
Abstract
Post-stroke movement disorders are a spectrum of rare complications associated with subcortical strokes. While these disorders tend to spontaneously resolve, early symptomatic management can complement ongoing stroke rehabilitation. There is no standardized management rationale for these disorders, which include chorea, athetosis, and hemiballismus, but treatment revolves around neurotransmitter modulation. We discuss a 91-year-old Caucasian male with a history of hypertension and type 2 diabetes mellitus who suffered a thalamic stroke with left-sided vascular choreoathetosis. The choreoathetosis markedly improved over 2 weeks with sodium valproate and risperidone, which were continued throughout rehabilitation and in the outpatient setting. The patient was readmitted a month later with a recrudescence of slurred speech and decreased mobility due to a suspected respiratory tract infection but reported no re-exacerbation of choreoathetosis. Risperidone was ceased during the second admission, and the patient was discharged on sodium valproate, with subtle evidence of residual left upper-limb chorea.
Introduction
Post-stroke movement disorders (PSMDs) are a spectrum of rare complications that can alter disease progression and treatment. 1 The frequency of PSMDs is unclear, with estimates of 1%-4%.2, 3 Chorea, athetosis, and hemiballismus are hyperkinetic movement disorders that are a part of the same spectrum of disease. Chorea refers to rapid, involuntary motions of flexion, extension, rotation, or crossing, which tend to involve distal extremities. Hemiballismus is a severe form of chorea characterized by violent, large-amplitude involuntary movements. Athetosis refers to slow, writhing movements mainly affecting distal extremities. 4 Disruption of the cortical, subcortical, or cerebellar circuitry contributes to PSMDs. 1 Although these conditions spontaneously resolve, short-term management may comprise antidopaminergic therapy, including typical and atypical neuroleptics and catecholamine-depleting agents.4, 5 Herein, we present an elderly male with choreoathetosis who responded to sodium valproate and risperidone.
Case Report
A 91-year-old Caucasian male presented to the emergency department (ED) in the afternoon with a sudden onset of progressively worsening left-sided involuntary jerking movements that were first noticed overnight. The purposeless movements were constant in his left upper limb, with intermittent involvement of the left lower limb. Associated symptoms included mild confusion and slurring of speech that were reported to have somewhat improved by the time of presentation. The patient had been otherwise well, with no precipitating headaches, visual disturbances, palpitations, or head trauma. He had never experienced this cluster of symptoms before and is normally right-handed.
The patient had several cardiovascular risk factors, including hypertension, atrial fibrillation, heart failure with reduced ejection fraction, ischemic heart disease, type 2 diabetes mellitus, and chronic kidney disease, for which he was on regular medications. His only regular neuropsychiatric medication was mirtazapine. There were no changes to his medications or missed doses leading up to his presentation. He recalled no family history of a similar presentation and had no significant social history. On initial ED assessment, he was found to have sensation intact bilaterally, brisk reflexes, and power 5/5 in both the upper and lower limbs. His random blood sugar level around admission was 9.0 mmol/L. Initial ED considerations were a basal ganglia infarct or partial seizure.
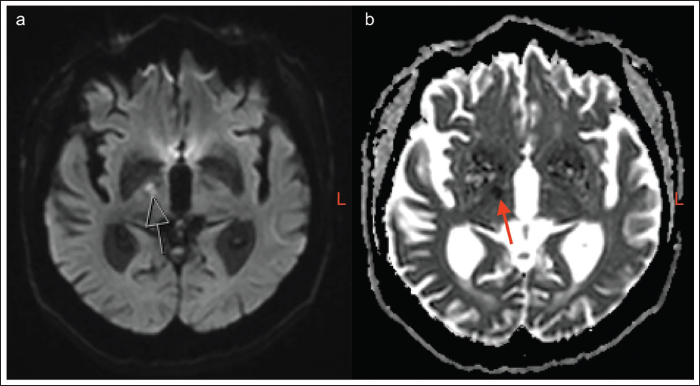
An initial non-contrast brain computed tomography (CT) scan reported no acute intracranial pathology. Given his ongoing involuntary jerks, an electroencephalogram (EEG) was considered, but a magnetic resonance imaging (MRI) scan of the head was prioritized by the treating team. The MRI identified an acute ischemic right thalamic infarct with mild age-related diffuse brain atrophy (Figure 1). A Doppler ultrasound of the carotids demonstrated mixed atherosclerotic disease bilaterally, with the degree of carotid stenosis later confirmed on CT angiogram to be approximately 80% on the left and 50% on the right.
Diffusion-weighted Magnetic Resonance Imaging (DW-MRI) Sequences of Right Thalamic Infarct with Age-related Diffuse Brain Atrophy. (a) B1000 Sequence. (b) Apparent Diffusion Coefficient (ADC) Sequence.
Routine blood tests were consistent with previous admissions, with normal levels of non-HDL cholesterol measured at 3.2 mmol/L, but glycated hemoglobin (HbA1c) was elevated at 7.1%. A transthoracic echocardiogram identified an ejection fraction of 20%. His systolic blood pressure (SBP) was previously reported to fluctuate between 115 and 135 mmHg at home.
With consideration of his medical history and imaging results, the patient was diagnosed with vascular choreoathetosis secondary to an ischemic right thalamic lacunar infarct. He was initially responsive to sodium valproate 500 mg bidaily (BD) to manage the choreoathetosis. After 5 days, it was decided that the patient would benefit from adding 0.5 mg risperidone BD, which was then titrated to 1 mg BD after a week. Risperidone was preferred over quetiapine, as guidelines suggested it is only helpful for chorea at high doses, for example, 300 mg daily. 6 No significant side effects were observed with dual treatment, and the patient’s symptoms markedly improved over the 2 weeks.
Vascular consultation suggested medical management of the carotid stenosis with lifelong aspirin 100 mg daily and atorvastatin 80 mg daily, as the patient was deemed unfit for surgical intervention given his age and comorbidities. With the support of ongoing rehabilitation, the patient’s functionality improved over the approximate 2-month hospital stay, and he was advised to continue sodium valproate (500 mg BD) and risperidone (1 mg BD) on discharge.
The patient was readmitted around a month later with a 2-day history of coryzal symptoms, worsening slurred speech, and decreased mobility. CT and MRI brain scans excluded an acute infarct, and his neurological symptoms were thought to be a stroke recrudescence precipitated by a respiratory tract infection. The patient reported no re-exacerbation of choreoathetosis but had some subtle residual left upper limb chorea. Risperidone was ceased at discharge, and the patient was to be continued on sodium valproate (500 mg BD) as an outpatient.
Discussion
Strokes affecting subcortical structures are more prone to develop PSMDs than cortical strokes. 5 Thalamic strokes are frequently attributed to lacunar infarction, in which small penetrating cerebral vessels are occluded due to pathologies such as lipohyalinosis and microatheromas. 7 Embolic events can also contribute to subcortical infarcts if a deep penetrating artery is occluded.5, 7 Anisetti et al. 8 suggest that high SBP variability increases stroke risk, and factors increasing variability include older age, hypertension, and chronic kidney disease, all of which comprise the medical history of our patient. A case series of patients with acute/subacute onset hemiballismus or chorea found that 11 out of 13 patients with diabetes mellitus had elevated HbA1c levels, suggesting a metabolic component to the development of movement disorders. 9
PSMDs comprise both hyperkinetic and hypokinetic disorders. 1 Clinical presentations may be difficult to classify due to overlapping features of abnormal movements and variation in severity. 4 Generally, hyperkinetic disorders are characterized by excessive, abnormal involuntary movements, as observed in our patient with features of chorea and athetosis. Hypokinetic disorders, including vascular parkinsonism, manifest as slowness of movement.1, 4 Transient dyskinesias may be difficult to differentiate from seizures, although EEGs during attacks do not show epileptiform activity. 4 Continuous jerking movements could also suggest epilepsia partialis continua, a rare form of recurrent focal seizures that can occur post-stroke, but these are classically clonic or myoclonic jerks restricted to one body part. 10
Understanding the pathophysiology of movement regulation can aid pharmacotherapy. The subcortical circuitry acts as a regulatory feedback mechanism, in which neocortical signals are relayed through the striatum, pallidum, and thalamus back to the cortex. 4 Cortical activity triggers the striatum to release the thalamus from pallidum inhibition, thereby allowing thalamic outputs to excite the cortex. These direct pathways are modulated by excitatory indirect pathways from both the substantia nigra (dopaminergic) and subthalamic nuclei (glutamate). Interruption of direct or indirect pathways may lead to PSMDs. Hence, PSMD management involves neurotransmitter regulation. However, there are no standardized guidelines for the pharmacological management of PSMDs. 5 In our case, sodium valproate and risperidone were utilized.
Sodium valproate has proven effective in managing Sydenham’s chorea in pediatric populations. 11 It is also an established treatment modality for epilepsy. While its exact mechanism of action is unknown, it is suggested that valproic acid inhibits the gamma-aminobutyric acid (GABA) transaminase enzyme, which is responsible for degrading GABA, the predominant inhibitory neurotransmitter in the brain. Valproic acid also inhibits voltage-gated sodium channels to decrease neuronal transmission and stimulates GABA synthesis by increasing the activity of glutamic acid decarboxylase, the enzyme responsible for converting glutamate into GABA. 12 Additionally, sodium valproate may reduce the risk of recurrent stroke through non-specific inhibition of the histone deacetylase 9 gene, which normally promotes atherosclerosis. 13
Antipsychotics can also be used for neurotransmitter regulation. Typical antipsychotics such as haloperidol block dopamine D1 and D2 receptors and are a first-line agent for hemiballismus.4, 5 However, typical antipsychotics have a greater risk of drug-induced parkinsonism and tardive dyskinesia than atypical antipsychotics. 5 Atypical antipsychotics such as risperidone and olanzapine antagonize dopamine D2 receptors with a lower affinity than first-generation antipsychotics. They also have a high antagonistic affinity for serotonin 5-HT2A receptors, which further reduces the risk of extrapyramidal side effects. 14 A study comparing risperidone, olanzapine, and tetrabenazine, a vesicular monoamine transporter 2 inhibitor, for the management of Huntington’s chorea identified comparable efficacy among the three drugs, with risperidone considered superior. 15 Koro et al. 16 established early on that patients taking olanzapine have a significantly increased risk of developing diabetes, while those taking risperidone have a non-significant risk. Regardless, a dose-dependent increase in diabetes risk is suggested for both olanzapine and risperidone. 17 For our patient with type 2 diabetes mellitus, risperidone was selected by the treating team.
Ultimately, there is limited research directly comparing the efficacy of these drugs for PSMDs. Moreover, it is unclear to what extent the recovery of our patient was spontaneous and how much of it was facilitated by sodium valproate and risperidone. 4 An EEG was also not obtained in the acute setting to identify any underlying seizure activity that may have guided the treatment regimen. Finally, the effectiveness of sodium valproate monotherapy after the second discharge was not determined.
Conclusion
PSMDs are rare complications associated with subcortical infarcts that require symptomatic control to facilitate rehabilitation. We present an elderly thalamic stroke patient with choreoathetosis who was effectively managed in hospital with sodium valproate and risperidone. Given the scarcity of reported PSMDs, ongoing research is required to optimize the acute pharmacotherapy regimen.
Footnotes
Author Contributions
All authors contributed to the article: conceptualization (AA), data curation (DA), writing—original draft (DA), writing—review & editing (DA, SM, and AA).
Data Sharing Statement
The data analyzed are not publicly available due to privacy and ethical reasons.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This report was exempted from ethical approval and reviewed by our district’s research committee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this case report.