
Abstract
Adopted children are likely to present with a wide range of common mental health issues requiring assessment and therapeutic support. In England the commissioning of therapeutic support is usually conducted by non-mental health professionals. The current study compares the mental health concerns raised in 153 consecutive referral letters from post-adoption social workers against the diagnoses subsequently identified by a specialist mental health clinic for adopted and fostered children. The social workers referred appropriate cases for specialist assessment, with an average of just over two psychiatric diagnoses per child identified in clinic, but there was low agreement between the mental health issues raised in the referral letters and the corresponding clinic diagnoses, particularly in relation to attachment and trauma issues. Most common amongst a wide range of conditions identified (N = 16) in the clinic were behavioural problems (66.0%), ADHD (61.4%), autism (26.1%) and anxiety diagnoses (23.5%). A minority of children received either post-traumatic stress (12.4%) or attachment-related (0.6%) diagnoses. Notably, when free to choose referral issues for further assessment, social workers also rarely identified issues with attachment (21.6%) or trauma (8.5%). Discussion considers the barriers to a shared understanding between social workers and clinicians regarding mental health issues in adopted children. These challenges are especially important in England where the study was conducted because contrary to the evidence base adoption support has since been restricted to address only issues of attachment and trauma, which were both minority issues in social workers’ referrals, rarely diagnosed and indicated little shared understanding between professionals.
Introduction
Post-adoption support takes many forms within and between countries, due to different conceptualizations of what post-adoption support means as well as the different adoption contexts in different countries (Drozd et al., 2017; Harris-Waller et al., 2018). For the UK context, knowing what kinds of mental health support would be most helpful for families is compromised by the absence of epidemiological evidence of the range of conditions typical of adopted children. However, the majority of children have been adopted from the UK’s domestic care system, and a high-quality epidemiological study of looked after children in the UK, conducted approximately 20 years ago, identified almost half with formal mental health conditions, primarily behavioural problems and ADHD, alongside elevated rates for all investigated conditions (Ford et al., 2007), consistent with a study of mental health conditions in adopted children in the US conducted during a similar period (Keyes et al., 2008). Similarly, international studies have confirmed the wide-ranging impact of early neglect and maltreatment on later mental health; for example, a large umbrella analysis based on over 11 million participants of the impact of child maltreatment on later outcomes revealed a small to modest effect distributed across all types of mental health conditions rather than for a subset of specific conditions (Coughlan et al., 2022). A pattern of elevated risks across a wide range of conditions has also been found for adoption samples in other countries (Behle & Pinquart, 2016).
Adoptive parents in the UK report significant and wide-ranging mental health issues for their adopted children, including behaviour problems, anxiety and peer relationships (Woolgar et al., 2024). Indeed, a recent survey of over 2000 adoptive parents revealed over a third (38%) were “facing severe challenges or reaching crisis point” and “three quarters reported a continual battle to get the help and support they need” (Adoption UK, 2024). The same report revealed over half (60%) of adopted parents had experienced violent or aggressive behaviour directed at them by their adopted children. Thus, there is likely to be a high level of mental health need, across a wide range of conditions for which families are seeking therapeutic support.
Within the UK a subset of adoptive families (i.e., those residing in England, but not those in Scotland, Wales or Northern Ireland) can apply to receive financial support “to pay for essential therapeutic services” for mental health needs from what was initially called the Adoption Support Fund (ASF; UK Government, 2017) and latterly the Adoption & Special Guardian Support Fund (ASGSF), to reflect the extension of the fund to some other families with permanency arrangements (UK Government, 2023). For simplicity, we will refer to the users of this fund as adoptive families and refer to the fund as the ASF due to that being the name of the fund during the period in question. The fund began in May 2015 and is predicted to have provided over £400million for assessment and therapeutic support in the following decade. Over the lifetime of the fund, and contrary to the available evidence, there has been an increasing narrowing of its remit to focus only on attachment and trauma at the expense of other mental health issues. Applications to the fund are made based on an initial assessment conducted by non-mental health professionals (post adoption social workers), which are evaluated and approved by a non-mental health external contractor (an engineering and infrastructure consultancy) and ultimately funded by an education department (the Department for Education in the UK, DfE). Therefore, neither mental health professionals nor mental health services have a direct role in the initial assessment of mental health needs nor the commissioning of therapeutic support for the families. From a research point of view, this offers the opportunity to explore how professionals from outside of the mental health sector make sense of adopted children’s mental health needs by comparing their assessments for therapeutic support with the findings of a specialist mental health clinic for adopted and fostered children.
The quality of mental health referrals from community services to specialist adoption and fostering mental health clinics has been previously explored in the UK and the US, by comparing the outcomes of formal assessments within specialist mental health clinics with the issues raised in the referral letters, revealing a consistent pattern of multiple mental health diagnoses being missed, and in particular an over-identification of issues to do with attachment (Allen & Schuengel, 2020; Woolgar & Baldock, 2015). There is additional evidence that practitioners have a tendency to bias their clinical explanations of care experienced children’s mental health needs with trauma-related explanations at the expense of identifying more common conditions (McGuire et al., 2022). However, potential biases towards attachment and trauma conceptualisations at the expense of other conditions have not been explored in the context of non-mental health professionals’ conceptualisation of adopted children’s problems.
In the current study we present a consecutive series of referrals from post-adoption social workers to a specialist mental health clinic for adopted children, at the beginning of a dedicated fund to commission mental health support for adopted children, but before a constraint was imposed to restrict the fund only to issues of attachment and trauma. We predicted that the descriptions of child mental health problems in the referrals for a clinical assessment would be characterised by an over-identification of attachment and trauma issues, and that this focus would mask more common mental health problems. We also predicted that children referred to the specialist clinic would have multiple mental health issues not previously identified, evident across a wide range of conditions. Finally, we explored the extent to which the issues highlighted in post-adoption social workers’ referrals mapped onto the final diagnoses, as an indicator of the extent to which a shared understanding exists between non-mental health and mental health professionals’ conceptualisations of adopted children’s therapeutic needs that is sufficient to guide the focus of specialist clinical assessments.
Method
Procedure
Each referral to the specialist clinic was accompanied by a letter in which a post-adoption social worker made the case for a multidisciplinary assessment based upon an initial assessment of the need for therapeutic support conducted within social care. Social workers also supplied previous reports that were available to them, including reports by local statutory mental health services (CAMHS). Thus, some children may have had mental health conditions previously diagnosed.
The specialist clinical assessment involved interviews and questionnaires with the parents; interviews, questionnaires and psychology assessments with the child, as appropriate; review of previous reports where available; and questionnaires and interviews from school, as indicated. The output of the assessment comprised a standardised structured report, that always included a section containing a biopsychosocial formulation (e.g., Pinto, 2019) and diagnoses based on ICD-10 categories (with the exception of reactive attachment disorder (RAD) and disinhibited social engagement disorder (DSED) which used DSM-5 criteria as these reflected significant research-driven changes in their conceptualisation since the creation of the ICD-10 codes).
A standardised coding sheet was used to extract data from the referral letters and clinical assessment reports. For the referral letters, a distinction was made between a pre-existing referral diagnosis, using either a recognised mental health term such as “conduct disorder” or some other specific reference to a ‘disorder’ even if this was not formal psychiatric terminology, versus a referral problem which described issues in non-diagnostic terms such as aggression, self-harm, sensory issues etc.
Formal diagnoses in both the referral letters and clinic were recorded under diagnostic clusters following the approach of O’Connor et al. (2020) who specified 10 clusters in CAMHS services. For the current study, there were no instances of the last four clusters (eating disorders; schizophrenia; personality disorders; and gender identity disorders). To ensure the key themes for this study of attachment and trauma were represented we a) split the ‘anxiety and stress related’ cluster into an anxiety cluster and a distinct PTSD cluster; and b) captured only the attachment disorders from the ‘disorders of social functioning’ cluster. This left seven diagnostic clusters (post-traumatic stress disorder (PTSD); RAD/DSED; oppositional defiant disorder/conduct disorder (ODD/CD); Anxiety diagnoses; Depression; ADHD; Autism). There were additionally several diagnostic neologisms in the referral letters also using the term ‘disorder’ (e.g., ‘trauma attachment disorder’), which were recorded in a free text box and are discussed separately.
Referral problems were mapped onto the seven categories corresponding to the diagnostic categories (Trauma-PTSD; Attachment-RAD/DSED; Behaviour problems-ODD/CD; Anxiety-Anxiety diagnoses cluster; Mood-Depression; Inattention/Overactivity-ADHD; Social Communication-Autism). Referral problems that did not fit into these categories were recorded in a free text box and grouped into six categories after data collection (Dysregulation; Risk; Cognition and Learning; Developmental Problems; Transitions; Social Problems; and Other). All referral letters and clinic reports were coded retrospectively by two clinicians in the team who were not involved in the original assessments and disagreements resolved by consensus.
Sample
The data comprised a consecutive series of case notes of 153 children and young people referred to the specialist clinic. The case notes were accessed as part of a service evaluation, approved by the institutional clinical governance committee.
The period under investigation includes referrals from the initiation of the Adoption Support Fund (ASF) in March 2015 until November 2019. Data beyond this point is not presented because the waiting times from referral to assessment meant that Covid restrictions had begun in the UK, with implications for the kinds of assessments that could be conducted by the clinic, in particular impeding the ability to do gold-standard, face-to-face assessments for neurodevelopmental conditions. Following the resumption of face-to-face assessments, the criteria for referrals approved by the ASF had been fully constrained to focus on issues of “attachment and trauma” only. This impeded the systematic investigation of all relevant aspects of mental health issues in the children and young people referred to the clinic, as well as restricting what issues the social workers were free to highlight in their referral letters and therefore referrals from this point onwards would be biased and were not used in the current report.
The sample was comprised of white British or white other (79.7%), dual heritage (13.1%), black British (4.6%), and Asian (2.6%) children (i.e., comprising 20.3% from racially minoritized groups, similar to the 19.0% and 16.3% recorded in recent UK adoption studies, Burch et al., 2023 and Woolgar et al., 2024, respectively). The sample was mostly boys (64.1% and 35.9% girls; no families reported non-binary children), with a mean age of 10.1 years (sd = 3.86, range 1 to 18), with 52.9% aged 10 or below and 47.1% aged 11 to 18.
Data analysis
Associations between referral problems and the clinic diagnoses with gender, age-group and ethnicity were made using chi-square. To assess the degree to which the terms used in the social workers’ referral letters, reflecting the outcomes of their initial assessments for therapeutic support, mapped onto the clinic diagnoses, percentage agreements and chance-corrected kappa statistics are presented. Finally, chi-square was used to test whether the general problems identified in the referral letters were more associated with some clinical diagnoses than others, i.e., were some general, but non-diagnostic problems guides to specific mental health issues.
Results
Referral problems
Mental health referral problems and clinic diagnostic categories by gender, age and ethnicity with chi-square tests (N = 153).
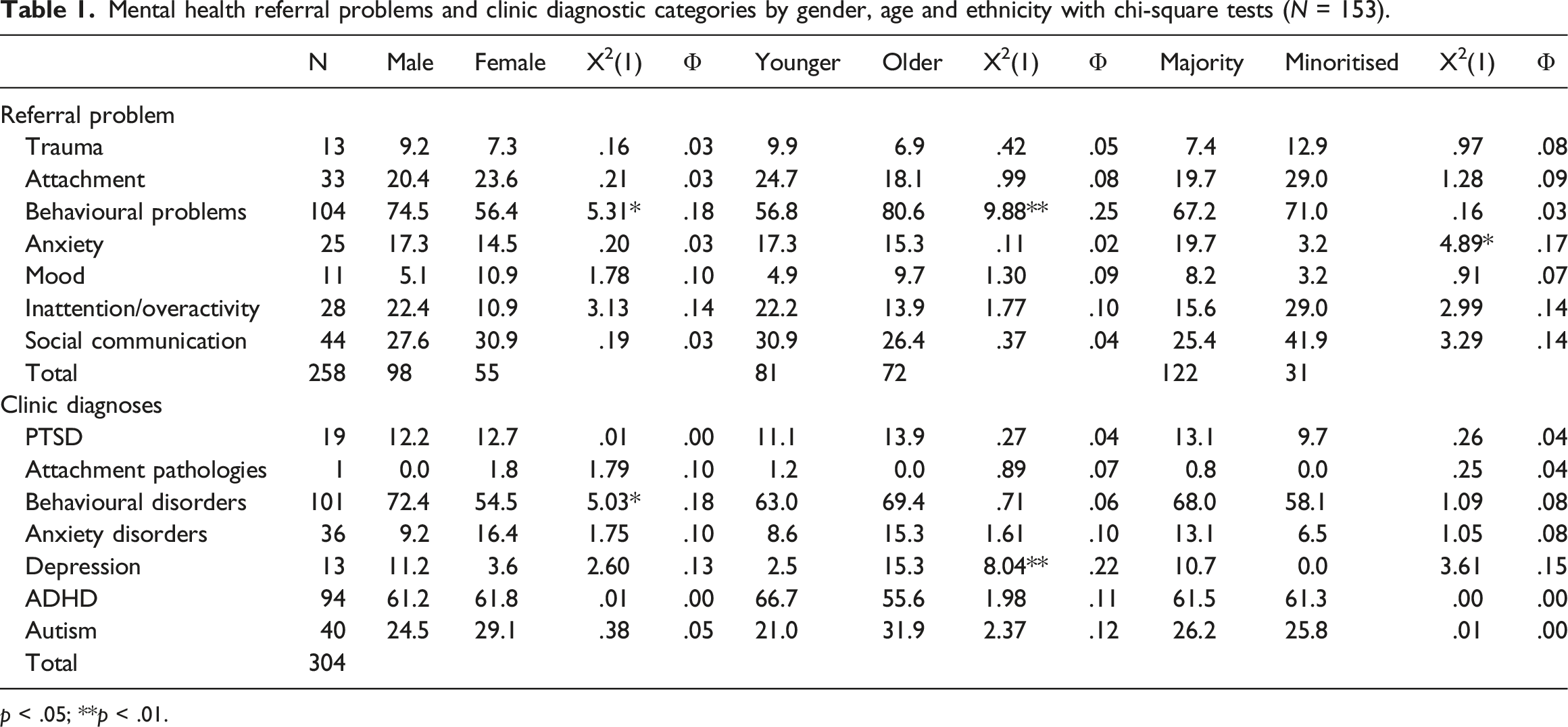
p < .05; **p < .01.
Mental health
Of the 153 cases referred, 21.6% of the letters referenced problems with attachment and 8.5% trauma, of which seven mentioned both attachment and trauma (4.5%). Thus, prior to the requirement that all referrals be exclusively for ‘attachment or trauma’ only a quarter (25.4%) of the social workers’ referral letters spontaneously mentioned either or both of attachment and trauma.
The most common referral problem (67.9%) was for behavioural problems, followed by the categories of social communication (28.7%) and attention and concentration (18.3%) relating to neurodevelopmental conditions. Lastly, 16.3% of referrals mentioned anxiety and 7.1% low mood. More boys (74.5% vs 56.4%, X 2 (1, N = 153) = 5.31, p < .05) and older children (80.6% vs 56.8%, X 2 (1, N = 153) = 9.88, p < .01) were referred with concerns about behavioural problems. Fewer children from racially minoritised groups were reported to have anxiety problems (3.2% vs 19.7%, X 2 (1, N = 153) = 4.89, p < .05) in the referral letters.
Referral diagnoses
103 pre-existing diagnoses were mentioned in the referral letters, of which 73 (70.8%) were formal mental health diagnoses distributed across 17 different conditions (most commonly ADHD and autism, in 14.3% and 6.5% of the cases respectively). Of the remaining conditions identified in the referral letters 16 (15.5%) were physical health diagnoses (e.g., foetal alcohol or chromosomal disorders) and a further 14 (13.5%) used diagnostic neologisms such as ‘disorganized attachment disorder’. Due to the small numbers of pre-referral diagnoses these will not be analysed further.
Clinic diagnoses
The clinical assessment identified 334 diagnoses, across 16 different conditions, with an average of 2.18 per case (sd = 1.03, range 0 to 5), representing a 4.5-fold increase compared with the number of pre-existing mental health diagnoses. Only 5.9% of referrals did not receive a diagnosis. The majority of the diagnoses (N = 304) fitted into the seven diagnostic clusters (see Table 1) the remaining 30 (8.9%) were a range of low frequency conditions, including enuresis/encopresis; tic disorder; eating disorder, and are not analysed further in this paper due to the heterogeneity of the resulting category.
The total number of diagnoses did not differ by gender (t = .72, ns), age group (t = .84, ns) nor ethnicity (t = 1.54, ns). Table 1 presents the clinic diagnostic groups along with the associations with gender, age and ethnicity. Boys were more likely to be diagnosed with conduct problems (72.4% vs 54.5%, X 2 (1, N = 153) = 5.03, p < .05), but unexpectedly, both boys and girls showed equivalent rates of ADHD and autism. Children over 10 were more likely to be diagnosed with a depressive disorder (15.3% vs 2.5%, X 2 (1, N = 153) = 8.04, p < .01). There were no differences for ethnicity.
The most frequent diagnoses were behavioural problems (66.0%), followed by ADHD (61.4%), while autism was diagnosed in just over a quarter of the cases (26.1%). Specific diagnoses within the anxiety cluster were identified for 23.5% cases, of which the majority (12.4%) were for separation anxiety disorder specifically. While only one case (0.6%) was diagnosed in the clinic with an attachment-related pathology (DSED), 12.4% were diagnosed with PTSD.
Agreements between the referral problems and the clinic assessments
Frequencies referral problems and corresponding clinic diagnoses with kappa agreement (N = 153).
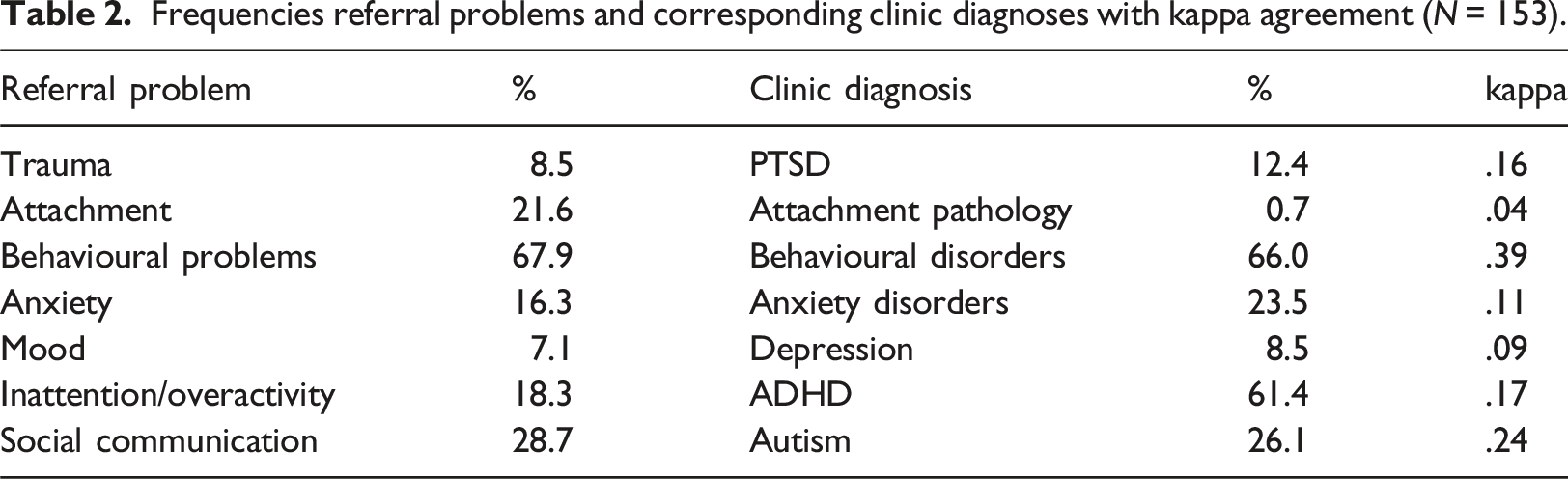
Notably, while attachment was mentioned as a problem in 21.6% of the referral letters, only one case was diagnosed with a formal attachment related diagnosis (DSED), although that case was one of the 33 mentioned as having attachment problems at referral. Of the cases that had had trauma flagged up as a concern in the referral letters, again there was low agreement with the clinic diagnosis of PTSD (kappa = .16). Of the 13 cases identified with trauma problems in the referral, only 4 (30.7%) received a diagnosis of PTSD, and almost 80% (15/19) of the new cases diagnosed with PTSD had not had trauma related issues identified pre-referral.
Discussion
The current paper investigated how post-adoption social workers, as non-mental health professionals, seek support from specialist mental health services for care experienced children in permanency arrangements, by comparing the issues raised in their referral letters with formal clinical diagnoses.
Contrary to predictions, only a quarter of the referrals identified issues with either or both of attachment (21.6%) and trauma (8.5%). Instead, a wide range of other concerns were raised in the referral letters, with an average of approximately three per case, indeed, attachment and trauma comprised less than 10% of the 465 referral problems in the social workers’ referral letters. Just over half of the referral problems could be mapped onto possible mental health conditions, and the rest to more general educational, wellbeing and adjustment issues. The most common mental health referral problem, in approximately two-thirds of the cases, was behavioural problems, followed by concerns about autism in over a quarter. This pattern of a wide range of co-occurring referral problems rather than just attachment or trauma corresponds closely to the diverse mental health concerns raised by adoptive parents who were seeking support from CAMHS services for their children during a similar period (Woolgar et al., 2024). It is also consistent with research on both the range of mental health conditions likely to be found in care experienced children in the UK (Ford et al., 2007), as well as the international studies looking at problems reported for adopted children (Behle & Pinquart, 2016).
Given that almost all children had at least one mental health diagnosis identified, with an average of just over two, post-adoption social workers’ assessments were identifying appropriate cases for referral to the specialist clinic, especially as so few of the children had had mental health diagnoses identified prior to referral. The most commonly identified diagnoses in the clinic were behavioural problems and ADHD (approximately two-thirds of cases for each), but also significant numbers of children with autism and anxiety diagnoses (approximately a quarter for each), amongst 16 different diagnoses across the 153 assessments. The rates of behavioural problems correspond closely to a large survey of adoptive parents in the UK which reported that approximately 60% had been victims of violent or aggressive behaviour enacted towards them (Adoption UK, 2024) and with a survey of what kinds of help adoptive families wanted from CAMHS (Woolgar et al., 2024). Almost two-thirds of the sample referred to the clinic were boys, and this probably influenced the excess of behavioural problems over more internalising issues (depression and anxiety in particular) because boys are consistently identified with behavioural problems and these are also more likely to be noticed by adults due to their disruptive impact on parenting and education, even though for young people as a whole, the rates of all mental health conditions are similar for boys and girls (NHS England, 2023). Hence, this clinic-referred sample is unlikely to be representative of the overall mental health needs of adopted children because help was being sought from a specialist clinic, and thus likely biased towards higher levels of mental health issues, especially for the externalising disorders more often identified in boys. However, as noted above there is no epidemiological data for adopted children’s mental health needs in the UK to compare with, so we cannot determine this. Similarly, much higher rates than usually found in community samples were identified for ADHD and autism (61.4% and 26.1%, respectively) for boys and girls equally, but again it is not possible to know whether this unexpected gender parity for neurodevelopmental conditions is typical in the adoption population without epidemiological data.
Notably, only one child out of 153 met criteria for an attachment-related pathology, (DSED) and only 12% for PTSD, emphasising that attachment and trauma diagnoses were not the primary mental health issues for these children. It has been noted previously that formal attachment related diagnoses are uncommon, even in severely neglected samples (Zeanah et al., 2016) and there has been a tendency to over-identify attachment-related pathology in adopted and looked after samples referred by mental health professionals for assessments (Allen & Schuengel, 2020; Woolgar & Baldock, 2015). It is unlikely that social workers were using attachment terms to map onto specific attachment diagnoses. Their concerns may refer more to the fact that adopted children have the developmental task of establishing new attachment relationships with new attachment figures and thus about the quality of the relationship that has emerged and how its development may not be progressing as well as hoped. Such variations in attachment relationship quality are very different to the diagnostic approach of gross distortions in the fundamentals of the attachment system (Opie et al., in press). In the light of these uncertainties about what different professionals mean when using attachment constructs clinically, one recommendation from the research looking into the mismatch amongst mental health practitioners and their understanding of attachment problems was that attachment problems should be carefully defined and described, so that there is clarity about what kinds of issues are being understood as specifically attachment-related for any given child (Woolgar & Baldock, 2015). Doing this would help here to ensure a shared understanding of what those problems are and the extent to which these problems make sense primarily as issues of attachment or whether better understood under another condition.
So, although social workers’ assessments of therapeutic needs were conceptualising more of the children’s issues as attachment problems than were ultimately identified in the clinical assessments as frank mental health conditions, it was still a minority of cases. So at this point in implementation of the ASF, social workers were not typically succumbing to “the allure of rare disorders” (Haugaard, 2004, p. 127) by routinely ascribing attachment pathology to children with histories of maltreatment and neglect. The argument made by Haugaard was that while rare conditions may be seen more often in maltreated children, they are still rare. Common conditions are still more common and indeed are seen more often in this group than in non-maltreated children, so there is frequently an issue of co-occurrence and comorbidity of common conditions alongside the occasional possibility of rare conditions. This was further elaborated by Chaffin et al. (2006) for attachment problems specifically, who reported a tendency to over-ascribe both the formal rare attachment conditions (at that point in time the two DSM-IV subtypes of reactive attachment disorder) as well as informal attachment-based diagnostic neologisms, at the expense of identifying “common but less exciting” (p82) conditions. Following from the tendency to miss treatable common conditions, there was then the risk that therapeutic support offered to maltreated children was not evidence-based and at times was even harmful. However, since the change of the ASF criteria so that social workers in England can only identify issues to do with attachment or trauma to receive funded support, this tendency to over-identify issues as attachment is likely to have increased.
Although few cases were identified with trauma related issues, the figure of 12% of cases with formal PTSD corresponds closely to contemporaneous research conducted in Wales on the mental health needs of a cohort of adopted children (Anthony et al., 2022). While only a minority of cases were diagnosed with PTSD, the figure still represents a significant increase on the rate expected in the general population, and while these figures for PTSD might seem low given that adopted children are likely to have been exposed to a range of traumatic events, typically only about 16% of children exposed to traumatic events subsequently develop PTSD (Alisic et al., 2014). However, the likelihood of developing PTSD varies according to a number of resilience and risk factors (Trickey et al., 2012), with risk factors expected to be higher in the care experienced cohort. Indeed, within UK care experienced youth rates of PTSD have been found to be higher, albeit still only for a minority of cases, at around 20% (Hiller et al., 2021) but this is almost 50% higher than identified in the clinic. One possibility is that there was more unidentified PTSD that was not being referred by post-adoption social workers for specialist assessment, and that perhaps their problems were being viewed under a different lens. Indeed, the vast majority of children, almost 80%, identified in the clinic with PTSD had not had trauma flagged up as a referral problem by social workers, which is not surprising given even clinicians significantly under-identify PTSD in care experienced young people compared with those in birth families (McGuire et al., 2022). Interestingly, both ADHD and autism were more commonly identified than PTSD in this sample, and there are many ways in ways in which the experience of being neurodivergent interacts with risks around negative life events and psychological trauma (Golm & Brandt, 2024). A failure to carefully assess and then formulate both adverse experiences and neurodivergence jointly (Cawthorne & Woolgar, 2025; Pinto, 2025), risks a “double jeopardy” for maltreated young people, potentially exacerbating the impact of both (e.g., Gajwani & Minnis, 2023).
Less than half of the children referred to the clinic had pre-existing mental health diagnoses identified, and the clinic identified over four times that number, suggesting these young people had not been comprehensively assessed for mental health problems prior to referral. Of course, one reason for a referral to the clinic could be to consider formal mental health diagnoses, but for a national specialist clinic, it would be typical for young people to have already had some contact with community CAMHS, especially given the extent of the mental health issues these young people presented with. Recent evaluations of the ASF in England have identified some unintended consequences of its implementation, including adopted children being denied access to standard CAMHS services because of the availability of this alternative provision (Selwyn & Lewis, 2021). A risk following from this is that if CAMHS increasingly rejects referrals for adopted children then opportunities for the stakeholders to encounter different perspectives, to translate between them and to come to a shared understanding of the issues will also reduce. A downstream risk of this is that there will likely be further divergence between professional groups in how adopted children’s mental health needs are understood, impacting upon how effectively families are able to negotiate between these perspectives.
Where mental health conditions had been previously identified, a notable minority (16%) were for idiosyncratic terms such as ‘disorganised attachment disorder’. Presumably, these diagnostic neologisms attempted to capture something important about the child’s presentation, but because they do not correspond to well-defined constructs their meaning remained obscure. Unfortunately, it is not possible to know whether these were idiosyncratic ‘disorders’ created by post-adoption social workers, or if they had been assigned in previous mental health assessments, either in CAMHS or from the large number of alternative non-statutory services commissioned by the ASF (Woolgar et al., 2025), or even if they were the result of transcription errors into the referral letters. However, whatever their origins, they had become part of the child’s clinical record, potentially shaping access to services.
A substantial minority of cases (15.5%) had pre-existing health conditions identified, including chromosomal and foetal alcohol disorders, presumably picked up as part of paediatric assessments. While none of the referrals from social workers during this period mentioned concerns about foetal alcohol exposure, the clinic did routinely assess cases referred for these issues from other NHS services, but as these cases were not referred via the ASF, they are not part of the current series. Interestingly, over the following years increasing numbers of children were referred by social workers via the ASF with concerns about possible foetal alcohol exposure, suggesting an increasing awareness of the issues developing over that decade consistent with national patterns (Whincup et al., 2024). Where these later cases were described as having had exposure to foetal alcohol it was typically used as evidence of a “trauma” as required for the referral to be considered under the attachment and trauma restrictions. Hence the concept of trauma was extended beyond the usual mental health meaning of the psychological legacy of adverse events to a physical health condition. While exposure to foetal toxins, including but not restricted to alcohol, were certainly part of the biopsychosocial formulations for the adopted children assessed in the clinic (e.g., Pinto, 2019), they are not usually considered psychological trauma.
Comparison of the mental health problems raised in the referral letters mapped onto the diagnoses made in the clinic assessment revealed very low agreement, even when the frequencies of diagnosed conditions and problems raised in the referral letters were similar. For example, two-thirds of the referral letters mentioned behavioural problems as an issue and while behavioural problems were identified at a similar proportion in the clinic, the agreement was still poor. Thus, there was little evidence for a shared understanding of problems between social workers and the clinic, or that referral problems could guide the focus of the mental health assessment.
When free to select any problems for referral few post-adoption social workers spontaneously referenced attachment or trauma. Unfortunately, all referrals using the ASF in England are now constrained to be only for attachment and trauma, so social workers must identify one of these to be able to access funding. This suggests that either three quarters of the cases presented here, even with their high levels of mental health comorbidity, would no longer be eligible for referral to the clinic, or that to be eligible, the referral problems would need to be recast as either or both of attachment or trauma, even though these terms did not adequately describe the issues, neither for social workers making the referrals, nor in the clinic at assessment, and would likely further compound the conceptual confusion between practitioners. Given the poor agreement evident here between professionals about these terms, constraining the referral issues so narrowly risks increasing barriers for inter-professional collaborative working (McGuire et al., 2022), as well as blocking access to effective evidence-based interventions for young people with high levels of mental health need.
Future studies could investigate whether the understanding of attachment and trauma amongst non-mental health professionals such as social workers or teachers, and of course with families, is internally consistent (e.g., when a social worker uses the term ‘attachment’ they use it in similar ways to other social workers) as well as the extent to which understanding overlaps with terminology used in mental health services or amongst other stakeholders. Research has already shown that attachment has a wide range of meanings amongst clinicians in the UK (Beckwith et al., 2022) and internationally amongst social workers (Bjerre et al., 2023; Hammarlund et al., 2022), but no research has explored how variations in meanings within and between professional groups could influence adopted and care experienced young people’s access to services. It seems likely that there is a similarly wide range of divergent understandings for the meaning of trauma within and between different practitioner groups, especially as the lay meaning of trauma can simultaneously relate to a variety of issues including physical wounds; negative events; as well as the short- or long-term psychological consequences arising from negative events. Studies could explore the various meanings of the trauma conceptualisations applied to care experienced children using Q-sort methodologies as in Beckwith et al. for attachment. A related approach would be to use consensus building methodologies. For example, a recent Delphi study amongst practitioners explored the possibility of finding consensus amongst clinicians for issues of autism, attachment, trauma and personality disorders (Sarr et al., 2025). That study was not focussed on the population of adopted or care experienced young people, nor did it give voice to adopters themselves. However, Delphi approaches have been used in other areas to explore the possibility of consensus between different stakeholders including families (e.g., Barrington et al., 2021), so it would be possible to design studies that included the adopters’ voice directly in building consensus and shared understanding of critical issues.
This highlights a limitation of the current study regarding the absence of adopters’ perspectives, including how they responded to the clinical reports, to the professional disagreements and to the different conceptual frameworks that arose. Did they prefer the conceptualisation of needs in the referral problems or the diagnostic and formulation-based reports that they received? While satisfaction surveys of the post-adoption support or clinical assessments could provide some initial information about this, it would be insufficient to explore this thoroughly because these could not tell us how families experienced being caught between the different narratives evident here. Moreover, families themselves may have differing narratives to account for their perceived needs from the different services. Going forward research that captures the family’s voice and is also open to the multiple positions that they are likely to hold, as well as how these influence their experiences of negotiating services amongst the different stakeholders is needed.
A further limitation of the current study is the use of the kappa statistic to measure agreement where agreement usually applies to raters using the same categories, but here the assessments that guided the social worker’s referral letters were not organised around the diagnostic categories used in the clinic and needed to be translated into those categories. This means we cannot extrapolate from the kappa statistic rates of diagnostic mismatch. Rather, we used percentage agreement and the kappa to illustrate the difficulties that would follow were clinicians to accept the issues in the referral at face value as referring to formal mental health conditions, and for these issues to then guide the focus of clinical assessments. The results here show that these referral letters cannot reliably to do that, which means that a clinically appropriate assessment may need to differ significantly from what was requested, which in turn raises issues for a shared understanding of issues. Given this, future research could investigate referrer satisfaction with the commissioning of assessments which ultimately deviate substantially from the referral concerns. Related to this, a further limitation of the current study is the focus on psychiatric diagnosis rather than broader formulations, because the latter are likely to be especially helpful for a cohort of young people with diverse and overlapping needs and for whom personalised formulations are likely to be most helpful (Pinto, 2019). Often the primary issues for families are not comprehensively captured by formal mental health conditions, and indeed important concerns such as difficulties with peers, school, or transitions etc. (Woolgar et al., 2024), can arise out of multiple mental health issues or indeed be wholly independent of them. Formulations may well help families and social workers make sense of the different ways in which the problems are construed in the clinic compared with the referrals. Further work could explore the fit between post-adoption social workers’ understanding of therapeutic support needs, families’ concerns and mental health formulations constructed in CAMHS services, alongside whether such formulations then enable access to helpful treatments.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
Institutional Review Board service project approval p8.
Consent to participate
Anonymised service data, consent waived by IRB.
Data Availability Statement
Unavailable as clinical record data and no consent for sharing outside the clinical systems.