
Abstract
The stroke burden in India is alarmingly high compared to Western industrialised countries, necessitating immediate action to develop stroke systems of care. Tailored stroke-prevention strategies, adequate resource allocation for stroke management and research, and increased awareness of specialised care in acute Stroke are critical. The COVID-19 pandemic has underscored the need for improved healthcare delivery and infrastructure. To address the rising stroke burden in India, comprehensive strategies encompassing prevention, awareness, specialised care and governmental support are urgently required. While the concept of ‘stroke-ready centres’ has emerged, their limited availability hinders widespread benefits. This expert consensus examines the current state of stroke care in India, identifies challenges, and proposes strategies to enhance stroke care systems. It offers valuable insights into stroke management at different levels, empowering healthcare professionals and administrators to assess their existing systems and make necessary improvements. Special attention is given to the role of physicians, including the use of thrombolytic therapies like Tenecteplase, in reducing the stroke burden and improving outcomes across the country. Significant strides can be made in stroke management and care in India by addressing these critical areas.
Introduction
Stroke Epidemiology Global Versus Indian
Stroke is the second-leading cause of death worldwide and the third-leading cause of death and disability combined of total disability-adjusted life-years (DALYs). Globally from 1990 to 2019, there was a rise of 22.0% (with a range of 21.0%–24.0%) in the prevalence rates and a 15.0% increase (with a range of 12.0%–18.0%) in the incidence rates among individuals under the age of 70. 1 Stroke imposes a greater burden on low- and middle-income countries (LMICs) compared to high-income countries, and this burden is increasing. 2 Stroke has a high prevalence in the South Asian region, which comprises India, Pakistan, Sri Lanka and Bangladesh. The incidence of stroke is particularly high in younger individuals in this region, and short-term mortality rates from stroke are also elevated. 3
In India, stroke accounts for 7.3% of deaths and is a significant cause of disability, contributing to 3.5% of DALYs.4, 5 According to a study conducted in a comprehensive stroke unit (SU) in South India, it was observed that women tend to experience more severe strokes compared to men. Men were more prone to large artery atherosclerosis, whereas women were more likely to develop cardioembolic strokes due to rheumatic heart disease. 6 As per the Hyderabad stroke registry, the pattern of ischemic stroke subtypes in India is similar to registries from West and East Asian countries. The registry indicates a significant occurrence of large artery and small vessel diseases, with intracranial atherosclerosis being the most prevalent. 7
The INTERSTROKE study emphasised that many strokes can be attributed to modifiable risk factors, including high blood pressure, smoking, poor diet and lack of physical activity. 8 India is expected to experience a rise in the burden of stroke owing to changes in demographics and lifestyle. The rise in India’s aging population 9 is primarily responsible for increased deaths due to ischemic heart disease and stroke. 10 As per the Trivandrum Stroke Registry, stroke patients living in rural areas are disadvantaged regarding optimal investigation and treatment compared to their urban counterparts. A comparison of stroke incidences between North and South India indicated that the traditional vascular risk factors are more prevalent in the South. 11
Data from the Indo-US Collaborative Stroke Project (IUCSP) and China National Stroke Registry-II of hospitalised ischemic stroke patients revealed that Indian patients with stroke were younger and had a distinct set of risk factors, with a higher incidence of diabetes mellitus, dyslipidaemia and coronary heart disease, and a lower incidence of prior stroke, hypertension, atrial fibrillation (AF) and smoking. 12
Status of Health Care and the Challenges in India
Stroke care in India faces multiple challenges, including limited stroke education and awareness among the population,13, 14 regional disparities and the rural-urban divide,15, 16 a divide between public and private healthcare models, a shortage of healthcare professionals, obstacles at the patient level, transportation-related challenges and issues within hospitals such as the need for more specialised healthcare providers and dedicated SUs. 17 These challenges highlight the urgent need for comprehensive strategies to improve stroke care accessibility, awareness and infrastructure throughout the country.
This expert consensus aims to outline the status of stroke care in India, identify the obstacles encountered, and identify avenues to enhance stroke care systems. It provides insights into managing stroke at various levels, enabling healthcare practitioners and administrators to evaluate their care systems and restructure them accordingly to improve stroke management.
Methodology
A virtual, multidisciplinary focused group discussion involving neurologists, stroke specialists and neurosonologists was organised. The experts explored, brainstormed, on various issues related to the stroke ecosystem in India and issued and agreed on common consensus statements towards improving the stroke care ecosystem in India. A senior neurologist and stroke specialist played the role of moderator. Similarly, senior neurologists and stroke specialists chaired the discussion.
Stroke System of Care
Efforts to alleviate the burden of stroke require healthcare providers, hospitals and communities to collaborate in developing systems that improve the efficiency and effectiveness of stroke care.
Understanding the entire spectrum of stroke care, including prehospital, intrahospital and post-hospital aspects, is crucial for achieving optimal outcomes. 17 This includes recognising the stroke chain of survival 18 and emphasising the importance of early intervention and management.
The ‘8 D’ approach to stroke chain survival involves
Early detection, Swift dispatch of emergency services, Timely delivery to a stroke-ready facility, Prompt evaluation and treatment at the hospital (door), Data collection, Expert decision-making, Appropriate drug administration and Comprehensive post-stroke care (disposition).
18
Delayed recognition of stroke as an emergency, lack of awareness about the importance of timely treatment, underutilisation of intravenous thrombolysis (IVT) and referral delays are the main issues affecting acute stroke management pathways in India. 19
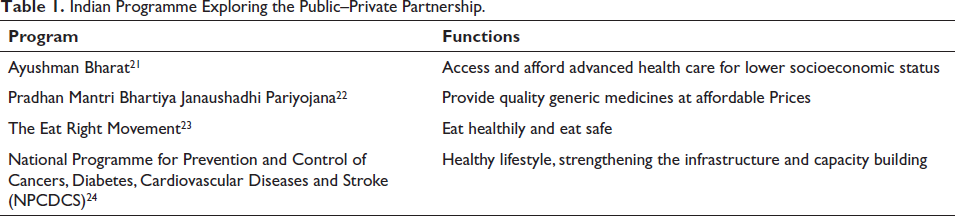
The government and non-profit organisations 20 should plan stroke awareness programs at the national level. By integrating physicians into the national stroke program, their full potential can be harnessed in the fight against stroke at the national level and will create a skilled workforce that can contribute significantly to the program’s success. Indian programs that aim to explore the potential for public–private partnerships (Table 1) in stroke care lead a healthy lifestyle, strengthen the infrastructure and capacity building and ensure accessibility of high-quality generic medicines at affordable prices.
Indian Programme Exploring the Public–Private Partnership.
Collaboration for Improved Stroke Care
Collaboration is essential for improving stroke care, which includes ensuring timely and coordinated care, reducing errors and delays and ultimately improving patient outcomes.
Stroke care unit (SCU): SUs are specialised hospital units for acute care and rehabilitation of stroke patients. Staffed by a team of healthcare professionals, including neurologists, nurses and therapists, SCUs provide basic brain imaging, intensive monitoring and specialised stroke care. 25 SU care has been shown to significantly reduce mortality and disability following a stroke, compared to conventional care given in a general ward. This effect on survival is evident early after the stroke and continues for at least 18 months of observation. 26
Hub-and-spoke model: In 2018, the ‘Save the Brain Initiative’ suggested implementing a ‘spoke and hub’ model in urban India for managing acute stroke and administering IV thrombolysis. 27 The hub-and-spoke model (Figure 1) involves providing specialised care to patients in community settings (spokes) through specialists associated with larger, more comprehensive tertiary care centres (hubs). Vascular neurologists and other acute stroke specialists form a call panel at the hubs to offer Telestroke services.
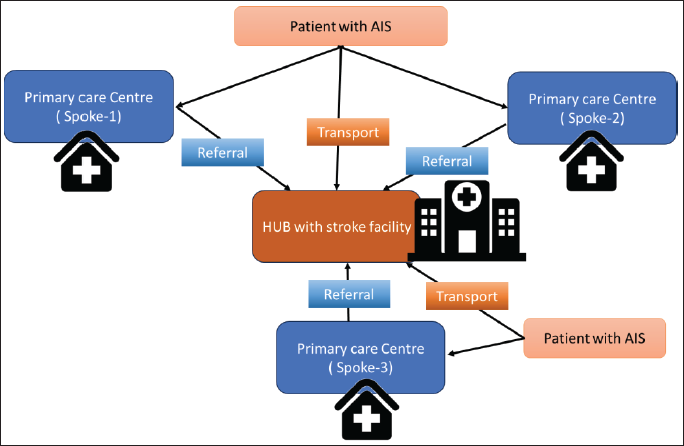
The ‘hub and spoke’ model has been successful globally. It increased thrombolysis access in southwest London and showed comparable outcomes to comprehensive institutions in New York State. The spoke hospitals consistently met high standards in stroke care compared to the standard hub hospital.28, 29
In India, the hub and spoke model improves thrombolysis rates and outcomes by sensitising healthcare providers and implementing a standard stroke management protocol. Hub hospitals provide SU care and thrombolysis through direct consultations, preventing overburdening of higher-level healthcare systems with ineligible patients. 30
Mapping of Stroke Centres
The process of mapping stroke centres aids in identifying existing facilities for rapid referral and treatment, leading to reduced treatment time and improved outcomes. Additionally, mapping reveals areas lacking stroke care infrastructure, allowing policymakers to allocate resources and establish new centres. Mapping enables prompt emergency response, quickly transporting patients to suitable stroke centres. Studies show that patients admitted to designated stroke centres have lower mortality rates and increased utilisation of thrombolytic therapy. 31
Telecommunication Approaches Between SUs and the Stroke Centre
Telecommunication methods, such as teleradiology, smartphone applications and Telestroke assessment, enable real-time remote specialist advice between SUs and stroke centres. Teleradiology allows the transmission of high-quality images for remote diagnoses and medical consultations. Mobile apps link stroke centres, ensuring quick access to neurologists, seamless image sharing and prompt large vessel occlusion (LVO) referrals. Telestroke services, structured in a hub-and-spoke model or distributed network, address the limited availability of neurologists in remote areas. These technologies provide valuable support, especially in regions with sparse populations.
32
There are various Telestroke models in different states of India (Table 2).
Telestroke Model in Different States of India.
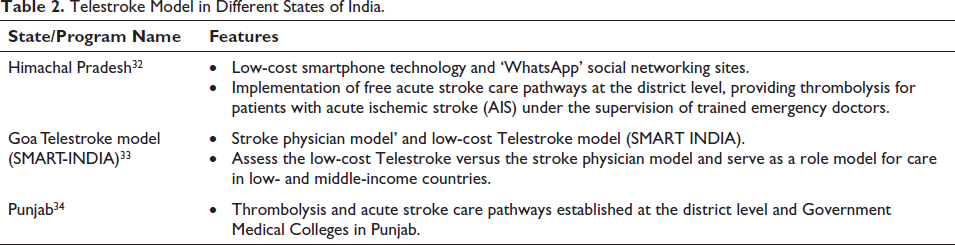
However, Telestroke implementation in India faces barriers such as limited internet connectivity, lack of specialised equipment and trained healthcare professionals in rural areas, high initial and maintenance costs, insufficient funding for telemedicine research, and a need for clearer regulations and guidelines. Potential solutions to overcome barriers include implementing community education and awareness programs, fostering public–private partnerships and philanthropic organisations, adopting the ‘hub and spoke’ model, geotagging stroke-ready hospitals and establishing a dedicated nationwide helpline number.
32
A Taiwanese retrospective study on a smartphone application for interhospital transfer in thrombectomy for large vessel occlusion (LVO) acute ischemic strokes (AIS) showed a decrease in door-to-puncture time from 109.3 to 92 minutes over three years (p = .045), with increased thrombectomy cases.
35
A Brazilian study supported the efficacy of a similar app, suggesting timely data review can be as accurate as the physical presence of stroke experts.
36
A review by Bonura et al. found mobile apps beneficial in stroke care but highlighted a need for more interactive systems for clinicians in primary prevention, acute management and post-acute stroke care.
37
Prevention of Stroke
Primary Prevention
Primary stroke prevention aims to reduce the risk of experiencing a stroke by managing established disease risk factors such as hypertension, hyperlipidaemia, AF and asymptomatic carotid stenoses. It involves routine care that includes screening for risk factors, medication management 38 and AF screening for, older individuals or those with additional risk factors.
Carotid ultrasound is used to diagnose carotid disease and assess the likelihood of carotid stenosis during primary prevention. Regular screening of asymptomatic patients is not advised. However, if carotid stenosis is suspected or atherosclerosis is present in other vascular areas, carotid ultrasound can aid in appropriate treatment and stroke prevention. 39
As a part of the Indian Government’s Non-Communicable Diseases (NCD) policy, the 2022 guidelines from the Ministry of Health and Family Welfare define the roles of Accredited Social Health Activist (ASHA) and Auxiliary Nurse and Midwife (ANM) in stroke prevention. ASHA workers are vital at the population level, conducting community-based risk assessments, creating awareness about stroke signs and symptoms and referring cases with high glucose and blood pressure for proper management. 40
Secondary Prevention
Secondary Prevention in Structured Semi-Interactive Stroke Prevention Package in INDIA (SPRINT INDIA) trial aimed to assess the effect of a structured semi-interactive stroke prevention package in patients with subacute stroke to reduce recurrent strokes, myocardial infarction, through a one-year program utilising SMS, video messaging and workbooks. Data supported its usefulness in drug adherence and lifestyle behaviour including smoking and alcohol use.41, 42 However no significant difference in the primary composite outcome between groups was observed (5.5% in the intervention group vs. 4.9% in the control group; p = .370). 43 Randomised trial data also supports the treatment of hypertension, carotid endarterectomy for symptomatic carotid stenosis, and management of acute stroke patients within structured SUs. 44
Role of Neurologists in the Prevention and Management of Stroke
The National Stroke Association characterises the role of stroke neurologists in stroke diagnosis, treatment and prevention. In secondary prevention, they directly manage risk factors such as blood pressure, AF, prescribe medications like statins, carotid stenting or endarterectomy.
45
They also play a crucial role in identifying risk factors, providing advice, integrating risk reduction into treatment plans and utilising community resources for stroke prevention.
42
Stroke accreditation program in collaboration with the Quality Accreditation Institute, which aims to certify stroke centres at the district and primary level for their ability to provide thrombolysis treatment.
Need for certification at the primary stroke centre level, A collaboration between primary and advanced stroke centres, The establishment of national assessors for the program, The invitation of neurologists to attend a session to understand the program, The empowerment of primary stroke centres to receive accreditation for their treatment capabilities. The centre should have the capability of performing at least a non-contrast computed tomography (NCCT) scan 24 × 7. In hospital.
For neurologists-Fellowship programs in neuro interventions. Training physicians for Acute stroke management. Neurologists and stroke specialists need to reach out and educate emergency room doctors and other physicians to improve stroke treatment.
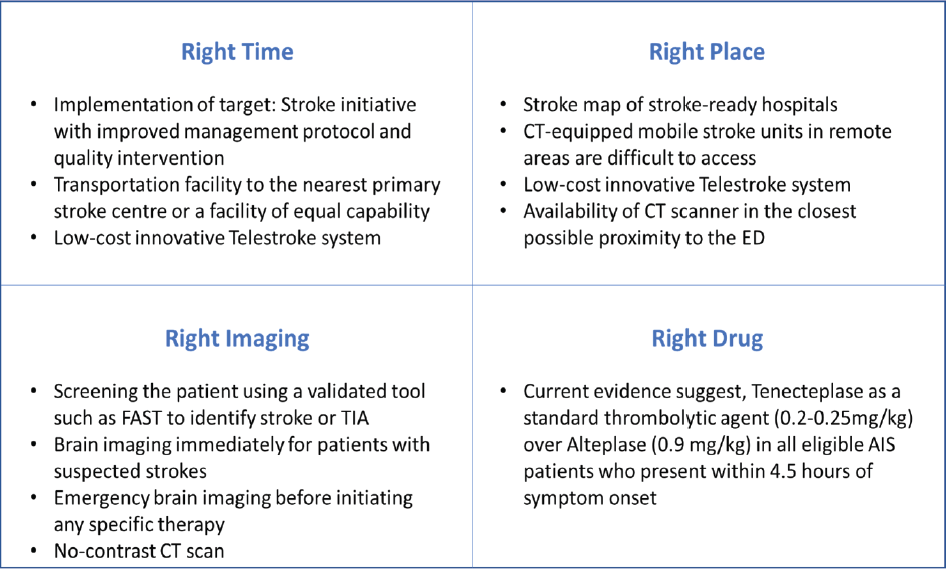
Concept of Right Time, Right Place, Right Imaging and Right Drug in AIS
Right Time (Transport Time)
The expression ‘Time is Brain’ highlights the importance of urgent evaluation and treatment for stroke, as the loss of human nervous tissue occurs rapidly during the progression of the condition. The typical patient loses 1.9 million neurons each minute in which stroke is untreated. 46 In India, the limited availability of structured ambulance services and trained paramedical staff delays stroke patient transportation. Mobile SUs (MSUs) offer a solution by providing specialised ambulances equipped with personnel and equipment to diagnose and treat acute stroke in the prehospital setting. Trials have shown that MSUs improve stroke management, ensuring safety and better functional outcomes. Studies indicate higher thrombolysis rates within the golden hour, accurate triaging to appropriate stroke centres, reduced disability at three months and prompt treatment delivery. MSUs improve stroke outcomes and play a crucial role in providing timely and effective care.47–50
However, several barriers hinder the widespread expansion of MSUs, including financial implications and inefficiency. Financial considerations encompass program costs, operations, medication and infrastructure. In India’s low-resource setting, focusing on strengthening EMS services to connect with stroke-ready hospitals is a practical first step, considering the considerable cost (1 million USD to purchase and up to 1 million USD per year in operational expenses) of MSUs. The use of MSUs can be explored on a need basis. 51 Enhancing public awareness and gaining government support, including subsidies for treatment costs, can accelerate the development of effective prehospital acute stroke care policies in India. 50
Right Time: Door-to-needle (DTN) Time
Timely administration of thrombolysis is crucial to reduce disability and dependence in patients with AIS. It is the most effective and definitive treatment for eligible patients, providing improved functional outcomes at three and six months when given within 4.5 hours of symptom onset. 42 Guideline recommends DTN times of <60 minutes. 52
Shortening the DTN time (≤60 minutes) for thrombolytic treatment is associated with lower mortality rates. 53 Even a 15-minute decrease in arrival-to-thrombolysis time correlates with a 5% decrease in in-hospital mortality odds. 53 According to the Himachal Pradesh acute coronary syndrome registry, an increase in DTN time delay by 1 hour resulted in a 20% increase in the hazard ratio of death. 54
Delays in prompt thrombolytic treatment can be attributed to various patient and hospital factors. Patient-related reasons for delay commonly include the delay in symptom identification. On the other hand, system-related factors often involve waiting for laboratory results, delays in CT scans, diagnosis or review of advanced imaging before a thrombolysis decision. 55
Strategies to improve DTN times, as per literature evidence are:
American Heart Association/American Stroke Association’s (AHA/ASA) Target: Stroke initiative shared strategies, provided decision support tools, promoted hospital engagement and encouraged best practice sharing to accelerate thrombolytic administration for faster DTN times.
52
Telestroke can offer patients in rural hospitals similar or shorter DTN compared to those who directly visit tertiary care centres after experiencing stroke symptoms.
56
Quality-improvement interventions such as single call notification, prioritising patients for CT scanning, lab analysis, providing ICU beds and conducting staff education have significantly resulted in an acceptable DTN time.
57
A significant improvement in DTN using the mobile app as a tool to improve team performance.
58
Right Place
The definition of the right place should be a centre where stroke care is set up for the management and monitoring of stroke patients including neurologists, nursing care, basic stroke imaging facilities, thrombolytic administration and rehabilitation services are available. Comprehensive Stroke Care (CSC) centres should have interventional facilities. SUs should have collaborate with CSC in case rapid referrals are required. Geotagging should enable patients to know the location of SU and CSC to arrive at the right place on right time (Figure 2).
Proposed Geotagging of Stroke Care Units and Comprehensive Stroke Care Units.
Right Drug: Tenecteplase reduces DTN Time
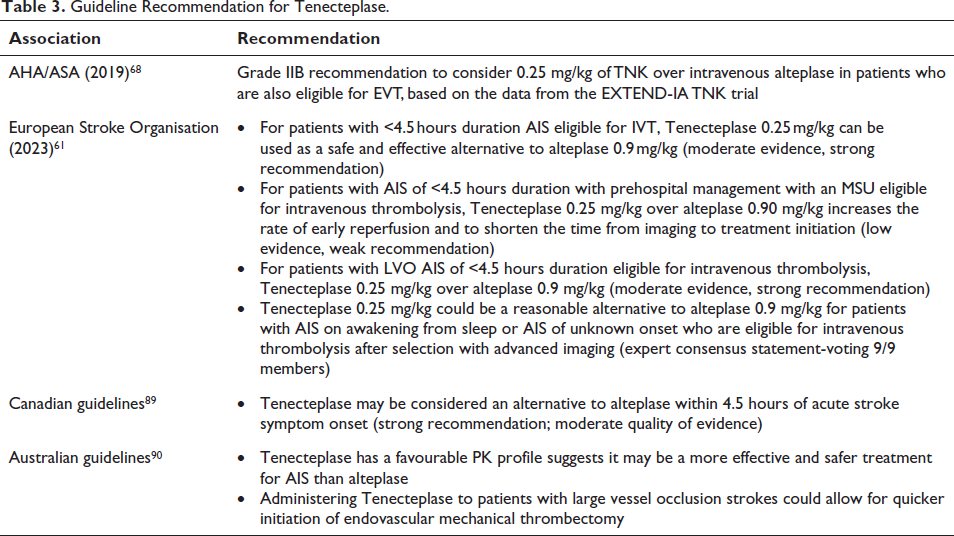
Tenecteplase and alteplase are the recommended first-line thrombolytic agents for the treatment of acute ischemic stroke.
59
TENVALT study reported Tenecteplase as a cost-effective and easily administrable option for thrombolysis in stroke treatment, which could serve as a viable alternative to alteplase, sole fibrinolytic therapy approved for AIS.
60
A recent 2023 ESO recommendation also suggests that for individuals who have experienced an AIS within 4.5 hours, the use of Tenecteplase at a dosage of 0.25 mg/kg may be ‘favoured’ over alteplase at a dosage of 0.9 mg/kg due to similar effectiveness and safety profiles as well as ease of administration.
61
Patients treated with Tenecteplase had faster transfer times between hospitals for mechanical thrombectomy (MT), resulting in a shorter time between thrombolysis and puncture (84 minutes compared to 95 minutes, with a p = .02).
62
Tenecteplase treatment resulted in a significantly shorter DTN time compared to other treatments (41 vs. 58 minutes; p < .01) and had a similar incidence of symptomatic intracranial haemorrhage (2% vs. 7%, p = .37) which may be due to the ease of administration of Tenecteplase in a single bolus.
63
An Indian study evaluating Tenecteplase for AIS treatment, reported an average DTN time of 76.7 minutes from patient arrival to receive the injection.
64
Compared to standard therapy, Tenecteplase has a faster preparation time, improving performance. It takes 10.5 minutes less to prepare than the standard treatment (p < .001), which may result in a clinically significant increase in survival by reducing the DTN time.
65
Administering Tenecteplase in an MSU leads to better reperfusion upon hospital arrival than alteplase.
66
Right Imaging
Timely and accurately identifying the type of stroke soon after the symptoms appear is essential to prompt the administration of suitable therapy. The crucial diagnostic step before initiation of treatment is cerebral imaging which is critical to differentiate stroke types and rule out mimics, ensuring prompt administration of appropriate therapy. NCCT should be the primary investigation in suspected patients. Magnetic resonance imaging (MRI) including Perfusion studies can done subsequently as required. 67
2019 AHA/ASA stroke guidelines suggest using non-contrast CT or MRI with diffusion-weighted imaging (DWI) to conduct an initial assessment. 68 Follow-up imaging is done with contrast-enhanced CT angiography (CTA) or magnetic resonance angiography (MRA) to identify patients eligible for endovascular thrombectomy if they have LVO.69, 70 Penumbral imaging also detects discrepancies between the core infarction and the potentially recoverable penumbra. 71
When ensuring the right imaging, possible strategies to improve door-to-imaging time (DTI) are the following:
Implementing an all-points alarm system significantly reduced the median time for DTI in eligible thrombolysis patients from 54 to 35 minutes.
67
Educating emergency department staff about stroke care significantly improves all acute stroke care quality measures.
72
Median DTI times decreased from 114 to 35 to 47 minutes over three consecutive phases.
73
Due to the lack of stroke education programs for the general public in India, DTI time was reported to be considerably longer than the recommended guidelines by AHA.
74
To enhance the promptness of acute stroke care, it is essential to prioritise enhancing stroke-specific care processes and initiatives to reduce overcrowding in the emergency department.
75
Relocating the CT scanner to the nearest location to the emergency department significantly impacted door-to-head CT scan time.
76
Implementing stroke codes in hospitals improves IV thrombolysis rates and reduces DTN time in AIS, decreasing at least 60 minutes in DTI time.
77
Right Drug: Thrombolysis
In India, only 35–50 Sus are available, and nearly 2,000 patients receive thrombolysis every year due to various challenges. 78 Most stroke patients cannot receive thrombolysis due to delayed hospital arrival, lack of early access to scanning facilities, inadequate infrastructure and high cost of thrombolytic and/or endovascular therapy. 79 Following the emergence of the COVID-19 pandemic, there was a 6.1% absolute reduction in IVT. 80
A wealth of evidence is available for Tenecteplase (0.2–0.25 mg/kg bolus) and alteplase (0·9 mg/kg, 10% bolus remaining infusion) in thrombolysis. In AIS patients who meet the standard criteria for thrombolysis, intravenous Tenecteplase is a reasonable alternative to alteplase. 81 In India, Tenecteplase has been approved at a dose of 0.2 mg/kg within 3 hours of stroke onset. 82 Tenecteplase has a 15 times higher fibrin specificity and a longer half-life than alteplase. 83
Following is evidence comparing both thrombolytics
TETRIS registry: Tenecteplase patients had a shorter imaging-to-thrombolysis time (27 vs. 36 min, p < .0001 compared to those who didn’t receive it, especially in patients treated at the CSC.
62
TASTE-A trial: Patients who received Tenecteplase had significantly smaller perfusion lesion volumes (median 12 mL [IQR 3–28]) upon arrival at the hospital compared to those who received alteplase (35 mL).
99
Trace-2 trial: Tenecteplase was as effective as alteplase in patients with ischemic stroke who could not undergo or refused endovascular thrombectomy.
84
Biosimilar Tenecteplase versus alteplase was evaluated in Indian patients
85
with AIS, and no difference was found in efficacy and safety both.86, 87 The retrospective study involved collecting data from consecutive AIS patients who reported Tenecteplase at a dose of 0.2 mg/kg is safe and efficacious for the thrombolysis of AIS during the 4.5-hour window period.
88
The guideline recommendation for Tenecteplase (TNK)is mentioned in Table 3.
Guideline Recommendation for Tenecteplase.
LVOs and MT
MT is highly effective for treating LVO in AIS, which frequently involves blockages in the proximal intracranial circulation. Five trials: SWIFT PRIME, REVASCAT, MR CLEAN, EXTEND-IA and ESCAPE have reported the superiority of MT using stent retrievers over the best medical management using IVT.91–93 An Indian study of 137 patients with LVOs found MT safe and efficacious for both the anterior and posterior circulation (AC and PC) LVO. 94
The usual treatment for LVO-related AIS is IVT followed by MT (bridging therapy, BT). A recent systematic review and meta-analysis comparing BT and direct MT for AIS with LVO found no significant difference in mortality and functional outcome after 90 days. 95 As per Indian guidelines, AIS patients with LVO may be considered for bridging IV thrombolysis (alteplase 0.9 mg/kg infusion or Tenecteplase 0.2–0.25 mg/kg bolus) followed by MT. 96
In India, MT costs approximately 400,000–500,000 INR. However, India’s average per capita income is only 126,406 rupees annually, highlighting affordability and access. To improve MT for stroke care in India, it is suggested to integrate MT training in neurology/neurosurgery and interventional radiology programs. Establishing a national EMS service, educating them about identifying LVO stroke, and creating a network of stroke care centres can reduce response time. Additionally, hospital-based stroke registries provide valuable insights into the quality of acute stroke care. One potential solution to address the cost issue is to consider capping the price of thrombectomy devices. 97
A summary of recommendations for the right time, right place, the right image and the right drug has been mentioned in Figure 3.
Recommendations for the Right Time, Right Place, Right Image and Right Drug for Stroke.
Future Strategies in Stroke Care in India
Artificial Intelligence (AI) and Digital Advancement for Stroke
AI technology shows great potential in acute stroke imaging, aiding in the detection of ischemic and haemorrhagic subtypes and assisting with tasks like infarct and haemorrhage detection, image segmentation and identification of LVOs. Additionally, a cost-effective diagnostic tool using real-time electromyography signals and AI technology has been developed, offering real-time stroke prediction and the possibility of diagnosing other conditions like heart disease.98, 99 In India, a lot of AI and digital advancement is happening. The IUCSP is one such program which integrates high-volume stroke centres in India with centres in the USA, expanding the network of collaborative stroke centres for more efficient therapeutic trials. 100 The MAMOR (Medication-Adherence and Management of Risk Factors) app is a smartphone-based innovation designed to enhance stroke awareness and medication adherence in LMICs with limited resources. It provides health education materials, reminders and physician intervention for effective secondary stroke prevention. 101
Strengthening Peripheral Health and Human Resources
The Global Stroke Guidelines and Quality Committee were created by the World Stroke Organization to aid stroke care, particularly in regions where healthcare resources are scarce. To enhance stroke care in India, key steps include establishing stroke centres in district-level referral hospitals, integrating health programs, educating primary health workers on stroke alongside antenatal care, implementing common protocols for stroke, STEMI and trauma, and fostering government partnerships with the private sector. Involving socio-religious leaders and celebrities is crucial for stroke education and awareness. A comprehensive communication strategy is needed to encourage public ownership and control of vascular risk factors for better brain health.
IMPETUS: Implementing a Uniform Stroke Care Pathway in Medical Colleges of India: IMPETUS Stroke is a study to assess the feasibility of real-world implementation of a uniform stroke care pathway in hospitals associated with medical colleges in India. The study aims to enhance stroke care from emergency recognition to patient discharge by employing an implementation design. 102
Advancement in the Management of Stroke
Advancements in Neuroimaging
Recent trial designs and clinical practices have explored additional imaging modalities for enhanced tissue viability assessment and patient selection for reperfusion interventions. The DWI/fluid-attenuated inversion recovery (FLAIR) mismatch has been confirmed in patients with unclear symptom onset times. Administering IV thrombolytics guided by a DWI/FLAIR mismatch led to significantly improved functional outcomes at 90 days. 103 Several prospective studies have validated the use of perfusion imaging to identify reperfusion-eligible patients beyond the conventional 4.5-hour window. 104
Advancements with Fibrinolytic
Extensive data, including two large phases three trials, have firmly established Tenecteplase as a suitable and more convenient option for AIS. Tenecteplase has an 80-fold higher PAI-1 resistance, allowing for a bolus intravenous administration over 5 seconds. This may reduce medication errors and nursing resources. Tenecteplase has a 15-fold higher specificity for clot-bound fibrin, potentially resulting in a lower risk of systemic fibrinogen depletion and bleeding. Evidence supports Tenecteplase as an appropriate treatment for AIS at 0.2–0.25 mg/kg push. It appears superior to alteplase for patients with LVOs undergoing thrombectomy. Ongoing trials, that is, ATTEST2, BRIDGE-TNK, Nor-TEST 2 part B, TEMPO 2 will evaluate its efficacy and safety. 105 TIMELESS trials failed to show benefit beyond 4.5 hours for Tenecteplase although results of other studies evaluating benefit beyond 4.5 hours are awaited. 106 Tenecteplase is now approved for use up to 4.5 hours of stroke onset in India.
Incorporating Tenecteplase in Healthcare Systems
Health systems are considering incorporating Tenecteplase into their stroke care protocols, following potential benefits in patient outcomes compared to alteplase for AIS. Apart from the ease of administration and dosing, the benefits of Tenecteplase in patients undergoing thrombectomy and cost savings for institutions and patients drive the transition to Tenecteplase therapy.
Advances in Pharmacotherapy of Acute Ischemic Stroke
Sovateltide, a selective endothelin-B receptor agonist, received approval in India in May 2023 for treating strokes within 24 hours of onset. 107 In a Phase III study with 158 AIS patients, the sovateltide group showed a significant increase in the number of patients with a ≥2-point improvement in modified Rankin scale (p = .004) and ≥6-point improvement in the National Institute of Health Stroke Scale (p = .033) at 90 days. 108 DL-3-n-butylphthalide (NBP), another neuroprotective agent with Phase III data, demonstrated efficacy in a multicentre trial in China. Among 1,236 AIS patients treated within 6 hours, those receiving NBP in conjunction with intravenous rt-PA or endovascular treatment had a significantly higher favourable functional outcome at 90 days (56.7%) compared to the placebo group (44.0%), with an odds ratio of 1.70 (95% CI, 1.35–2.14; p < .001). 109 Neuroprotective agents targeting the process of oxidative stress, mitochondrial damage, apoptosis or ferroptosis-related cell death, inflammatory response and disruption of the blood–brain barrier are under evaluation. 110
Advancements in Thrombectomy
MT has advanced treatment for anterior LVO by removing clots. Guidelines recommend it within 24 hours of the last known normal for those with LVO in the anterior circulation who meet DAWN or DEFUSE 3 criteria. 68
Summary
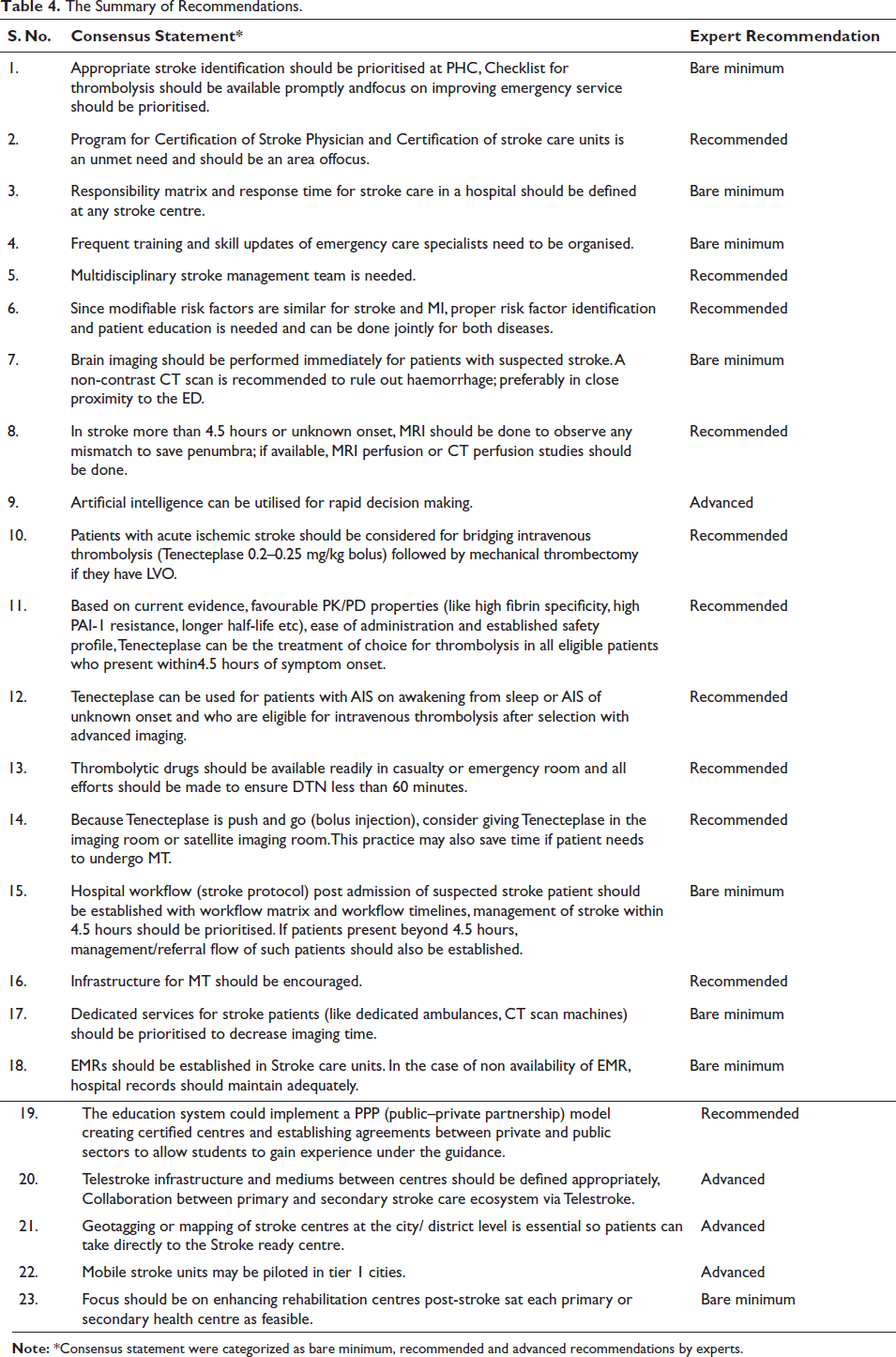
India is currently experiencing a high incidence of stroke, unlike industrialised Western countries where stroke rates have declined. This is primarily due to inadequate control of common risk factors such as hypertension, diabetes, smoking and dyslipidaemia, coupled with low public awareness. To address this challenge, comprehensive strategies are urgently needed in India, including prevention efforts, increased awareness, specialised care and government support. Promising models of stroke care in LMICs offer the potential for improved outcomes. Access to effective treatments like thrombolysis and thrombectomy requires subsidised funding from the government. In the absence of these treatments, establishing modified SUs with trained professionals is essential. Integrating stroke care services into national NCD programs can pave the way for widespread implementation. It is crucial to take decisive action to combat the growing burden of stroke in India. A summary of recommendations is mentioned in Table 4.
The Summary of Recommendations.
Footnotes
Acknowledgements
The authors of this guideline have granted their final approval for the recommendations. The authors would like to acknowledge Dr Punit Srivastava and Dr Nidhi Gupta from Mediception Science Pvt Ltd (
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. Ankush Gaikwad and Sachin Suryawanshi are employees of Emcure Pharmaceutical Ltd.
Ethical Approval
Ethics approval not applicable since no animal or human participants involved.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed consent was not applicable since all data is gathered from published sources.