
Abstract
Background
Chronic subdural haematoma (CSDH) is a common neurosurgical disease, particularly among the elderly, especially those on antiplatelet or anticoagulation with trivial trauma. While anticoagulants/antiplatelets increase the chance of rebleeding in cases of CSDH, discontinuation may increase the risk of stroke in these patients.
Case Description
We report two cases of CSDH in elderly patients with risk factors who suffered from an ischaemic stroke after undergoing surgery. The first case was an elderly gentleman who had a history of percutaneous coronary intervention, presenting with a CSDH. He developed an anterior cerebral artery infarct in the immediate postoperative period. The second was an elderly gentleman with a history of hypertension presenting with a concomitant left thalamic infarct and large left-sided CSDH. He developed a second middle cerebral artery infarct of the opposite side in the immediate postoperative period.
Conclusion
The medications used for stroke prophylaxis, that is, antiplatelets and anticoagulants are predisposing factors for the development of CSDH. However, the perioperative period of these patients remains vulnerable to the development of new-onset ischaemic stroke.
Introduction
Chronic subdural haematoma (CSDH) is one of the most common neurosurgical disorders, particularly in aged patients. The incidence of CSDH has been reported to be between 1.72 and 20.6 per 100,000 persons per year. 1 Risk factors include advanced age and use of antiplatelet/anticoagulant drugs. According to He et al., individuals taking aspirin experienced a rise of 12 events per 10,000 individuals in the risk of haemorrhagic stroke. 2 The risk of haemorrhagic stroke is significantly amplified by anticoagulation, with an increase of 7−10 times, resulting in an absolute rate of 1% per year. 3 Risk of perioperative stroke after neurosurgery depends on the type and indication of surgery. The incidence of stroke is 1.7% after surgery for intracranial tumours whereas it can be up to 11.8% in neurovascular surgery for aneurysm clipping.4, 5 However, ischaemic stroke after the evacuation of CSDH is a rare complication. Murthy et al. have found that the risk of arterial ischaemic events is significantly increased within 4 weeks after a diagnosis of non-traumatic SDH. 6 They further found that among arterial ischaemic events, the risk of ischaemic stroke is significantly increased following a diagnosis of non-traumatic SDH but not the risk of acute myocardial infarction. Hamou et al. reported 10 cases of stroke in 395 patients of CSDH. 7 Herein we report the findings of two patients who suffered from an ischaemic stroke after evacuation of chronic SDH.
Case 1
A 75-year-old gentleman presented to the emergency department of our hospital with a history of progressive weakness of the right upper and lower limbs along with altered sensorium for one week without any definite history of significant trauma. He had a history of undergoing percutaneous coronary angioplasty and was on clopidogrel. He also had hypothyroidism and hypertension for which he was on regular medication. On examination, he had right hemiparesis and was disoriented. Non-contrast computed tomography (NCCT) scan of the head at the time of admission showed the presence of a left-sided CSDH with a significant midline shift (Figure 1A). Clopidogrel was withheld and he was taken up for burrhole and evacuation of CSDH. In the morning of postoperative day one, he had regained full sensorium and was following commands with the improvement of his hemiparesis. A post-operative NCCT scan of the head showed evacuation of haematoma (Figure 1B). However, later on, the same day, he had a drop in sensorium and required intubation. A repeat NCCT scan of the head did not show any significant change. MRI of the brain was done which showed an infarct in the left anterior cerebral artery territory (Figure 1C). His sensorium improved gradually, and he was weaned off from ventilator support but he developed akinetic mutism. Echocardiogram, ECG and Doppler scan of the carotid arteries did not show any significant abnormality. He was started on aspirin and clopidogrel along with atomoxetine for akinetic mutism and was discharged to home and advised to follow up for further workup.
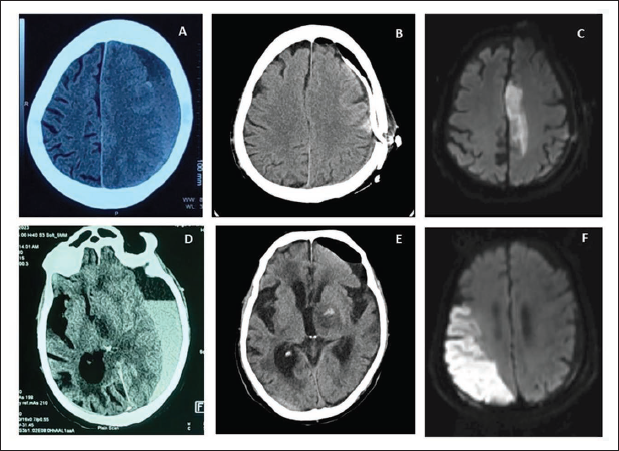
(A) Non-contrast CT Scan of the First Case Showing Left-sided CSDH with Midline Shift. (B) Post-operative Non-contrast CT Scan Showing the Evacuation of the Haematoma with Subdural Drain in situ. (C) DWI Sequence Showing Diffusion Restriction in Left Anterior Cerebral Artery Territory Suggestive of an Infarct. (D) Non-contrast CT Scan of the Second Case Showed Left-sided CSDH with a Hypodense Area in the Left Thalamus. (E) Post-operative Non-contrast CT Scan Showing Evacuation of Haematoma with Haemorrhagic Transformation of the Thalamic Infarct. (F) DWI Sequence Showing Diffusion Restriction Along the Inferior Division of the Right Middle Cerebral Artery Suggestive of Infarct.
Case 2
An 84-year-old gentleman presented with a history of right-sided weakness and altered sensorium for 3 days. He was intubated in the emergency due to poor sensorium. On examination, his Glasgow Coma Score (GCS) was E1VTM4 with right hemiplegia. He was hypertensive, on medication, and did not have any other comorbidities. His NCCT scan of the head on admission showed a left-sided chronic SDH with a significant midline shift. There was also a hypodense area in the left thalamus suggestive of an infarct (Figure 1D). He underwent burrhole and evacuation from CSDH. However, post-surgery he had difficulty in weaning off from the ventilator. Post-operative CT scan showed evacuation of the CSDH and a decrease in mass effect. A repeat CT scan of the head done on postoperative day 4 showed a haemorrhagic transformation of the thalamic infarct (Figure 1E). However, on postoperative day 9, his GCS dropped further and his GCS became E1VTM3. An MRI of the brain was done which showed a new infarct involving the inferior division of the right middle cerebral artery territory (Figure 1F). Echocardiography, ECG, and carotid Doppler did not show any significant abnormality. He was started on aspirin and was gradually weaned off from the ventilator. His GCS slowly improved to E2VTM4 and was discharged to home care with advice to follow up for further workup.
Discussion
About 45% of patients presenting with CSDH have a history of some form of anticoagulant or antiplatelet use. 8 The use of these medications increases both the incidence of CSDH and the risk of recurrence after evacuation of CSDH.9, 10 Hence, it is common to reverse the effects of these drugs or to delay the surgery, if possible, until the drugs have been cleared. Common strategies to achieve this include the use of platelet transfusion, delayed surgery in non-urgent cases, use of clotting factors or Vitamin K. 8 However, these measures come with a trade-off of increasing the risk of ischaemic events.
Murthy et al. have reported that the risk of an ischaemic stroke increases significantly after the diagnosis of nontraumatic SDH. They found the hazard ratio of an ischaemic stroke to be 4.2 (95% CI 2.1−7.3) after a diagnosis of non-traumatic SDH. 6 They also found that patients who had a previous history of valvular heart disease or atrial fibrillation or were on antiplatelet/anticoagulant drugs had a significantly increased risk of arterial ischaemic events. Hamou et al. reported an incidence of 10 cases of stroke in 395 cases of CSDH in their series. 7 In their literature review, they further found that the risk of thrombotic complications was significantly increased in patients on anticoagulants however, there was no increase in the thrombotic complication risk in patients on aminosalicylic acid.
Multiple mechanisms have been proposed to explain the cause of ischaemic stroke after subdural haematoma. The commonly suggested mechanism is decreased cerebral blood flow and subsequent cerebral ischaemia due to cerebral oedema. 11 Post-evacuation seizures resulting in cerebral ischaemia have also been proposed as a putative mechanism. 12 Use of antithrombotics/antiplatelets and previous history of valvular heart disease and atrial fibrillation have also been reported to be associated with the risk of stroke after CSDH.7, 6 The diagnosis of a stroke can be made rapidly using an MRI which shows diffusion restriction in the affected arterial territories. Alkhachroum et al. reported the use of transcranial Doppler to determine the arterial flow velocities of intracranial arteries. 13 They found the mean flow velocity to be lower and the pulsatility index to be higher in the affected site than on the normal side suggesting hypoperfusion and increased distal vascular resistance.
In the present cases, we believe that withholding the antiplatelet in the peri-operative period may have precipitated the ischaemic stroke in the first patient. For the second patient, we presume that the underlying mechanism was atherosclerosis, considering his age and history of hypertension. However, we couldn’t perform a diagnostic cerebral angiography to confirm the hypothesis at the present admission.
Previous use of anticoagulants has been shown to increase the risk of recurrence of CSDH by 18.8% and 32.1% in previous studies.14, 15 However ceasing antiplatelet therapy escalates the risk of ischaemic stroke or transient ischaemic attacks by 40%. 16 No definite guidelines are available for restarting anticoagulants or antiplatelets after surgery for CSDH and must be decided on a case-by-case basis. Chari et al. have suggested a comparative analysis between the CHA2DS2-VASc thromboembolism risk score and the HAS-BLED bleeding risk score in atrial fibrillation patients with CSDH to determine the suitability of resuming anticoagulants. 17 The RESTART trial examined the effect of starting antiplatelet therapy after intracerebral haemorrhage and didn’t find any significant difference in the risk of rehaemorrhage after starting antiplatelet therapy. 18 Naylor et al. in their cohort of patients didn’t find any increased rate of unplanned haematoma evacuation in patients with traumatic subdural haemorrhage who needed antiplatelet/anticoagulant therapy. 19 Zanaty et al. have performed a machine learning analysis and found that restarting antithrombotics after 2 days and within 21 days of surgery is associated with the lowest recurrence of bleed and low stroke rate in patients of CSDH. 20
Conclusion
Ischaemic stroke after CSDH is a rare complication but causes significant comorbidity if it occurs and delays the recovery of the patient. The risk factors that predispose the patients of CSDH to ischaemic strokes should be evaluated and decisions should be taken about starting anticoagulants or antiplatelets on a case-by-case basis to obtain an optimum outcome.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval from an institutional review is not applicable as the present report is a retrospective description of two cases and no prospective or retrospective research was carried out. Consent for publication was obtained.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Written informed consent was obtained to publish the clinical details of the patients.