
Abstract
Background
Females are disproportionately affected by strokes when compared to males. This may be attributed to non-traditional stroke symptoms in females and stroke care sex variance. This study explored sex and ethnicity discrepancies in the FAST-ED and stroke outcomes.
Methods
An internal hospital registry created in 2017 evaluated EMS FAST-ED compliance and monitored patient outcomes. We assessed two cohorts, the 2017 cohort collected one year after FAST-ED implementation, and the 2019 cohort collected two years after FAST-ED implementation. Inclusion criteria included patients aged ≥18 years arriving via EMS as a stroke alert; walk-ins were excluded. EMS FAST-ED compliance, FAST-ED score, final diagnoses, door to needle time (DTN), door to puncture (DTP) time, and stroke treatment volumes were evaluated for sex differences.
Results
1,156 cases were analyzed, 638 (55%) were female. EMS FAST-ED compliance decreased by 17%, but did not differ by sex or ethnicity. EMS FAST-ED score was similar for females and males. Despite the similarity in FAST-ED score, females scored higher on the initial NIHSS (F(1) = 6.25, p < .05) and discharge NIHSS (F(1) = 8.588, p < .01). Those diagnosed with a stroke were 1.4 times more likely to be female (χ²wald = 6.21, p < .01, 95% CI [1.07–1.80]). Treatment rates did not vary between sex or ethnicity and overall DTN decreased by 10 minutes (2017 cohort M = 36 minutes, SE = 1.96; 2019 cohort M = 26 minutes, SE = 1.69).
Conclusions
The FAST-ED demonstrated equitable implementation and scoring among a diverse population, regardless of sex or ethnicity. Additionally, patients were equally likely to receive treatment, while benefiting from a decrease in DTN times.
Introduction
Ischemic strokes are a leading cause of death and long-term disability within the United States, 1 affecting more females than males. Stroke prevalence has been consistently higher for females between 2015 and 2018. 2 In addition, females disproportionately have worse stroke outcomes compared to males. 3 Some of these differences may be attributed to reduced pre-hospital stroke recognition, 4 a reduction in stroke priority, 5 and general delays in receiving stroke treatment. 6
A recent study identified that early National Institute of Health Stroke Scale (NIHSS) scores assessed at initial stroke presentation tended to be higher for males compared to females, 7 indicating that males appear to have more severe strokes than females. However, the authors noted that females were more likely to present with non-focal stroke symptoms, not currently captured by the NIHSS, which may have resulted in decreased stroke severity scores. 7 The NIHSS is an early measure of stroke severity and is frequently used by treating physicians to make stroke treatment decisions. The NIHSS is also the premise of most pre-hospital measures used by Emergency Medical Services (EMS) to triage stroke. If the NIHSS does not fully capture stroke severity for females this could cause rippling effects with stroke care beginning with pre-hospital stroke assessment.
One of the pre-hospital assessment measures currently used is called the Field Assessment Stroke Triage for Emergency Destination (FAST-ED). This tool helps to detect large vessel occlusion strokes and route them to the nearest thrombectomy-capable or comprehensive stroke center. This tool was successfully implemented in South Florida in 2017, improving door-to-reperfusion times. 8 If the patient is given a FAST-ED score of four or greater, they are transported to the nearest comprehensive stroke center, by-passing closer hospitals. For FAST-ED scores of six or greater, the neuro-interventional team for the receiving hospital is activated from the field. 8 Given the significant role this tool plays in timely stroke triage, it is important to identify whether any sex differences in either compliance or scoring exist. To the best of our knowledge, this tool has not been evaluated for sex disparities.
In the current study, we investigated sex discrepancies with the FAST-ED and NIHSS for patients who arrived via EMS to the Emergency Department of a community comprehensive stroke center in South Florida. Two cohorts were evaluated—one shortly after the FAST-ED initiative was implemented in 2017 and another two years after implementation in 2019.
Methods
We performed a retrospective cohort study using an existing FAST-ED stroke quality database from a South Florida community comprehensive stroke center. Waivers of informed consent and HIPAA authorization were granted by a local Institutional Review Board (BHSF1667091). We assessed two cohorts, the 2017 cohort was comprised of data collected the year after FAST-ED implementation (March 1, 2017 to February 28, 2018) and the 2019 cohort included data collected two years after FAST-ED implementation (March 1, 2019 to February 28, 2020). Only adult cases that arrived via EMS services were included in this analysis. Demographic information collected included age, sex, race, and ethnicity. Stroke data collected included EMS-reported FAST-ED, calculated FAST-ED, initial NIHSS, initial stroke symptoms, stroke treatment type (thrombolysis, endovascular therapy [EVT], or both), stroke treatment times (door to needle time [DTN], door to puncture time [DTP]), stroke diagnosis (acute ischemic stroke [AIS], hemorrhagic, transitory ischemic attack [TIA] or other), and discharge NIHSS. Other data available included length of stay (LOS) and discharge disposition. The FAST-ED score was abstracted from the EMS run sheet. The calculated FAST-ED scores were derived from the initial NIHSS using the worksheet provided by Lima and colleagues in 2016. 9 A Fast-ED difference score was calculated by subtracting the calculated FAST-ED from the EMS-reported FAST-ED. This was done to evaluate stroke progression from EMS assessment to hospital arrival. Positive scores indicated a decrease in stroke symptoms upon arrival; whereas, negative scores indicated an increase in stroke symptoms upon arrival.
Statistical Analysis
Descriptive analyses of baseline demographics were completed. FAST-ED compliance was evaluated using Pearson’s Chi-square analysis between the 2017 and 2019 cohorts. Additional Pearson’s Chi-square analysis was also used to evaluate the relationship between FAST-ED compliance and stroke severity and a logistic regression was used to explore if FAST-ED compliance influenced stroke diagnosis. A three-by-two-factor analysis with sex (e.g., male & female), ethnicity (e.g., Hispanic & non-Hispanic), cohort (e.g., 2017 & 2019), and their interactions were used to evaluate the primary endpoints of EMS-reported FAST-ED, Calculated FAST-ED, FAST-ED difference score, and initial NIHSS. The secondary endpoints of stroke treatment rates were evaluated using binary logistic regression on sex after controlling for ethnicity and cohort, whereas stroke treatment times were evaluated using factor analysis. Nominal regression was used to evaluate the role of sex, ethnicity, and cohort on stroke diagnosis and discharge disposition. All statistical tests were performed using SPSS version 25 at the alpha level of 0.5.
Results
Demographics
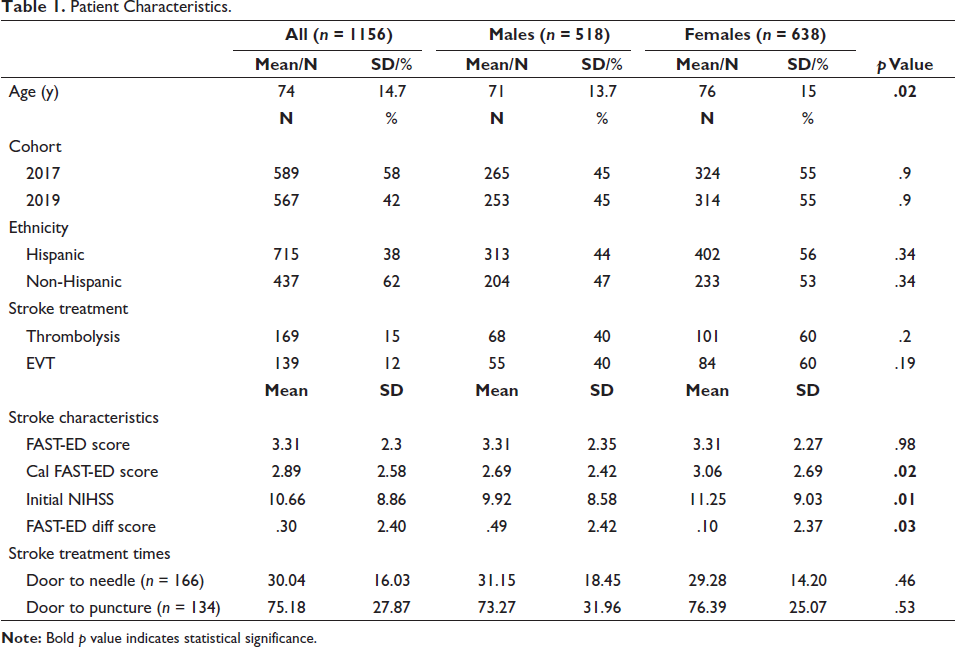
The database included 1,156 cases from 3/1/2017 to 2/28/2018 and 3/1/2019 to 2/28/2020. Of those, 808 cases had reported FAST-ED scores by EMS. The sample was evenly split between the two cohorts, with 589 cases in the 2017 cohort (51%) and 567 cases in the 2019 cohort (49%). The sex proportion between the two cohorts was similar with 324 (55%) females in 2017 cohort and 314 (55%) in the 2019 cohort. Likewise, there was a similar proportion of Hispanic patients between cohorts (2017 63%, n = 367; 2019 62%, n = 348). The average age was 73.6 (SD = 14.67, range 21–102), average length of stay was 7.6 days (SD = 14.6, range 0–298), and average presenting NIHSS was 10.6 (SD = 8.8, range 0–38). Most patients were diagnosed with AIS (47.9% n = 554), followed by intracerebral hemorrhage (ICH) (8% n = 93), TIA (7.5% n = 87), and subarachnoid hemorrhage (SAH) (1.4% n = 16). The remaining subjects did not receive a primary stroke diagnosis. Of those with AIS, 15% (n = 169) received thrombolytic therapy and 12% (n = 139) underwent EVT. A complete list of variables is available in Table 1.
Patient Characteristics.
FAST-ED Compliance
There was a significant decline in reported FAST-ED scores by EMS from 2017 to 2019 from 58.3% to 41.7% (χ 2 = 55.769, p < .001). The FAST-ED score was reported 17% less often on the EMS run sheet. Despite the decrease in reported FAST-ED scores on EMS run sheets, there was no statistically significant difference in FAST-ED compliance between sex or ethnicity. FAST-ED compliance was not associated with stroke severity (χ 2 = 2.29, p = .52), the non-compliant group’s average initial NIHSS score was 10.44 (SD = 9.07) and the compliant group’s score was 10.28 (8.77). Lastly, FAST-ED compliance did influence stroke diagnosis (χ²wald (3) = 12.7, R 2 = 0.02, p < .01). Non-compliant FAST-ED patients were 1.47 times more likely to be diagnosed as a stroke mimic than the compliant FAST-ED patients (χ²wald = 7.53, p < .01, 95% CI [1.12–1.94]). All other stroke diagnosis types remained similar between the two categories.
FAST-ED and Initial NIHSS Score
There were no statistically significant differences in reported EMS FAST-ED scores for sex, ethnicity, or cohort. When considering the calculated FAST-ED score, there was statistically significant primary sex (F(1) = 5.78, p < .05) and cohort effects (F(1) = 6.20, p < .05). Females (M = 3.06, SE = 0.11) had higher calculated FAST-ED scores compared to males (M = 2.69, SE = 0.12) and the 2019 cohort (M = 3.08, SE = 0.11) had higher calculated FAST-ED scores compared to the 2017 cohort (M = 2.67, SE = 0.11). Similar results were found with the initial NIHSS; females (M = 11.25, SE = 0.36) had statistically significantly higher NIHSS (F(1) = 6.25, p < .05) when compared to males (M = 9.92, SE = 0.40) (see Table 1). When evaluating the FAST-ED difference score, only cases that contained both an EMS FAST-ED score and a calculated FAST-ED score were evaluated. There were statistically significant primary effects of sex (F(1) = 4.87, p < .05) and cohort (F(1) = 3.90, p < .05). Males (M = 0.49, SE = 0.13) had higher positive scores compared to Females (M = 0.10, SE = 0.12) and the 2017 cohort (M = 0.47, SE = 0.11) had higher positive scores compared to the 2019 cohort (M = 0.11, SE = 0.14).
Stroke Diagnosis, Acute Stroke Reperfusion Treatments, and Outcomes
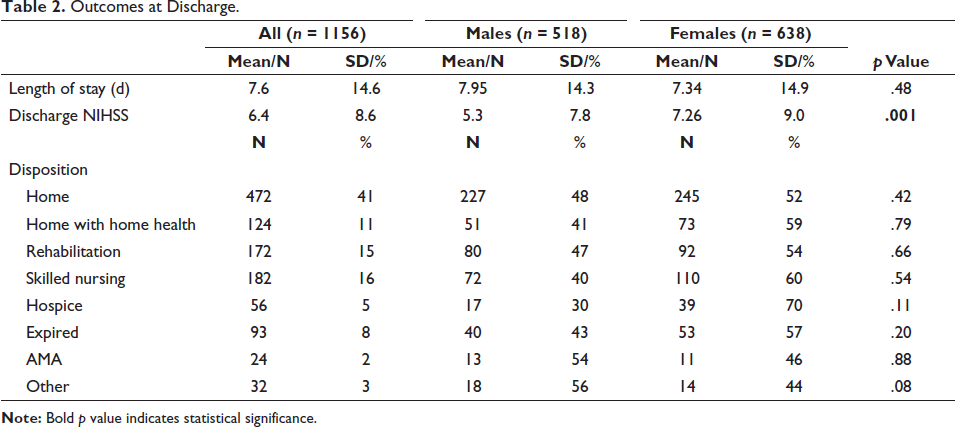
Patients who received a stroke diagnosis, as compared to non-stroke diagnoses, were 1.4 times more likely to be female than male (χ²wald = 6.21, p < .01, 95% CI [1.07–1.80]), as noted in Table 1. Treatment rates did not statistically vary between sex, ethnicity, or their interactions. However, logistic regression did show that those in the 2019 cohort were 1.7 times more likely to receive stroke treatment (χ²wald = 14.42, p < .001, 95% CI [1.29–2.27]), when compared to their 2017 cohort counterparts. Additionally, there was a statistically significant improvement (F(1) = 18.34, p < .001) in DTN between the 2017 cohort (M = 36 minutes, SE = 1.96) and the 2019 cohort (M = 26 minutes, SE = 1.69) as illustrated in Figure 1. DTP times did not vary by cohort. Importantly, stroke treatment times (i.e., DTN and DTP) did not vary by sex or ethnicity. When considering discharge NIHSS, females (M = 7.26, SE = 0.43) had statistically significantly higher discharge NIHSS (F(1) = 8.588, p < .01) when compared to males (M = 5.33, SE = 0.46) as noted in Table 2; whereas discharge NIHSS remained similar between ethnicities. Lastly, sex and ethnicity were not statistically significant when considering discharge disposition.
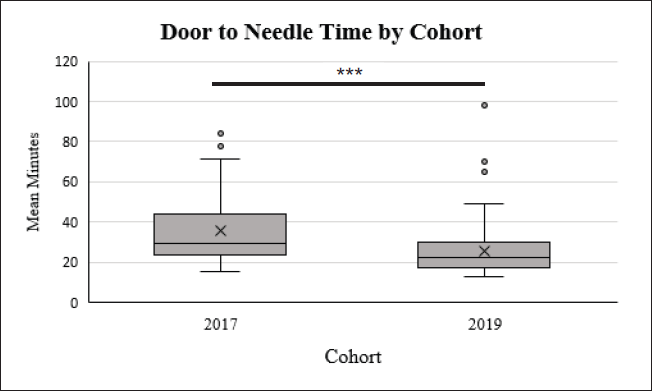
Boxplots Show the Door to Needle Treatment Times by Cohort where X Indicates the Sample Mean in Comparison to the Sample Median and the Dots Indicate Outlier Cases.
Outcomes at Discharge.
Discussion
Our study on the effect of biological sex on FAST-ED demonstrated no significant compliance concerns or numerical score disparities with sex or ethnicity. EMS personnel were equally likely to implement the FAST-ED initiative on all patients, regardless of biological sex or ethnicity. Despite these reassuring findings, overall FAST-ED compliance rates declined between the 2017 and 2019 cohorts. The decline in compliance does not appear to be related to stroke severity but does seem to be related to final stroke diagnosis. More patients without FAST-ED scores were diagnosed with a stroke mimic. EMS were able to correctly identify AIS and TIAs in 55.4% of patients. Another study had similar findings, wherein EMS were able to correctly identify 59.9% of AIS and TIA patients. 10 Overall, the decline in FAST-ED compliance and rate of false stroke alerts highlights the need for continual EMS training, to ensure all EMS personnel are familiar and comfortable using the FAST-ED assessment tool and understand its significance for improving treatment times and patient outcomes.
Even with the decline in compliance, our results showed an improvement in stroke treatment rates and DTN times between 2017 and 2019 with no discrepancy based on sex or ethnicity. However, despite these equable improvements, females continued to be discharged with higher NIHSS compared to males. Based on our study results, this is unlikely to be explained by sex treatment bias either in the pre-hospital or hospital setting. This conclusion aligns with other studies that have also reported poor stroke outcomes for females, which seem to be related to other confounding factors. A previous study analyzing the sex gap and differences in stroke outcomes found that while females were more likely to have poor outcomes, sex itself was not associated with unfavorable outcomes. Rather, females were more likely to present with severe stroke symptoms with a higher mean age, which were both independently predictive of poor outcomes. 3 Similarly, in our analysis we noted that females presented with initially higher NIHSS and a significantly higher mean age, therefore we would expect that discharge NIHSS, a measure of stroke outcomes, would also be higher. The notion that sex is not independently linked with poor outcomes is further substantiated by a study analyzing the efficacy of EVT between sexes. EVT, when appropriately implemented, is equally effective for both females and males. 11
Interestingly, we also found that females tended to have higher initial calculated FAST-ED scores and NIHSS compared to their male counterparts, a finding that differed from prior studies suggesting females may score lower due to atypical symptoms. 4 It is important to note, that in our study the NIHSS was assessed in the hospital setting and the calculated FAST-ED score was derived from that initial NIHSS. Therefore, the observed sex differences between the later acquired first hospital NIHSS and the reported EMS FAST-ED score may be related to rate of stroke progression. In our study we found that female FAST-ED difference scores were significantly lower compared to male scores, indicating that stroke symptoms from EMS initial assessment to hospital arrival stayed the same or increased. Another study found that females may actually have a higher disease burden at onset with symptoms that are not scored on the FAST-ED (e.g., headaches, blurry vision).7, 12 Therefore, when females are evaluated at the hospital, their NIHSS may be higher due to inadequate symptom scoring and subsequent disease progression during transit. Another theory is that variance in premorbid conditions between females and males may further lend itself to discrepancies in NIHSS. Therefore, females may have presented with elevated NIHSS due to a potentially greater degree of sex-specific premorbid risk factors than their male counterparts. 3 A similar parallel is noted in females diagnosed with STEMIs, wherein, females were older with greater co-morbidity at presentation and, therefore, had worse outcomes. 13 However, more research into the field would be necessary for identification of a true cause.
Our study reflects real-life results from a comprehensive stroke certified community hospital that serves a predominately Hispanic population. Limitations of our study includes its single center retrospective design with little access to pre-stroke health information and the limited availability of the reported EMS FAST-ED score. Notwithstanding these limitations, in our community, we found no evidence of sex or ethnic disparities in the implementation or score assessment of the FAST-ED initiative or with acute stroke treatment in either the pre-hospital or hospital setting. While we did find some evidence of sex disparities when assessing stroke severity, additional research is needed to confirm these results.
Footnotes
Acknowledgments
This study was support by the Miami Neuroscience Institute of Baptist Health South Florida. We would like to extend thanks to all the staff and research volunteers that aided with data collection.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Waivers of informed consent and HIPAA authorization were granted by a local Institutional Review Board (BHSF1667091). This study involved no direct patient contact.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
This was a retrospective study that was granted a full waiver of consent by the local Institutional Review Board (BHSF1667091).