
Abstract
The Mothers Delivery Kit discusses an innovative healthcare package sold in the poor West African region to aid with the delivery of expectant mothers. The package combines various necessary items used for proper and hygienic delivery of the rural and remote mothers with the help of a local midwife or medical practitioner. Antenatal care in the region is poor due to lack of infrastructure and government funding in healthcare. The Mothers Delivery Kit addresses that issue by providing a cheap and hygienic alternative to conventional delivery methods. The kit has decreased newborn death in the region noticeably. The founders have worked closely with local midwives to train them and enable them to use the Mothers Delivery Kit properly to improve delivery conditions. Regardless of the setbacks caused by local traditional beliefs and culture, the kit has proven to be an active effort to improve delivery conditions.
Introduction
The healthcare in sub-Saharan Africa (SSA) looks very bad because they find it tough to get basic healthcare. According to the World Health Organization (WHO), USD 34–40 is the minimum amount per year that could be spent on healthcare, which is not provided by the governments. Even after going through extreme poverty, 50 per cent of the country’s health expenses are financed by the individuals’ own savings. Donor attention has yielded remarkable efforts to fight HIV/AIDS, tuberculosis and malaria. But most of the region lacks the infrastructure to deliver healthcare and faces a severe shortage of trained medical personnel. As Africa’s economies improve, the demand for good quality healthcare will only increase further.
The effect of antenatal care (ANC) on women’s decision to seek skilled birth attendance (SBA) has received less attention by researchers than its impact on maternal and child health outcomes (Jewell & Rous, 2009). Three pathways may explain the relationship between ANC and SBA: through the quality of services provided and the information given to women (Nikiema et al., 2009); by increasing their familiarity with medical personal and thus reducing the ‘psychological costs’ related to seeking their services (Barber, 2006); and by creating or reinforcing habits to make use of this care. There are several reasons to believe that the decisions to seek ANC and qualified help at delivery (or to give birth in a health centre) are interrelated. First, various characteristics of women or their households, such as schooling attainment or income, can explain why women may opt for both types of care.
Concern over possible health problems may also affect both the demand for ANC and the likelihood of an SBA, acting to bias the estimated impact of ANC on SBA in single-equation models (Jewell & Rous, 2009). Thus, women experiencing complications or worried about health problems may seek both ANC and SBA more frequently than other women. However, expecting complications may, at times, have the opposite effect—deterring women from seeking formal care at delivery through fear of a caesarean section (Carter, 2010) or to avoid the direct and indirect costs of interrupting their normal activities. Thus, the direction of the bias cannot be known in advance as it will depend on the dominant effect.
In this case study, the authors intended to use different types of secondary documents (Ahmed, 2010), namely, Mothers Delivery Kit archival report, media reports, websites, mortality reports, and WHO and UNICEF reports. A purposive sampling method is applied as authors have only approached organizations where they have access to collect relevant data for the purpose of study (Yin, 2013).
The rest of this case study is developed by discussing ANC in Africa and factors affecting newborn deaths. Then, the case of Mothers Delivery Kit is discussed, including its inception, delivering hope to mothers, teaching birthing skills and helping to improved service utility. The subsequent section presents the setbacks and challenges, followed by the impact of COVID-19, ANC, policymaking and intervention.
Antenatal Care in Africa
The ANC/SBA association may also be partly explained by the existence of contextual factors that affect both phenomena simultaneously. This is the case when certain socio-cultural norms discourage women from using maternity services of any kind—ANC or SBA at birth. Women may make antenatal visits to verify how their pregnancy is progressing and, once reassured, they may not necessarily seek skilled help for the birth itself (Amooti-Kaguna & Nuwaha, 2000). A variety of reasons may underlie these decisions, and the researcher is not always aware of them. Some women may be seeking a kind of assurance vis-à-vis their community so as to avoid personal blame should their pregnancy end badly (Carter, 2010). In communities that prize childbirth without medical assistance, women may use these services to make sure that the pregnancy is progressing without complications. In addition, antenatal visits can be planned ahead of time (for example, coinciding with a trip to a local market)—something that is more difficult to do for childbirth. Whereas ANC can be given in any circumstance and at any time, delivery may begin unexpectedly and distance from healthcare services may prevent women from seeking trained assistance, even when they want and can afford it. Policies targeting the demand for services alone may not suffice and guarantee the desired decline in maternal and infant mortality (de Bernis et al., 2003). Improvements in maternal and child health in recent years could be attributed in large part to the improvement of the supply of care in the four countries studied and to the changes in the health policies with a greater decentralization in services in many countries since 2004. Ensuring a safe mechanism for the remote African region where resource shortage is a major reason for lacking healthcare especially for antenatal healthcare issues is a rigorous challenge.
Over 86 per cent of pregnant women take assistance of ANC with skilled health personnel at least once. However, among them, only 62 per cent receive at least four antenatal visits. Moreover, even fewer women received four antenatal visits in continents with the highest rates of maternal mortality, such as SSA and South Asia (52 per cent and 46 per cent, respectively) (UNICEF, 2016). It is important for pregnant women to visit the doctors regularly as it allows them to have a regular check-up of their health and that of their future children. It is recommended by the WHO for pregnant women to at least go to four ANC visits.
Factors Affecting Newborn Deaths
Maternal mortality is an acute problem for many countries in Africa, particularly those at the bottom of the pyramid (BoP) (Ahmed et al., 2020). The risk of dying as a new-born varies enormously depending on where a baby is born. The number of deaths per country is determined by the number of births and the risk of newborn death. Liberia has the highest risk of newborn death, with 6.6 per cent of babies dying in the first month of life. Many countries with the highest risk of newborn death have experienced war or diseases. Countries with large populations tend to have more births and are likely to have large number of newborn deaths. Poverty and the ill health and deaths of new-borns are intimately connected. The newborn health gap between rich and poor countries is unacceptably high, ranging from an NMR of 9 in Seychelles (GNI of USD 8,090) to 66 in Liberia (GNI of USD 110).
Newborn survival is closely linked to a country’s income level. High-income countries have an average newborn mortality rate of just 3. In comparison, low-income countries have a newborn mortality rate of 27. This gap is noteworthy. Rwanda, a low-income country, has more than halved its newborn mortality rate in recent decades, dropping it from 41 in 1990 to 17 in 2016. This exemplifies that the existence of political will to endow in strong health systems that prioritize new-borns and arrive at the poorest and most marginalized is serious and can make a major difference, even where resources are controlled.
Moreover, babies born to mothers with no education face almost twice the risk of dying during the newborn period than babies born to mothers with at least a secondary education. Babies born to the poorest families are more than 40 per cent more likely to die during the newborn period than those born to the least poor (UNICEF, 2014). They are dying because their families are too poor or marginalized to access the care they need. The good news is that progress is possible, even where resources are inadequate. Hence, it is quite a challenge to come up with an innovative solution at a reasonable cost that can address the issue and improve the lives.
Case: Mothers Delivery Kit
Background
Brown Button Foundation, a Lagos-based social enterprise, was founded in 2011 and focuses on training traditional birth attendants (TBAs) and community health extension workers (CHEWs) as well as nurses and midwives across rural communities in Nigeria. With a vision to bring maternal and child mortality in Nigeria to its lowest ebb, they work to sensitize pregnant women on health-seeking behaviours and nutrition in pregnancy, advocate immunization, especially for children under the age of two years, and provide family planning or child spacing options for women in rural communities. Its Mothers Delivery Kit was launched in 2013. The patrons of the Mothers Delivery Kit run have been actively working to provide women with the needful reproductive health services, increased access to healthy living and medical support, and further reduce the social stigma on women making independent and educated choices.
Inception
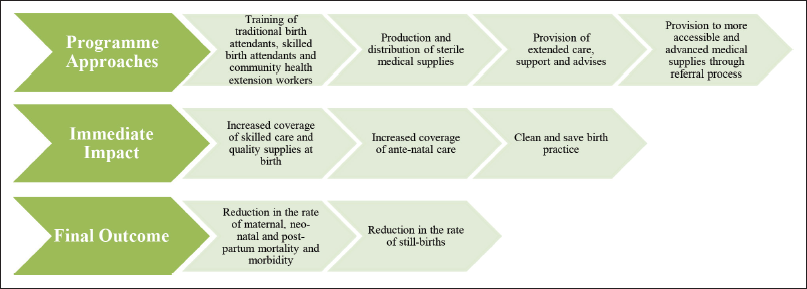
The inception of Mothers Delivery Kit has a rather tragic cause. Adepeju Jaiyeoba, a lawyer by profession and the founder of this social enterprise, was shaken by the loss of her dear friend to childbirth in 2011. Her friend belonged to an educated and financially solvent background. It befuddled her that the grim statistics of maternal mortality was not only limited to the less privileged but was also rather more outspread and alarming. She was quick to identify that the lifetime risk of 1 in 22 for women in Nigeria dying during pregnancy, childbirth and postpartum is a threat to the greater community (Ope, 2020). Hence, upon consultation with some of her well-wishers, she founded the Brown Button Foundation. Through their foundation and launch of Mothers Delivery Kit, they have been successful in making significant, all-embracing and positive changes in the maternal and child health and safety. Figure 1 aims to simply illustrate their impact in Nigeria.
Service Delivery Through Social Enterprising
This initiative stemmed as a need for urgent intervention into protecting the health of mothers and children. It aims to provide affordable, clean and safe delivery kit and to distribute across the rural zones of Nigeria to promote safe births. Even when services are available, people may not know how to access them. The 4A’s model of service delivery (affordability, availability, acceptability and awareness) provides a useful way of thinking about the issues involved (Ahmed et al., 2019). This initiative further advocates for women empowerment and for instigating a structural behavioural change in reproductive rights and choices. Their impact in the lives of the women and children in Africa goes beyond time and technology. Despite all the developments across the word, African women and children have always been negatively affected at a disproportionately higher rate due to systematic marginalization and gender bias.
Delivering Hope to Mothers
This social enterprise advocating and protecting the health of mothers and children is a major success across in Nigeria and highly lauded all around the globe. It was only made possible for its changemaker, which is a clean and safe USD 5 delivery kit that is manufactured and distributed by this enterprise. The usual kit contains a bundle of cotton wool, one anti-septic soap bar, delivery mat, methylated spirit, two pairs of sterile gloves, two chord clamps, mucus extractor, scalpel blades, gauze, disinfectant, maternity pads, infant receiver and olive oil. Olive oil is a cultural addition to this kit to cater and personalize the cultural beliefs in Nigeria. The locals have a strongly held spiritual belief of rubbing olive oil on the stomach of the mother and on the child to ease pain and for good health. Hence, Mothers Delivery Kit was quick to adapt to it. Furthermore, there is the availability of another kit termed as the ‘value added kit’ which is more customized by the addition of the drug Misoprostol. Tracing back to the direct causes of maternal and child morality, much of it is caused due to infection, haemorrhage and sepsis. This one-time usable kit has an immediate and direct impact on mitigating infection and sepsis by promoting a safe, hygienic and clean delivery process conducted by trained health professionals. The use of clean gloves, clean and one-time useable delivery mat, and sterile implements to cut placenta have been shown to reduce infection by more than half. Furthermore, research suggests that Misoprostol (worth around USD 3) is highly effective in preventing postpartum haemorrhage, which is a significant direct contributor of maternal death. Figure 2 shows a picture of the Mothers Delivery Kit packet.

Teaching Birthing Skills
From its inception, Mothers Delivery Kit has rigorously worked towards its vision to eradicate maternal and infant mortality through improved healthcare access. It has reached over 1 million mothers and children and has trained over 8,000 TBAs, mid-wives and CHEWs in Nigeria. They have successfully tapped into 186 local communities and 30 out of 36 cities, deployed over 512,000 kits, and conducted over 300 trainings and workshops for health and medical professionals in Nigeria.
Mothers Delivery Kit has proactively targeted as many cities, localities and communities to conduct trainings and workshops for TBAs and Skilled Birth Attendant(s) (SBA). They have further introduced several advocacy sessions in all those communities to spread awareness on service development and availabilities. These trainings and workshops aim to equip the birth attendants with the modern methods using the available kit. It boosted the confidence of the birth attendants and improved their service delivery. Increased trainings and workshops have naturally created a tier-based process for delivery in the communities of Nigeria. TBAs are well- equipped and proficient in the following:
Handling primary ante-natal care, Inducing medication by the blood loss limit, Recognizing complications, Setting up a linkage with referral hospitals, healthcare centres or SBAs, Conducting natural deliveries for safe birth.
The ultimate achievement of these trainings has been the success of the referral process. The TBAs are taught to understand the level of severity or complication of the expecting mothers. Hence upon identification of complicated or sensitive cases, the TBA carries out primary procedures to contain the severity and quickly communicate with an SBA in one of the referral hospital or healthcare centres. The increased engagement of the facility providers with the referral centres has boosted the trust of both the parties as well as of the expecting mothers and their families.
Helping to Improved Service Utility
The increase in the number of TBAs and SBA have shown slow yet convincing results. Within a few years of the launch of this programme, delivery by SBAs doubled to 23.9 per cent. Furthermore, the rate of women seeking ANC has also shown a sharp increase to 48.8 per cent by 2015. The rate of maternal mortality in Nigeria has dropped from 1,200 (per 100k live births) in 2000 to 972 in 2011 and to 917 in 2017. The declining trend is a strong indication of positive reception of modern methods and new initiative as well as a change in traditional beliefs. The linkages are expanding and allowing necessary equipment or network with blood banks to be more accessible. One of the key initiatives taken by Mothers Delivery Kit was building a digital bridge between private facility providers to public hospitals and blood banks by collaborating with a new start-up, Life Bank. Life Bank uses advance technology, big data, smart logistics and artificial intelligence to gather information and trace the needs of medical supplies, blood and others. By tracing these needs at particular locations, they connect them with the nearest facility provider or healthcare centre with an existing inventory of those supplies. It generates data from more than 40 blood banks and over 300 hospitals and healthcare centres in their marketplace app. They further use their own delivery system (each ride costing around USD 8) to collect and distribute the supplies (Rotinwa, 2021). In the past nine years, the organization has come a long way. It evolved from a small-scale initiative for assisting mothers in a poor West African region to an organization which received ample international media attention and significantly scaled up its operation. As of 2021, 186 communities are reached, 347 dedicated training and workshops have been arranged, and beyond half a million kits have been deployed.
Setbacks and Challenges
Amidst all the success and encouraging numbers seen by this initiative, the challenges are yet to concealed or eliminated. Adepeju Jaiyeoba and her team have been persistent with their efforts to turn the challenges into their benefits. This has been seen through them embracing some cultural beliefs, channelling in political network and building a lobby of powerful individuals to boost the presence and the activities of Mothers Delivery Kit.
Initially, the challenges were seen to be coming from the conservative nature of the households in Nigeria. Women must seek approval from their male family members to avail any services in the healthcare facilities. Nigerians have a centuries-old tradition in home births and in spiritual and herbal remedies for comfort and ease of pain. However, this setback was successfully managed by having greater reach to target audience, creating more awareness of maternal healthcare and services to women and their family, and through provisions of affordable medical equipment and trained healthcare professionals. The Mothers Delivery Kit initiative, through their parent organization Brown Button Foundation, have ensured and promised a systemic development in the following:
Efficient service of healthcare workers, TBAs and CHEWs through a series of trainings and workshops. Timely and consistent distribution of sterile maternal kits at affordable pricing. Provision of excellent support through easily available services, advises and support to the women and their family regarding maternal and reproductive health. Provision of increased and constant support to healthcare facilities by necessary equipment, extended external support (i.e., getting emergency blood) and required renovations.
Finally, challenges were further imposed by conflicting political interests of different agencies, political parties and government authorities. These challenges were imposed either by restriction of progressing into their initiative or by demanding ownership or financial benefits. Adepeju Jaiyeoba have smartly channeled through these challenges by constant engagements of stakeholders at all levels to accumulate public demand and support. Further, the foundation exercised its network primarily through related contacts and snowballing into expanding the network into lobbies of powerful individuals in government, politics, media and various other capacities. They have further garnered sufficient international support. They have been receiving funds from various US-based development programmes. Furthermore, Adepeju Jaiyeoba received the Mandela Washington Fellow in 2014 and a special invite in the White House during President Barack Obama’s period as a successful changemaker.
Impact of COVID-19
Historically, pandemics and epidemics have heavily disadvantaged the poorer nations. COVID-19 brought the entire world to a standstill. While every nation struggled to revamp their economy after a series of lockdowns, slow economy, and reduced production and services, a greater portion of Africa, Asia and South America are having to bear the damage even now and are expected to continue for longer. Inequality of vaccine distribution, inefficient policies and misinformation are some of the major reasons of this prolonged economic struggle. COVID-19 has far-ranging impact on the privilege, health and lifestyle of women and children in Africa. Figure 3 illustrates on the impact in Africa due to COVID-19.
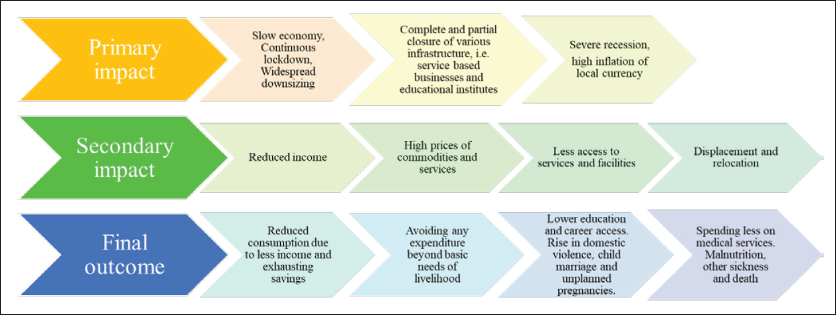
The illustration in Figure 3 draws a grim picture of the current situation in Africa as a result of COVID-19. Although significant formal jobs have been protected, most of the informal jobs in Africa saw massive downsizing. Service-based, part-time and other forms of informal jobs accumulates the greater majority of income sources in Africa. As this sector received major damage, the population in general is facing reduced income; exhausted savings; lower consumption of food; shrinking expenditure on products, services and healthcare facilities; and rising social inequity (UNICEF, 2020). More women are having to compromise on their jobs and some others on their education. There has been a significant rise of assault, rape and abduction of women since the beginning of COVID-19. Due to less income and safety concerns, families are marrying off their young daughters to reduce the cost and risk of the dependents, whereas families of the prospective grooms are encouraging further marriages in expectation of receiving dowry to support their livelihood. During the first half of 2020, around 4,000 Kenyan school children were subject to child marriage. This has led to a drastic spike in unplanned and early pregnancies. Many of these girls are either unaware, prevented from or afraid of the use of contraception and abortion services (African Child Policy Forum [ACPF], 2020). Ongoing school closure has further triggered the number of child marriage and unplanned pregnancies. Data suggests that until 2020, around 450 million modern African households were using contraception. However, the number is expected to drop drastically by 47 million or more if the lockdowns continue and if the economy fails to pace up the growth soon (ACPF, 2020). The consequences of COVID-19 have put Africa almost 20 years behind from all the progress and developments it had made for the economy, health and safety of its citizens, and in empowering and ensuring the rights of its women and children.
Antenatal Care: Policymaking and Intervention
To eradicate maternal mortality, it must seek for a strategy that stems from the government and other concerning authority. This strategy will support the availability of facilities, finances and effective policymaking which ultimately improves infrastructure, awareness, communication and overall health standards. Policymaking and intervention regarding maternal mortality needs to start from the grassroots, that is, policies regarding childbearing and support. The first policy initiative should be directed towards expanded literacy on sexual health and safe motherhood. Second, attempts to improve emergency obstetric care is inevitable to reduce direct causes of maternal mortality. Finally, initiatives are to be direct at a legal and government level to lift the ban on abortion and use of contraceptives, and by reducing the cost of health facilities and medication.
First, policies should be designed to make effective intervention through education and awareness. Such intervention can be made through acknowledging and accepting the ‘taboo’ concepts of the less developing societies, and educating on issues of safe sex and motherhood. In other words, there needs to be greater awareness and knowledge regarding conceiving, contraception and safe pregnancy. Hence, initial initiatives should be directed towards expanded literacy for both genders and of all ages regarding sex, safety and motherhood. Male-dominated social ideologies continue to suppress and marginalize women, leading to sexual violence and unwarranted pregnancies. Allowing women to plan pregnancies, that is, participating in family planning, leads to an average birth spacing of minimum two years and hence creates safer maternal health (United Nations Population Fund [UNFPA], 2013). Second, policies need to be directed towards creating effective clinical intervention. This policy emphasizes on the need of having increased access to skilled health attendants and adequate emergency obstetric care. Most direct maternal deaths are preventable if attended to by skilled health personnel- doctors, nurses or midwives, regularly supervised, properly equipped with medicines, lifesaving drugs and tools to offer emergency obstetric care and surgical interventions. According to an experimental project carried out by CARE in parts of Africa (Kayongo et al., 2006), effective clinical intervention can take the form of the following:
Equipping with indispensable tools and supplies required for surgeries and obstetric care, Structural developments of clinics and increasing the number of availabilities across different locations, Skill-based training to provide quality care, better supervision and quick referrals, Efficient record keeping and analysis, Review and development of policies and protocols, Aligned strategies to support services for ante-natal, natal and post-natal care.
Finally, effective policymaking at a legal and government level is required to address the grassroots issues of direct maternal mortality. Such issues stem from ban on abortion, limit on the purchase of contraceptives, unaffordable healthcare, and inadequate number of skilled health professionals and medical centres.
Footnotes
Declaration of Conflicting Interests
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support from InterResearch, Dhaka, Bangladesh.