
Abstract
Vaccines have taken the centre stage in the fight against COVID-19 pandemic, and in reducing hospitalisation and associated mortality. Countries around the world are heavily dependent on the successful rollout of their vaccination programmes to open up the societies and re-start their economies. However, the success of any vaccine programme, to a large extent, depends upon the efficacy and safety of the vaccines. Given that UK has been way ahead in vaccinating its population, is considered a successful model compared to other countries in Europe and elsewhere and has a yellow card reporting system for adverse events, we use UK as an example to understand the side effects and fatal outcomes following vaccinations. Our results show that AstraZeneca seems to be underperforming in terms of overall reporting of minor adverse events, serious incidents and fatal outcomes following vaccination. The risk of serious anaphylactic reaction and fatal outcome was 1.36 and 1.17 times more in case of AstraZeneca vaccine when compared with Pfizer BioNTech vaccine. The analysis has implications for vaccine policies and programmes both at nation-state and global levels.
Keywords
Introduction
There have been over 230 million cases and 4.7 million deaths due to COVID-19 worldwide (Worldometer, 2021). In the United States alone, there were 43.2 million cases with 696,869 deaths due to COVID-19 (Worldometer, 2021), making it the 3rd leading cause of death in the United States in 2020 (Ahmad et al., 2020). The UK has reported 7.4 million cases and 135,455 deaths as a result of COVID-19 since the start of the pandemic (see UK Coronavirus Dashboard; Worldometer [2021]).
Social distancing measures, testing and contact tracing, isolation and quarantine, wearing personnel protective equipment, washing hands and using disinfectants are still important measures in containing the spread of transmission of this virus. However, with accelerated development and emergency approval for its use, vaccines against COVID-19 have taken the centre stage in the prevention of this disease, and in reducing hospitalisation and associated mortality, and countries are heavily dependent on the successful rollout of their vaccination programmes to open up the societies and re-start their economies. On the one hand, the developed world has purchased and pre-ordered doses in bulk to cover its entire population, and, on the other, majority of the low-income countries are left out without any vaccines to protect their populations. Recently, some low-income countries, through the WHO’s COVAX programme (WHO, 2021) are being given access to the COVID-19 vaccines but inadequate to offer protection to their population.
The success of any vaccine programme to a large extent depends upon the efficacy and safety of the vaccines. The UK has led the way with respect to vaccine development, authorising regulatory approvals and the use of vaccines against COVID-19. It was the first country to approve and authorise the use of Pfizer BioNTech vaccine on 2 December 2020 (Pfizer, 2021) followed by Oxford–AstraZeneca vaccine on 30 December 2020. The first dose of Pfizer BioNTech vaccine was given in the UK on 8 December 2020.
Since regulatory approval for the vaccines, number of countries have used millions of doses to protect their populations from COVID-19. Such data further provides information on various adverse effects, serious incidents following vaccination, especially with respect to those rare and fatal events that may have been missed out in clinical trials because of a relatively small sample. Vaccine development goes through various phases of clinical trials and typically takes many years to develop. For example, it took about 40 years for Ebola vaccine to be licensed in the United States after linking of the disease to Ebola virus (Ball, 2020). However, under the accelerated vaccine development, it took less than a year to develop the COVID-19 vaccines, a remarkable achievement. However, concerns have also been expressed with respect to the accelerated development of these vaccines in terms of safety of these vaccines (Torreele, 2020).
With regards to the size of clinical trials, the AstraZeneca vaccine trial was based on 23,000 participants, whereas the Pfizer BioNTech trial had 43,000 participants. These trials were designed to estimate the efficacy of the vaccines and detect common side effects. In comparison to the trials, as of 28 March 2021, UK had given 19.5 million doses of AstraZeneca vaccine and 14.6 million doses of Pfizer BioNTech (Medicines and Healthcare Products Regulatory Agency [MHRA], 2021), which provides an opportunity to analyse the rare side effects and fatal outcomes following vaccination. Given that UK has been way ahead in vaccinating its population, is considered a successful model compared to other countries in Europe/the region and has a yellow card reporting system for adverse events following COVID-19 vaccinations, we use UK as an example to understand the side effects and fatal outcomes following COVID-19 vaccinations.
Adverse Events, Serious Incidents and Fatal Outcomes Following COVID-19 Vaccinations.
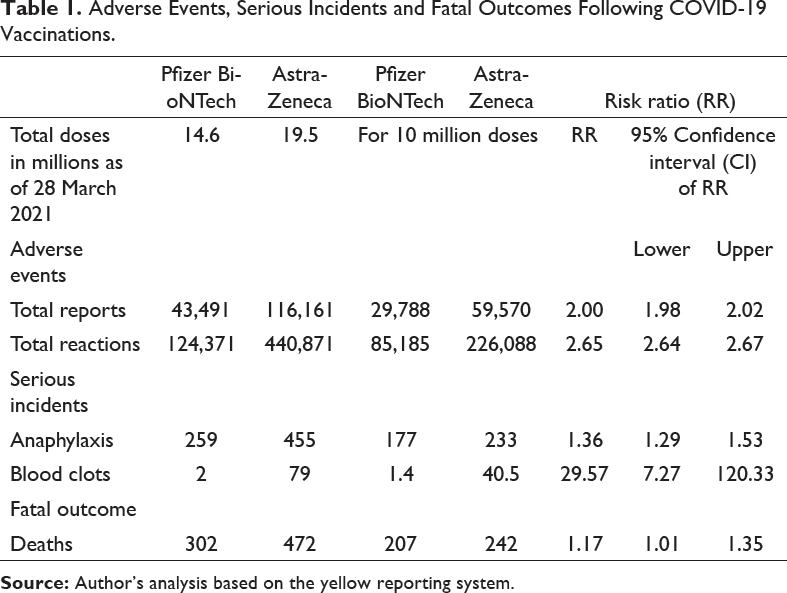
Results show that AstraZeneca seems to be underperforming in terms of overall reporting of minor adverse events, serious incidents and fatal outcomes following vaccination (Table 1). The reporting rate for Pfizer BioNTech was 2.98 per 10,000 doses whereas it was 5.96 per 10,000 doses in case of AstraZeneca. Persons vaccinated with AstraZeneca vaccine were two times more likely to report as compared to those vaccinated from Pfizer BioNTech. Similarly, total side effects reported were over 2.6 times in case of AstraZeneca as compared to Pfizer BioNTech. The risk of serious anaphylactic reaction was 1.36 (95% CI 1.29–1.53) times in case of AstraZeneca vaccine when compared with Pfizer BioNTech. Similarly, the risk of fatal outcome was 1.17 (95% CI 1.01–1.35) times that of Pfizer BioNTech.
In the United States, as per CDC, there were a total of 2,794 fatal outcomes following the vaccination of over 167 million doses were reported as of 5 April 2021 (CDC, 2021). This gives us a fatality rate of 167 per 10 million doses in the United States. In comparison, the UK fatality rate was 207 and 242 per 10 million doses for Pfizer BioNTech and AstraZeneca, respectively.
Results also show that the risk of fatal outcome with respect of vascular conditions, including blood clots and thrombolytic events, was around 30 times following AstraZeneca when compared with Pfizer BioNTech. The risk of blood clots following AstraZeneca vaccination is around 41 in 10 million doses whereas it is 1.4 in case of BioNTech. Not surprisingly, AstraZeneca was in news lately with respect to blood clots following vaccination. In March 2021, number of European countries had temporarily banned its use and re-started after reassurances from European Medicine Agency (EMA) and MHRA regulators that its benefits outweigh the risk of rare events like blood clots. Yet, number of countries have banned the use of AstraZeneca in younger age groups. For example, AstraZeneca is not being used for population below the age of 60 years in Germany and elsewhere. Given the announcement of 7 unfortunate deaths from the 79 cases of blood clots following the AstraZeneca vaccination in the UK on 3 April, the MHRA issued a statement in its press conference on 8 April, curtailing the use of AstraZeneca vaccine for those in the age group of 18–29 years. Since the announcement on 8 April, number of other countries including New Zealand and the Philippines too have restricted the use of AstraZeneca vaccine. It is understood that the African Union too was looking for alternatives to AstraZeneca and is considering 400 million doses of Johnson and Johnson as a replacement for AstraZeneca.
It is important that safety concerns of any vaccines are considered in the light of its efficacy. The efficacy rates reported from the clinical trials for AstraZeneca was 62% (Voysey et al., 2021) whereas it was 95% for Pfizer BioNTech vaccine (Polack et al., 2020). Thus, with lower efficacy rates on the one hand and higher risk of serious side effects and fatal outcomes, it appears that confidence in AstraZeneca vaccine both within the UK and globally is being eroded.
Caution is advised in interpreting and comparing the results based on a yellow card reporting system. Such systems are prone to reporting bias as anyone may choose to submit a report which may not be accurate as they are not verified. Even if the reports are accurate, and consistent in terms of quality, causal inference may not be justified as the reported adverse effects or fatal outcomes, as these could be incidental and not linked to the vaccines. In addition, absence of beneficiary characteristics, age differences, associated co-morbidities and so on make it difficult to establish any direct comparisons between the two vaccines. This is all the more relevant in the context of COVID-19 vaccination as the vaccinated groups are different. For example, selection bias in terms of the beneficiaries of these vaccines is a strong possibility, as Pfizer BioNTech was given much earlier in the UK to the elderly population with co-morbidities, those belonging to priority risk groups 1–5, whereas AstraZeneca was given to the population belonging to priority risk groups 6–9. It may also be noted that the analysis presented above is restricted to data analysed just prior to the MHRA announcement with respect to blood clot cases in the UK in the month of April 2021.
However, irrespective of the type of COVID-19 vaccine, recent data suggests that vaccines not only prevent infections but also reduce the severity of symptoms, hospitalisation and death. Majority of hospital deaths observed among COVID-19 patients are among the unvaccinated. According to the modelling by the Public Health England, as of June 2021, it is estimated that COVID-19 vaccines have prevented 7.2 million infections and 27,000 deaths in England alone (Public Health England, 2021a).
Concerns over its efficacy and safety record, and negative media coverage, specifically relating to blood clots, are diluting confidence in AstraZeneca vaccine and may result in reported in the recent report by Office for National Statistics (2021). The vaccine hesitancy was over two times among adults belonging to the Asians, Chinese or mixed ethnic backgrounds as compared to Whites and was over five times in case of Black adults. This is likely to be aggravated following the 7 deaths and 79 cases of blood clots reported after the study. It is therefore not surprising to note that although the UK medicines regulator has approved the use of Pfizer and AstraZeneca as COVID booster vaccines, the Joint Committee on Vaccination and Immunisation (JCVI) in its recent press conference on 14 September 2021 side-lined AstraZeneca vaccine and recommended that only the Pfizer and Moderna jabs, which use mRNA technology, should be used in any national booster programme (Public Health England, 2021b).
Awareness raising and confidence building measures along with transparency with respect to safety concerns might be needed to augment uptake of AstraZeneca vaccine among the Black and Minority Ethnic (BAME) group within the UK. Where alternatives are available, policymakers may wish to consider, offering its population the choice of vaccines, where appropriate, to boost vaccine uptake and minimise vaccine hesitancy among its population. These findings also have serious implications for low- and middle-income countries, whose demographic profile includes large percentage of young population who may be at a higher risk of blood clots. In fact, unlike the developed world, who have the resources to consider alternate vaccines for their national programmes, many of the low-income countries may have little choice in terms of affordability. They are heavily reliant on the WHO’s COVAX programme, which to a large extent, is dependent on the AstraZeneca as it has committed millions of doses to this programme.
More transparency is needed in decision-making and sharing information including the data from the investigation of the 70 blood clot cases and the deaths reported in the UK. All subsequent serious adverse events and fatal outcomes for each vaccine are timely reported in a full and transparent manner. Along with the yellow reporting system, the data on beneficiaries should be made available in the public domain by individual vaccines. Further research needs to be undertaken with respect to comorbidities, age and sex distributions, and risk profile verses adverse events so that one can minimise the risk of serious and fatal outcomes from the vaccines. Other low- and middle-income countries can learn from the UK experience of yellow reporting systems and implement similar robust monitoring systems. For example, India, given its population size and extensive use of AstraZeneca vaccine (Covishield), too should ensure that robust systems are in place to monitor adverse events and fatal outcomes as a result of vaccination and ensure transparency in making this data available. The awareness of such adverse events and its impact should be made available at local level so that the communities are able to take informed decisions. WHO’s lead in collating and monitoring such information is crucial and can provide early warning with respect to safety concerns both in terms of short- and long-term adverse effects of COVID-19 vaccines.
Contributory Statement
Mrigesh Bhatia planned this article and wrote the first draft. Venkata Putcha, D. P. Singh and Laxmi Kant Dwivedi provided statistical inputs. All authors have contributed to the writing of the final version of this article and have approved it.