
Abstract
59-year-old male had four episodes of transient, painless vision loss in right eye in the last 20 days which had resolved spontaneously. Three years ago, patient had been diagnosed with oropharyngeal squamous cell carcinoma, which had been treated with six cycles of chemotherapy and radiotherapy. MRI brain angiogram showed diffuse long segment wall thickening of Right Internal Carotid Artery with luminal narrowing with no acute infarct or haemorrhage; which was later confirmed by four vessel DSA. He was treated with Right Carotid Artery angioplasty with a cutting balloon while using a distal protection device, followed up by stenting. The patient recovered well on follow-up and there were no further episodes. Thus, amaurosis fugax may be a presentation of carotid artery stenosis, especially after radiotherapy and such patients can be treated by carotid angioplasty and stenting.
Key Message
Amaurosis fugax may be a presentation of carotid artery stenosis especially after radiotherapy and such patients can be treated by carotid angioplasty and stenting.
Case
A 59-year-old male, presented with complaints of four episodes of transient loss of vision in the right eye since the past 20 days which was painless, lasting for a few seconds and without any associated complaints of headache, diplopia, facial or limb weakness or sensory complaints. These episodes resolved spontaneously and completely. The patient had past history of oropharyngeal squamous cell carcinoma of stage T2 N2b M0, three years ago, for which he had received six cycles of cisplatin-based chemotherapy along with radiotherapy (45 Gy to neck and 70 Gy to the primary lesion). He was non-diabetic and non-hypertensive without any history of previous strokes. At presentation, his neurological examination was normal with no focal neurological deficit.
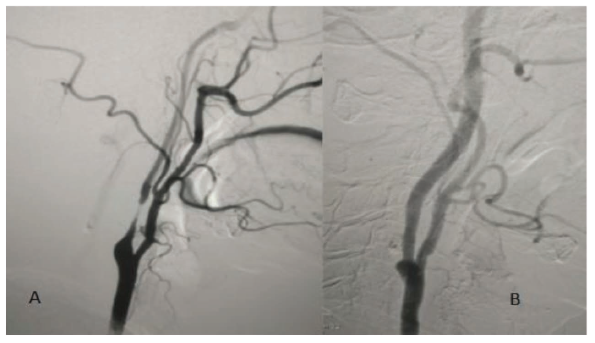
The patient was investigated further. MRI brain with angiogram was suggestive of diffuse long segment wall thickening with luminal narrowing of Right Internal Carotid Artery without any acute infarct or haemorrhage. Carotid Doppler study was suggestive of concentric stenosis causing 90% of luminal occlusion of Right Internal Carotid artery. These findings were confirmed by a four-vessel digital subtraction angiogram (Figure 1). Routine lab investigations including CBC, LFT, RFT, serum homocysteine, serum lipid profile and coagulation profile were normal. 2D Echocardiography was normal with an ejection fraction of 60% with normal chamber sizes. In view of the repeated episodes of amaurosis fugax, the patient was planned for Right Carotid Angioplasty.
A: Right CCA Angiogram Showing Long Segment Luminal Narrowing (90%) of the Right Internal Carotid Artery. B: Left CCA Angiogram Showing Mild Narrowing of the Left ICA.
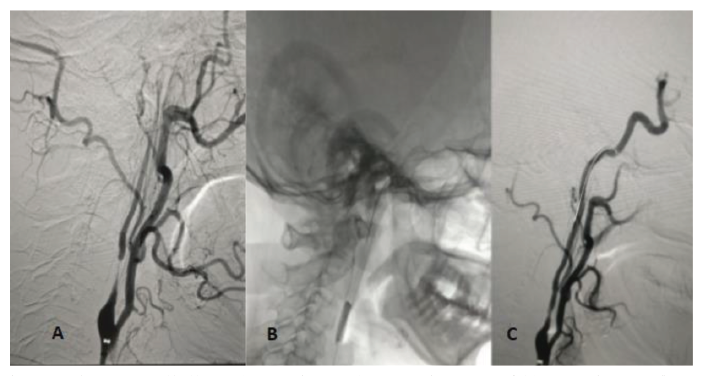
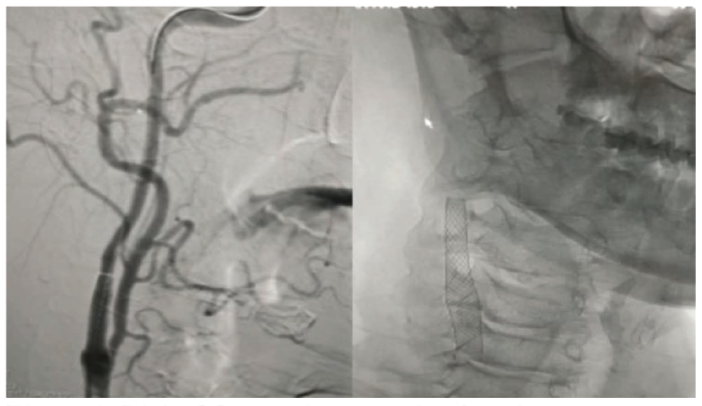
Under all aseptic precautions, the patient underwent Right Carotid Artery angioplasty using a cutting balloon (Boston Scientific 3 × 30 mm followed by 5 × 30 mm) using a distal protection device (Figure 2). This was followed by stenting (Wall Stent 8 × 40 mm) (Figure 3). The procedure was uneventful. Following the procedure, the patient was started on injectable Low molecular weight Heparin at dose of 0.6 ml subcutaneously twice a day for two days and then shifted to dual antiplatelets (Tablet Aspirin 150 mg OD and Tablet Clopidogrel 75 mg OD) and atorvastatin 40 mg once a day. On discharge, the patient was vitally stable and Dual antiplatelets and statin were advised to be continued. At three months of follow-up, the patient was hemodynamically stable and had no further events of amaurosis fugax or new focal neurological deficit. Repeat CT angiography showed normal flow across the carotid artery with good patency of stent. The same line of management was continued and he was advised regular follow-up.
Cutting Balloon Angioplasty of the Right Internal Carotid Artery. A: Pre-angioplasty, B: Balloon Inflation, C: Post-angioplasty.
Right CCA Angiogram After Stenting.
Discussion
Radiotherapy (RT) is an important part in the management of malignancies of the head and neck. Large vessel injury is now known to be a major complication of radiation in such cases. A review of 99 studies by Plummer et al., 1 showed that RT for head and neck cancer doubled the risk of TIA and ischemic stroke. These studies demonstrate an increased prevalence of carotid stenosis, which may be hemodynamically significant, in such cases. This is illustrated by an increase in the carotid intima-media thickness (IMT). Huang et al. 2 studied the IMT, which showcased the severity of atherosclerotic disease in extracranial vasculature. and increased in a linear way, with duration of RT. The pathophysiologic mechanism of the disease is related to radiation, 3 that directly injures the highly sensitive endothelial cells leading to apoptosis and senescence which leads to a systemic chronic inflammatory state that causes atherosclerosis. There is an increased tendency for thrombus formation, especially in the CCA and proximal segments of the ICA and ECA. Large vessel injury caused by RT can also manifest with unusual complications such as formation of an internal carotid artery pseudoaneurysm. Nazari P et al., 4 reports such a case of ICA pseudoaneurysm which presented with massive epistaxis.
The usual manifestations of extracranial carotid stenosis are paresis, sensory disturbances, aphasia, and dysarthria; whereas amaurosis fugax, dizziness, diplopia, amnesia, cognitive decline and headache are relatively uncommon. 5 Carotid bruit may be heard on auscultation. The time from onset of RT to the onset of symptomatic disease may take months to years. It may be related to the diameter of the irradiated arteries.
Carotid stenosis is diagnosed mainly by non-invasive imaging approaches like Doppler ultrasonography, which also measures IMT, a predictor of future strokes. 2 Other techniques, like ultrasonographic 2D-strain imaging, calculate arterial stiffness, while contrast ultrasound imaging is used to detect early atherosclerotic vascular changes. Magnetic resonance imaging and CT angiography are commonly used but digital subtraction angiography is the gold standard for carotid arterial stenosis. On angiography, carotid stenoses post-radiation were significantly longer than those caused by atherosclerosis and the area of maximum stenosis was usually at the end of the stenosis. 6
The two major treatment procedures for carotid artery stenosis include Carotid Artery Stenting (CAS) and Carotid Endarterectomy (CEA). Patients who underwent CEA had greater incidence of cranial nerve injury (CNI). It is also technically challenging, as vessel wall consists of adhesion of different layers. This complicates the excision of the plaque. 7 Presently, CAS has been increasingly used in patients after RT as the main advantage is that there are no CNI or wound complications. 8 Due to extensive disease, there is a larger surface area which has potential to embolize which may require angioplasty of longer segments and placing of multiple stents. Although this may lead to intimal hyperplasia and recurrence, most in-stent restenosis are asymptomatic. In such cases, cutting balloon angioplasty can be used for in-stent stenosis and fibrosis. 9 With the availability of new stents, delivery techniques, and distal protection devices, CAS has become a safe and effective option for radiation-induced carotid stenosis.8, 10 Although debatable, antiplatelet agents and statins can be used for secondary prevention. Few studies 11 have shown that vascular events decreased significantly with antiplatelets and statins in patients who underwent CAS.
Thus, this case highlights that amaurosis fugax can be a presentation of a patient presenting with carotid artery stenosis which has developed after RT and such patients can be safely managed by carotid angioplasty and stenting.
Author Contributions
Shashank Nagendra: Substantial contributions to conception and design. Avinash Gutte: Acquisition of data, analysis and interpretation of data. Abhijit Gaikwad: Drafting the article and revising it critically for important intellectual content.
Footnotes
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics Consent
Not applicable.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Not applicable.