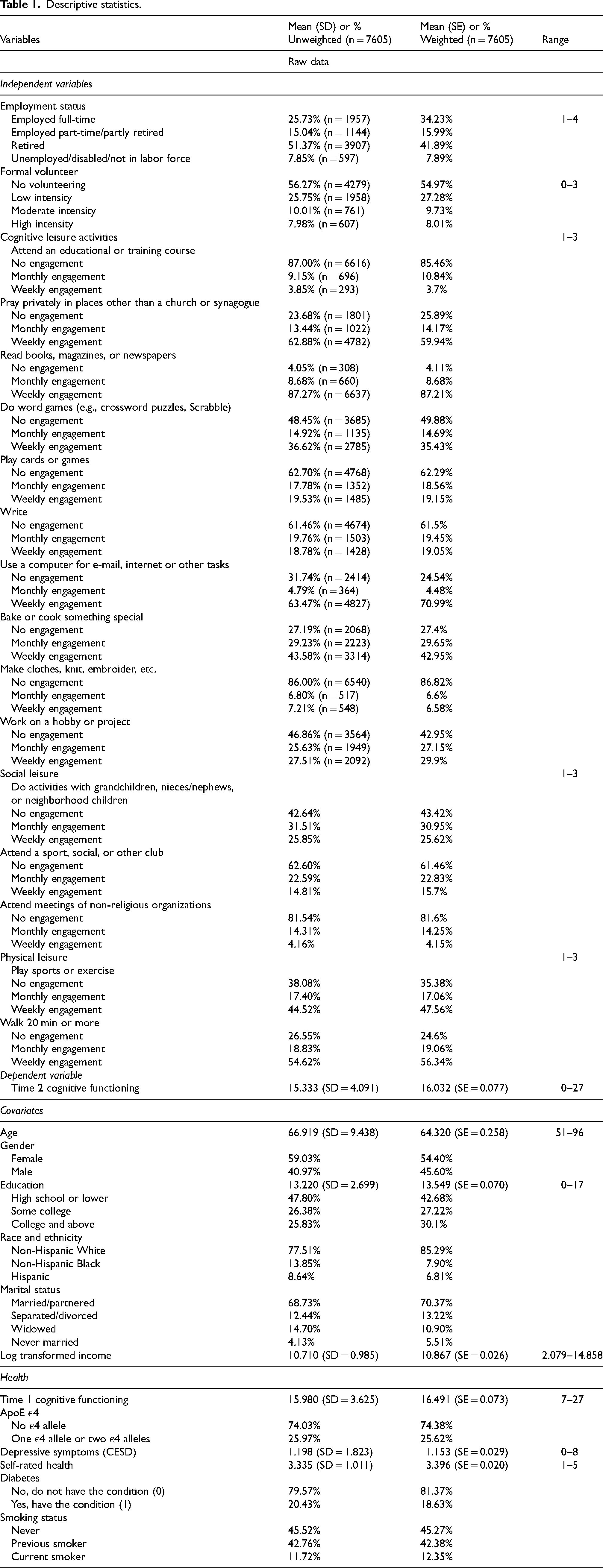
Table 2 represents associations between productive or leisure activities and cognitive functioning at T2 among all participants (n = 7605): employed part-time/partly retired, volunteered at low or high intensity, and some leisure activities were associated with cognitive functioning. Model 1a indicated that among all participants, being employed part-time/partly retired was associated with better cognitive functioning (B = 0.32, p = 0.017). In Model 1b, compared to those who did not volunteer, people who were engaged in low-intensity volunteering (B = 0.21, p = 0.033), and those who were engaged in high-intensity volunteering (B = 0.36, p = 0.046) had better cognitive functioning at T2. When cognitive leisure activities were examined in Model 1c-1, weekly engagement word games (B = 0.33, p < 0.001) and weekly engagement in using a computer (B = 0.67, p < 0.001) were associated with better cognitive functioning at T2. Model 1c-2 indicated that weekly engagement in attending meetings of non-religious organizations was marginally associated with higher levels of cognitive functioning at T2 (B = 0.55, p = 0.009). Physical leisure activities in Model 1c-3 presented a marginally significant association between monthly exercise and cognitive functioning at T2 (B = 0.19, p = 0.095). Across all models, the presence of the APOE ε4 alleles was statistically associated with lower cognitive functioning. Variables in all models explained approximately 51% to 52% of the variance in cognitive functioning at T2.
Table 3 represents associations between productive or leisure activities and cognitive functioning at T2 among participants without the APOE ε4 allele (n = 5630). Employment, volunteering, cognitive leisure activities, and social leisure activities were significantly associated with cognitive functioning. Model 1a indicated that part-time employment and partial retirement status were associated with higher cognitive functioning at T2 (B = 0.38, p = 0.037). In Model 1b, compared to those who did not volunteer, people who were engaged in high-intensity volunteering had better cognitive functioning at T2 (B = 0.48, p = 0.025). When cognitive leisure activities were examined in Model 1c-1, weekly engagement in word games (B = 0.38, p < 0.001) and using a computer (B = 0.63, p < 0.001) were associated with better cognitive functioning at T2. Model 1c-2 indicated that weekly engagement in attending meetings of non-religious organizations was associated with higher levels of cognitive functioning at T2 (B = 0.43, p = 0.026). In all models, the independent variables explained approximately 51% of the variance in the outcome.
Table 4 represents associations between productive or leisure activities and cognitive functioning at T2 among participants with at least one APOE ε4 allele (n = 1975). Among people with at least one APOE ε4 allele, volunteering and some leisure activities were associated with cognitive functioning. In Model 1b, compared to those who did not volunteer, people who were engaged in low-intensity volunteering had better cognitive functioning at T2 (B = 0.50, p = 0.008). When cognitive leisure activities were examined in Model 1c-1, weekly engagement in using a computer (B = 0.78, p < 0.001) and monthly baking/cooking (B = 0.46, p = 0.038) were associated with better cognitive functioning at T2. Model 1c-2 indicated that weekly engagement in attending meetings of non-religious organizations was marginally associated with higher levels of cognitive functioning at T2 (B = 0.89, p = 0.070). Model 1c-3 examined the association between physical leisure activities and cognitive functioning at T2. Walking weekly was associated with higher levels of cognitive functioning (B = 0.46, p = 0.044). Independent variables in all models explained approximately 53% to 54% of the variance in cognitive functioning at T2.
Overall, among the covariates, it was found that being older, Black, Hispanic, a current smoker, and having low education, lower baseline cognitive functioning, low income, worse self-rated health, diabetes, and depressive symptoms were associated with lower cognitive functioning at T2.
Discussion
The present study examined productive and leisure activities in relation to cognitive functioning in later life among older adults in the U.S. while considering the role of APOE ε4, a major risk factor for AD. The main findings indicate that among participants without at least one APOE ε4 allele, employment (i.e., working part-time or being partly retired), volunteering (i.e., high-intensity), weekly engagement in word games, weekly computer usage, and attending meetings of non-religious organizations were associated with higher levels of cognitive functioning at follow-up, compared to their counterparts. Among participants with at least one APOE ε4 allele, low-intensity volunteering, weekly engagement in using a computer, monthly baking/cooking, and walking weekly were associated with higher levels of cognitive functioning at T2. These results provide insights into activities that can be recommended for those with APOE ε4 who are inherently at a higher risk of developing AD and often in search of modifiable activities that could be implemented into their daily lives. When the full sample was analyzed, employment (i.e., being employed part-time/partly retired), low-intensity volunteering, high-intensity volunteering, weekly engagement in word games, and weekly engagement in using a computer were associated with better cognitive functioning at T2.
These results are mostly consistent with studies focused on the environmental complexity hypothesis and productive aging research indicating that cognitively stimulating and socially engaging activities are beneficial to the human brain and cognitive health.3,11–13,17,23 Also, the finding of having APOE ε4 alleles to be a risk factor for cognitive health is supported by the previous literature. 25 Productive and some leisure activities were associated with better cognitive functioning while controlling for the APOE ε4 alleles. Modifiable cognitive health interventions to promote these activities may reduce the development of cognitive decline and impairment. More studies are needed to try to replicate these findings, as well as to assess which groups might benefit the most (e.g., populations with a genetic predisposition to cognitive impairment, racial and ethnic minorities, lower-educated, worse health, socially isolated, etc.) from particular activities.
Findings from this study are similar to other studies that show maintained or improved cognitive functioning among older adults who engaged in productive activities,2,5,7,14,20,45 especially varying levels of intensity in intergenerational volunteer programs, such as AARP's Experience Corps. 17 The findings about cognitively stimulating leisure activities (i.e., a significant association between word game/using a computer and cognitive functioning) were consistent with a research study that found a significant positive association between the number of hours spent using a computer or playing cards/games/solving puzzles and total cognition score. 22 The cognitive health benefits of exercise were supported in previous literature. 46
Research has generally found a dose-response relationship between civic engagement and health outcomes: More volunteer hours are positively associated with various health outcomes. For instance, volunteering at least 100 h per year was found to be significantly associated with increased positive self-perceptions of aging and fewer depressive symptoms; 47 volunteering at least 200 h per year was associated with lower odds of developing hypertension and better psychological well-being and physical activity compared to not volunteering; 48 greater hours of volunteering were associated with higher levels of well-being. 49 One study revealed a nonlinear association between volunteering hours and health, showing decreased perceived physical health benefits of volunteering after 100 h per year. 50 A study by Proulx et al. 36 found that all levels of formal and informal volunteering were associated with higher levels of cognitive functioning when compared to not volunteering. They also found that the cognitive benefits of volunteering 100–199 h per year reduced over time. None of these studies examined how APOE ε4 allele status plays a role, but some evidence indicates possible nonlinear volunteering health benefits. Clearly, more research is needed to clarify linear and curvilinear associations between civic activities and health.
Limitations
Although the study utilized the domains of labor force status and leisure activities, people who may be engaged in other types of activities may not have been captured, such as homemakers and caregivers who may be exposed to highly stimulating environments depending on the demands of those roles. Second, all of the health measures are self-reported, thus they may be subject to reporting and social desirability biases. Moreover, some of these activities merely measured the roles and not the mechanisms. Furthermore, while the study captured time spent volunteering, it did not capture the complexity of volunteering—a measure that needs to be developed. Similarly, this study did not examine the underlying mechanisms of how leisure activities (e.g., word games, computer usage, social engagement) are associated with cognitive health. Further research is needed to understand the mechanisms to examine how these civic and leisure activities can be protective factors for cognitive health in later life. Finally, alternative statistical methods, such as propensity score weighting and latent class analyses, can help clarify causality across diverse groups that might share similar genetic and health behaviors.
Implications and conclusion
Despite these limitations, there are important implications for research, practice, and social policy. The present study findings are consistent with the previous literature indicating the benefits of cognitive, social, and physical activities in relation to dementia. 51 To advance scientific knowledge, future research could identify barriers to productive and leisure activity engagement among older adults. It is important to understand how these activities are associated with cognitive health across racially and ethnically diverse older adults and design interventions for populations at greater risk for developing cognitive impairment. Studies examining the mechanisms of activity engagement and cognitive health benefits can help develop cognitive health programs for older adults. Future research can also explore different cognitive health domains as outcomes.
In this study, we found employment, volunteering, and some leisure activities have cognitive health benefits regardless of the APOE ε4 allele's presence. It is important to note that among people with at least one APOE ε4 allele, volunteering and some leisure activities were important factors that were associated with cognitive functioning. Providing opportunities to engage in moderate volunteering consistently would be critical in promoting the cognitive health of people at higher risk of dementia and other related conditions. Expanding opportunities for formal education, reduction in the prevalence of poverty, support for mental health, and prevention of diabetes and smoking could be examples of potential cognitive health promotion programs. Volunteering opportunities could also provide chances for older adults to learn more about health education.
Offering cognitive and social leisure activity programs for older adults may provide cognitively stimulating environments in later life. Gerontologists, social workers, and health care providers working with older adults should make plans with their clients and patients to understand the impact of active lifestyles on cognitive performance and to develop diverse activity portfolios with consideration of the environment and needed resources.
Our findings have implications for social policy at the federal level in the U.S. Senior Corps (Retired and Senior Volunteer Program, Foster Grandparent Program, and Senior Companion), Older Americans Act, and senior centers have become resources for older adults to access opportunities for civic engagement, employment, social activities, and better health. 52 Senior centers serve approximately 1 million older adults and policies should encourage collaborations with community organizations to increase cognitive and social leisure activities and other productive activity engagement.
In conclusion, the present study provides empirical evidence that not just productive activities, but also cognitively and socially stimulating leisure activities, can be important to maintaining cognitive functioning, while considering the role of APOE ε4. Productive and leisure activity programs can be cost-effective modifiable interventions to prevent or delay cognitive impairment in later life, especially for those who are at a higher risk of AD.
Footnotes
Acknowledgments
The researchers are grateful to the study participants, data providers, and Kuakini COBRE for making this study possible. The authors have no further acknowledgments to report.
Author contributions
Yeonjung Jane Lee (Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Writing – original draft; Writing – review & editing); Ernest Gonzales (Conceptualization; Supervision; Writing – original draft; Writing – review & editing); Yanyan Wu (Methodology; Supervision; Writing – review & editing); Kathryn L Braun (Supervision; Writing – review & editing); Peter Martin (Methodology; Supervision; Writing – review & editing); Bradley Willcox (Funding acquisition; Supervision; Writing – review & editing); Ross Andel (Conceptualization; Methodology; Supervision; Writing – original draft; Writing – review & editing).
Funding
Kuakini Medical Center, NIH grant 1P20GM125526-01A1 (Kuakini Honolulu Heart Program Center of Biomedical Research Excellence for Clinical and Translational Research on Aging).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.