
Abstract
As a response to the substantial health problems and unmet needs among children in out-of-home care, a comprehensive health assessment was piloted in a Norwegian region, as the first of its kind in Norway. The current study is a follow-up of service use among children who received the assessment, designed to investigate the relationship between service recommendations and service contact with six services within the following year. Participants included children (ages 1–17 years) living in out-of-home care, who had received the health assessment (N = 103, M age = 7.5 years). Baseline data on service recommendations were extracted from assessment reports, while data on service contact was collected through a survey to carers 12 months after the assessment. Bivariate analyses and logistic regression models tested associations between service recommendations and service contact. Results show that for low-threshold services within municipal primary health care, recommendations were associated with service contact (OR 5.0, [1.65–15.19] p = .001). For specialized mental and somatic health care and educational services, no associations between service recommendation and service contact were found. Around 40% of the children had been in contact with recommended specialized mental or physical healthcare services, and educational services at follow-up. The findings illustrate the failure of the existing service systems in meeting the severe health challenges of this high-risk child population. This has implications for assessment practices, child welfare services referral routines and interagency collaboration, and may indicate a need for specialized organizational solutions to provide necessary services to children in out-of-home care.
Keywords
Introduction
Children placed in out-of-home care 1 (OOHC) have higher rates of mental health, medical and educational problems than the general child population (Bronsard et al., 2016; Kling et al., 2016). A large body of research provides compelling evidence that children in OOHC have special health care needs and are prone to suffer significant health issues throughout their lives (Goemans et al., 2015; Gypen et al., 2017; Villodas et al., 2016). With a mental health disorder prevalence between 50% and 70%, children in OOHC represent an unparalleled high-risk child population (Bronsard et al., 2016; Chambers et al., 2010; Haune et al., 2023; Lehmann et al., 2013; Milburn et al., 2008). The high levels of health problems are a result of multiple factors, including pre- and postnatal exposure to stress, exposure to abuse and neglect, and disturbed attachment with caregivers (Rutter, 2000; Szilagyi et al., 2015). In addition, there is substantial evidence for a system failure and a lack of routines for identifying needs and providing necessary services to children in OOHC (Lee et al., 2015; Leslie et al., 2000; Mensah et al., 2020; Vinnerljung & Hjern, 2018).
Although children in OOHC often have higher rates of service utilization than their non-fostered peers, they do not receive sufficient care given their level of need (Christian & Schwarz, 2011; Lee et al., 2015; Stein et al., 2016; Vinnerljung & Hjern, 2018). Studies report that the use of child and adolescent mental health services (CAMHS) in particular, is not according to needs (Larsen et al., 2018; McLean et al., 2021; Minnis et al., 2006; Tarren-Sweeney, 2010a), but these children are also underserved by somatic health care services and educational services (Jaudes et al., 2004; Petrenko et al., 2011; Scherr, 2007). Unaddressed health issues may have long-term consequences for their physical and mental health, relationships, education, and employment (Szilagyi et al., 2015).
International guidelines and a substantial body of literature have recommended that comprehensive health assessments should be provided to all children entering OOHC, to detect unidentified and/or unmet health problems, and to ensure early intervention and appropriate referral to services (American Academy of Pediatrics, 2000; Chambers et al., 2010; Leslie et al., 2005; Vinnerljung & Hjern, 2018). Studies of comprehensive health assessment models have reported the detection of substantial mental health, medical, and educational needs (Haune et al., 2023; Hill & Watkins, 2003; Nathanson & Tzioumi, 2007; Petrenko et al., 2011).
It is less clear whether health assessments lead to the receiving of appropriate services. An Australian study found that between 69% and 79% of the recommendations had been or were being implemented within 6–18 months of the assessment (Nathanson et al., 2009). A study from the USA reported that post-assessment recommendations increased the likelihood of receiving the services. However, 50% of the children still had unmet mental health needs, and more than 80% still had unmet educational needs one year after the assessment (Petrenko et al., 2011). Another study from the USA found that the assessment increased the likelihood of being referred to mental health services, but it did not influence the likelihood of receiving the services (Bunger et al., 2021). Due to substantial variations in assessment models and methods across studies, and differences between nations in the organizing of services, comparisons must be made with caution. Nevertheless, the research status in the field necessitates further investigation into the effect of health assessments on service use.
At the end of 2023, there were 9,255 children (aged 0–17 years) residing in OOHC in Norway (Statistics Norway, 2024). Norway provides no national figures on service utilization for children in OOHC, although the neglect of their health care needs has been emphasized in recent studies and in national reports (Directorate for Health/Directorate for Children, Youth and Family Affairs, 2017; Lehmann & Kayed, 2018). As a response to this, the Children at Risk Evaluation (CARE) assessment model was developed and piloted, as the first of its kind in Norway. The multi-disciplinary assessment teams identified high levels of mental disorders and previously unrecognized service needs across a range of services among the 196 participating children (Haune et al., 2023). The current follow-up study was designed to examine whether the service needs were met within the first year of the assessment, and to gain knowledge of the influence of the assessment on service receipt.
Study aims
Our aim was to examine whether the service recommendations were associated with service contact within one year of the assessment. We investigated whether children for whom a service was recommended at baseline exhibited a higher likelihood of engaging with this service, and/or had a greater number of visits than children without a service recommendation, within 12 months after assessment. The study included six services from three different sectors: General Practitioner (GP) and municipal health clinics (primary health care services), CAMHS and specialized somatic health care (specialized health care services), and educational psychology services (EPS) and special education (educational services).
Methods
The CARE assessment model
The CARE assessment model was piloted in the Southern Region of the Norwegian State Child Welfare Services (CWS); see Figure 1 for a description of the assessment model and its key components. Within a three-year period, CWS offices were invited to refer all children entering OOHC for a comprehensive assessment of their mental and physical health and development. Dental health care was also included in the comprehensive assessment, and when a need was identified, an appointment with a dentist was arranged after the assessment day. This was deemed necessary for 19.9% (n = 39) of the children at baseline (Haune et al., 2023). Further follow-up on dental health care was not included in the current study. Multi-disciplinary teams of specialized clinicians (a medical doctor/psychiatrist, a clinical psychologist, and a social worker) conducted the assessments, using standardized assessment measures. The recommendations for further mental or physical health evaluation or treatment were based on established clinical cut-points and clinical judgment. Recommendations for the further educational evaluation of services were based on scores that were below average or discrepancies between scores on measures and clinical assessment. Details of the health assessment performed, and measures used, have previously been described (Haune et al., 2023). Key components of the assessment model.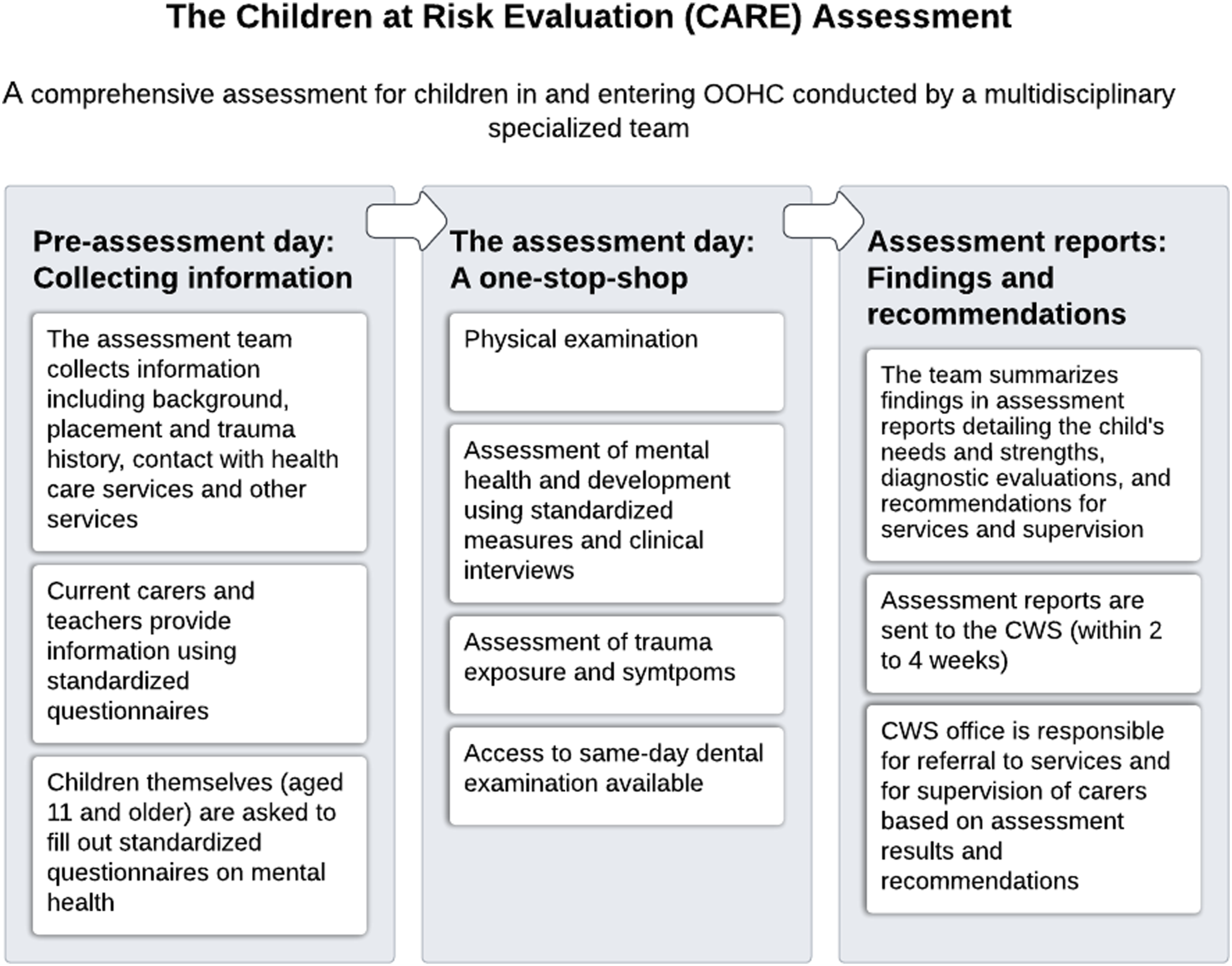
Study design
This is a follow-up study of a cohort of children in OOHC who received a multi-disciplinary health assessment. Baseline data were extracted from assessment reports retrospectively. Data at follow-up were collected 12 months post-assessment through a survey provided to carers.
Recruitment and participants
The study population included children who had received the CARE assessment during the two-year inclusion period. Carers for 168 eligible children (85.7% of the baseline study population) received a survey on child service use 12 months after the assessment. A completed survey was returned for 103 children (61.3% of the follow-up study population). Figure 2 provides a flowchart of the data collection process Flowchart of data collection.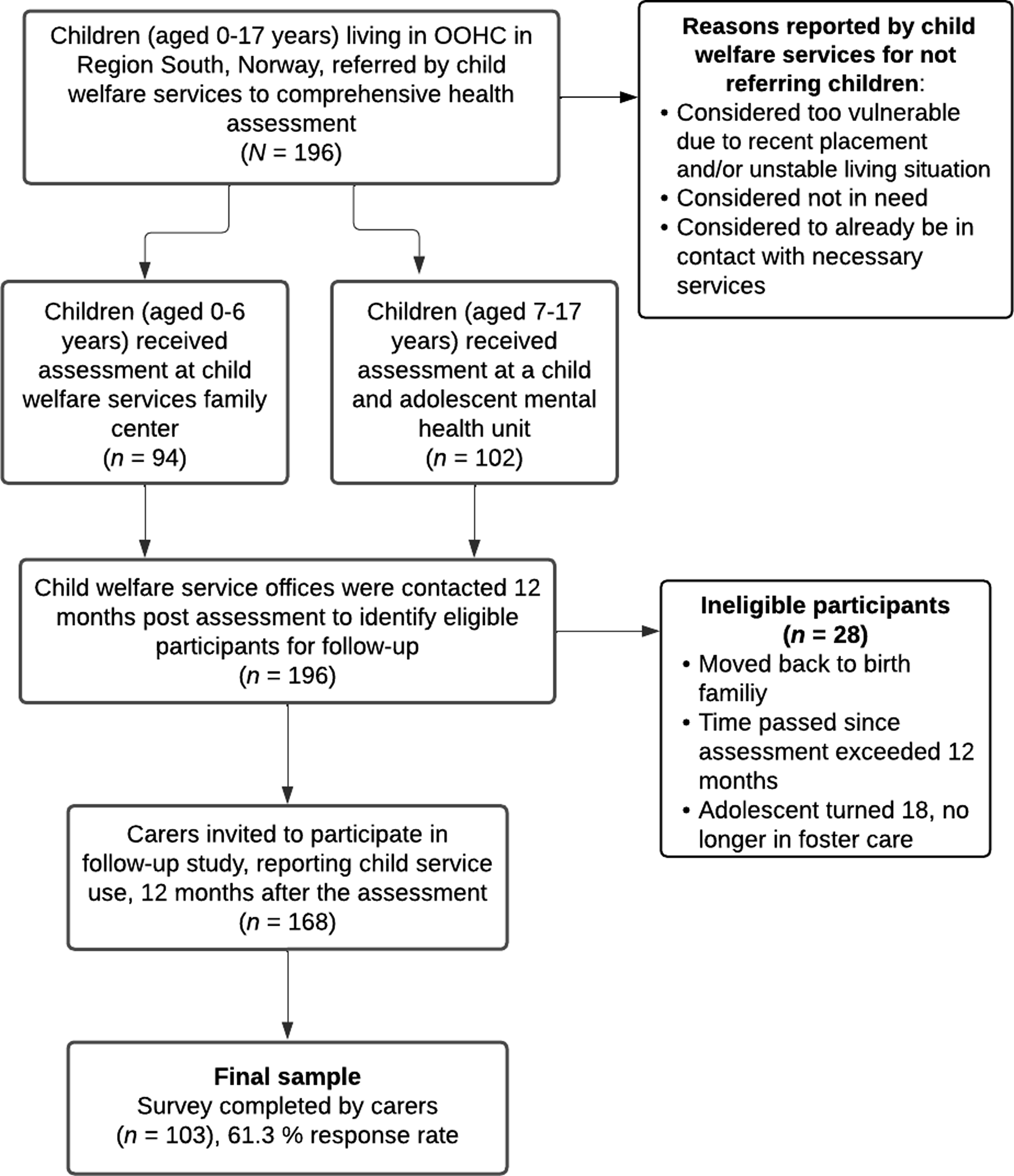
Procedures
Baseline data were extracted retrospectively from the assessment reports and coded by the first, fourth, and fifth authors. Approximately 12 months post-assessment, eligible carers were contacted by e-mail and/or telephone and invited to participate in the study. They received an information letter describing the study and how to complete the survey. The survey was completed online through secure webpages. If the child had recently moved (within the past month) and the current carer had limited knowledge of the child in their care, the previous career was contacted and invited to respond. There was no compensation for participation.
Ethics
The study received approval from the Norwegian Centre for Research Data (NSD). The Norwegian Directorate for Children, Youth and Family Affairs and the Council for Confidentiality and Research mandated the CWS to consent to participation in the study in the place of biological parents and provided exemption from confidentiality for CWS officers.
Variables and measures
Service recommendation
Baseline data on service recommendations were coded from the assessment reports and plotted into a retrospective form (recommendation for new service = 1, no recommendation for new service = 0) for each service. This variable included only recommended new referral to a service, and not recommended continuation of existing service contact. The following services were included: GP, municipal health clinics (including low-threshold mental and physical health services for young children, families, and adolescents, and school health care), CAMHS, specialized somatic health care (including pediatrics, habilitation, and specialized units for effects of intrauterine drug exposure), EPS (including educational and psychological counselling), and special education (psychosocial and academic support in school).
Service contact
Service contact was measured through a custom-made questionnaire issued to current carers with questions concerning child service contact during the previous year for all six services listed above. For each service, a dichotomized variable was made, measuring any service contact or no service contact. To measure frequency of service contacts, the following categories were used: every week, every month, every 3 months, every 6 months, and less frequently than every 6 months (more than 6 months between contacts). Only new service contact was included in the current study, and not services that were already reported utilized at baseline (see Figure 1).
Demographic variables and placement stability
Information on age and sex was obtained from the national identity number registry, while placement status was reported by the carers. The placement stability variable measured whether children had changed placement once or more within the past 12 months.
Statistical analyses
All analyses were conducted using STATA 16. We used an alpha level of .05 to indicate statistically significant results. Demographic and placement variables were presented as percentages, means, and standard deviations. Chi-square tests for equal proportions were used to investigate bivariate associations between service recommendation and service contact. Analyses were conducted separately for each service. A set of logistic regression analyses were conducted to assess whether receiving a recommendation for service contact/referral was associated with new service contact, adjusting for age, sex, and placement stability. Odds ratios (OR) and 95% confidence intervals (CI) were calculated as a measure of effect size and are presented for all analyses. A second set of analyses examined the relationship between recommendations for new service contact/referral and the frequency of service use within the following 12 months. The frequency scale was treated as an ordinal response variable. We conducted ordinal logistic regression analyses to model the relationship between service recommendation and the frequency of service contact, adjusting for age, sex, and placement stability. Given the exploratory nature of the study, no formal power analysis was conducted at baseline. Regardless of the significance level found, the results must thus be interpreted with caution.
Results
Sample characteristics
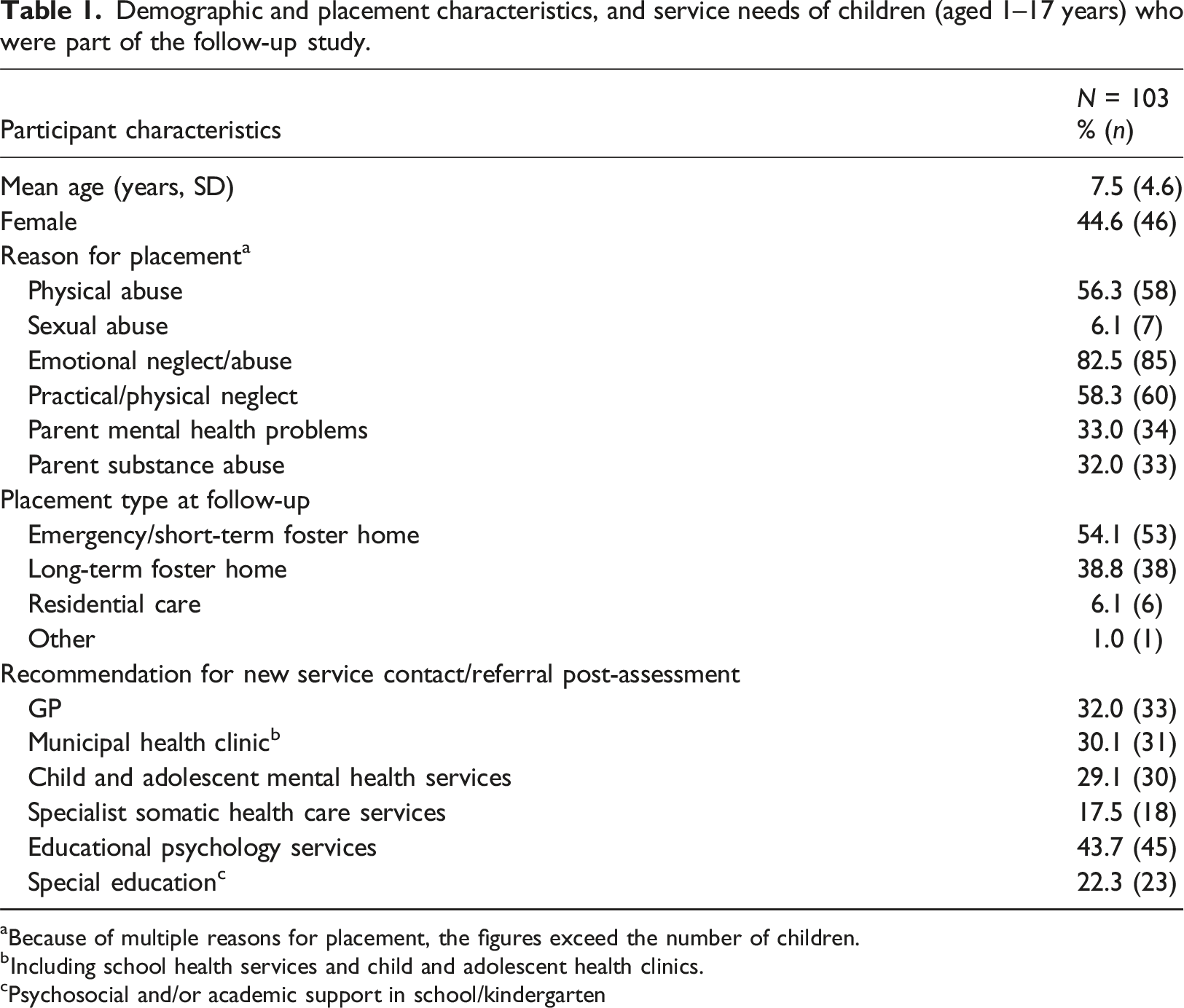
Demographic and placement characteristics, and service needs of children (aged 1–17 years) who were part of the follow-up study.
aBecause of multiple reasons for placement, the figures exceed the number of children.
bIncluding school health services and child and adolescent health clinics.
cPsychosocial and/or academic support in school/kindergarten
Service recommendations
As shown in Table 1, the assessing clinicians recommended contact with GP for 32.0% of the children (n = 33) and with municipal health clinics for 30.1% (n = 31). Referral to CAMHS was recommended for 29.1% (n = 30) and to specialized somatic health care for 17.5% (n = 18). EPS was the single most recommended service, with referral recommended for 43.7% (n = 45) while special education was recommended for 22.3% (n = 23).
Service contact
Overall new service contact among children in out-of-home care 12 months post-assessment (N = 103 a ).
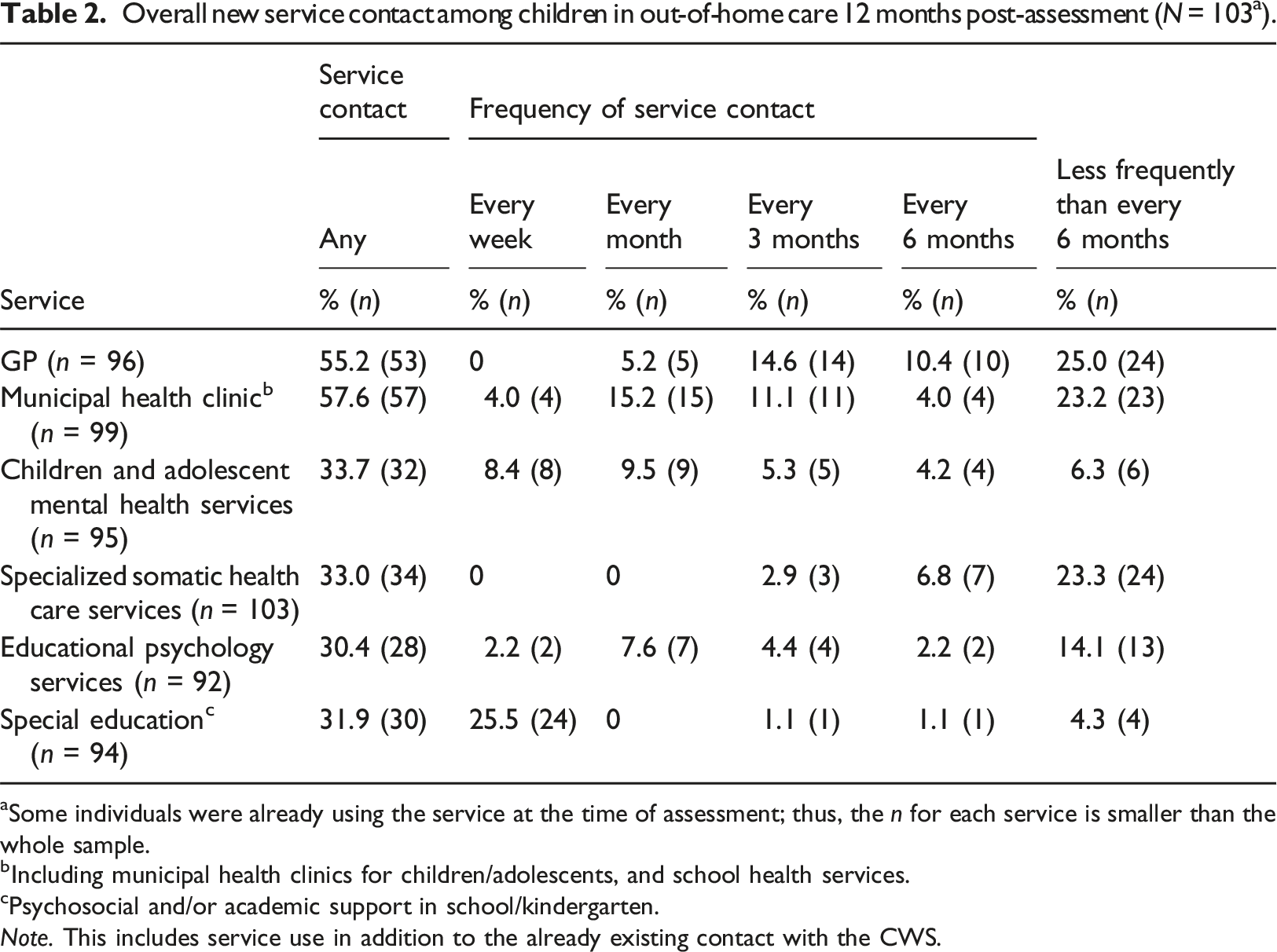
aSome individuals were already using the service at the time of assessment; thus, the n for each service is smaller than the whole sample.
bIncluding municipal health clinics for children/adolescents, and school health services.
cPsychosocial and/or academic support in school/kindergarten.
Note. This includes service use in addition to the already existing contact with the CWS.
Relationship between service recommendations and service contact
Bivariate analyses of differences in service contact between children with and without post-assessment service recommendation.
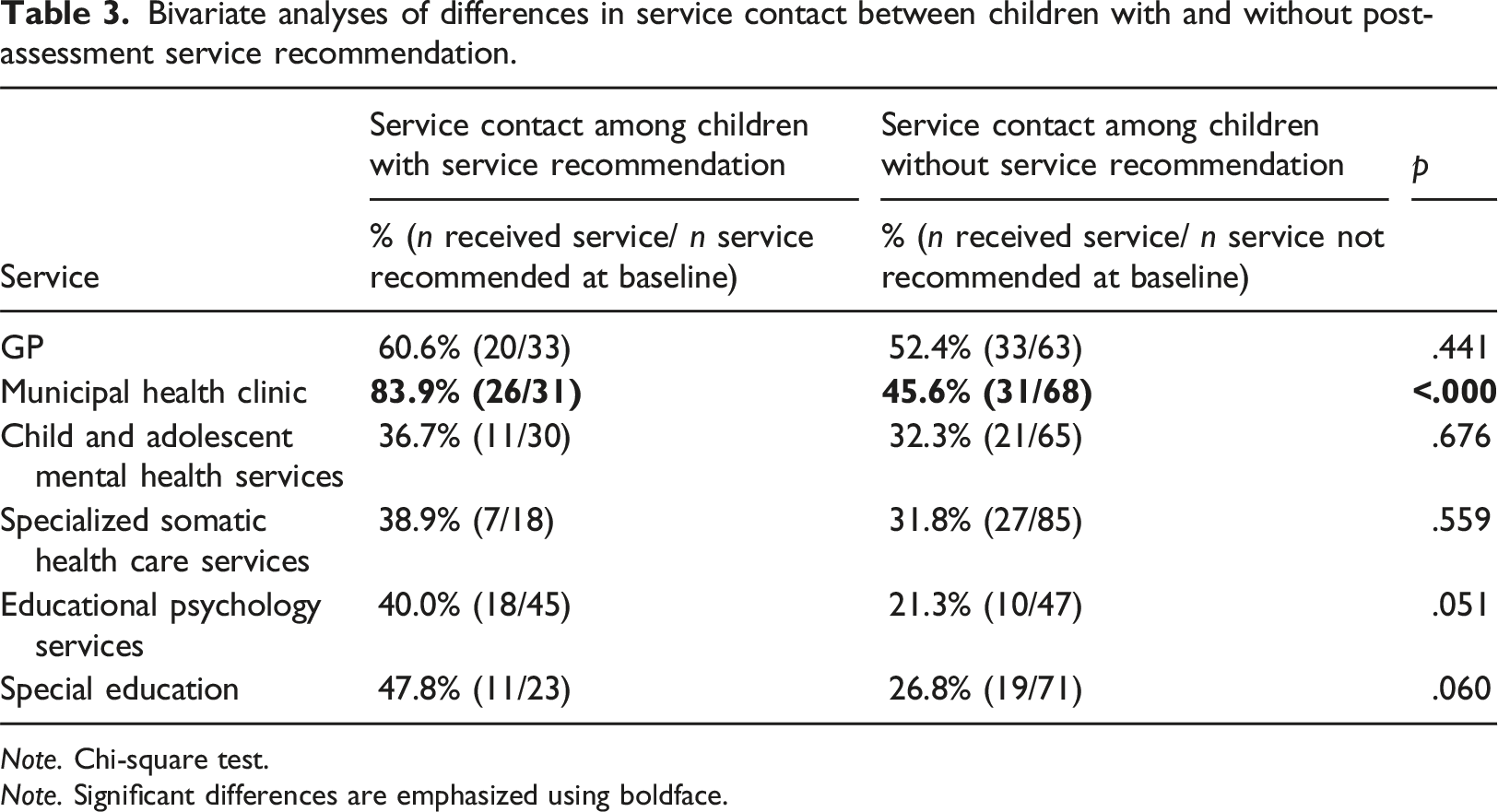
Note. Chi-square test.
Note. Significant differences are emphasized using boldface.
Logistic regression analyses of associations between service recommendation at baseline and service contact the following year, presented as Odd Ratio, 95% Confidence Interval and p-value.
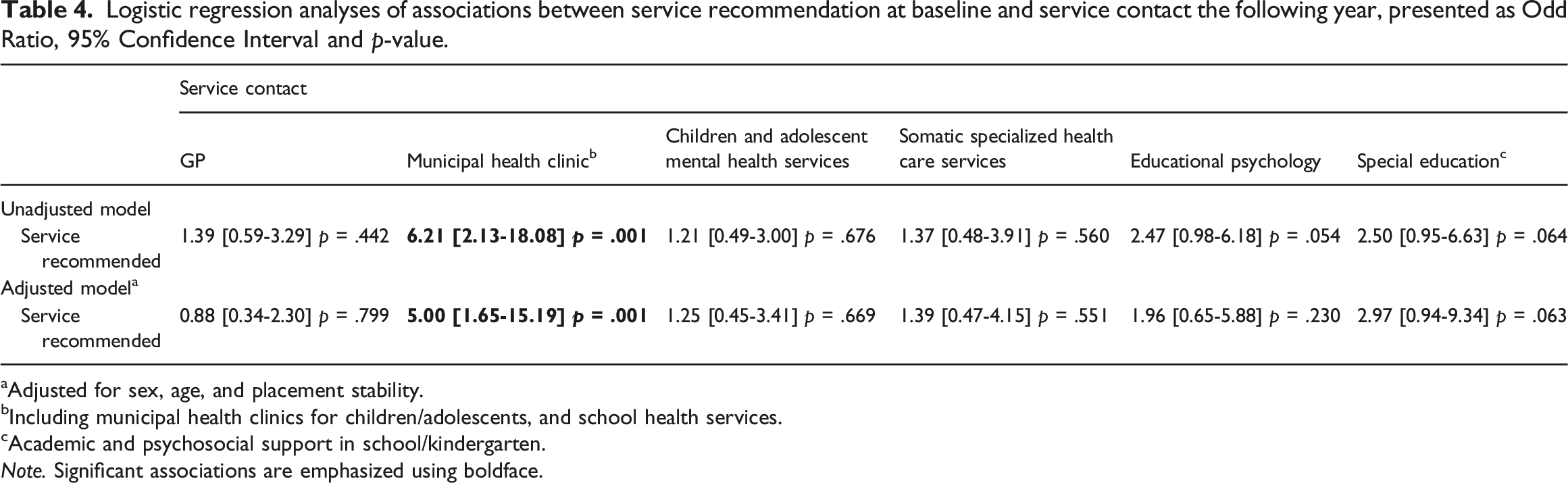
aAdjusted for sex, age, and placement stability.
bIncluding municipal health clinics for children/adolescents, and school health services.
cAcademic and psychosocial support in school/kindergarten.
Note. Significant associations are emphasized using boldface.
To investigate whether a more fine-scaled modeling of the outcome variables would reveal an effect of service recommendation, we conducted ordinal logistic regression analyses, using the five levels of contact frequency (as described in Table 2). The results show similar patterns as found in the logistic regression analyses and the bivariate analyses of dichotomized service contact. Significant associations (p < .001) were found between service recommendations and service use for one service – namely, municipal health clinics – both in the non-adjusted model (OR = 6.57, CI [2.85–15.20]) and after adjusting for age, sex, and placement stability (OR = 6.13, CI [2.5–15.00]). This indicates that the odds of being in the higher frequency category versus the lower category were six times higher for those children with service recommendations for municipal health clinics compared to those without, across all possible cut-points of the outcome. No significant associations were found between recommended service contact and the frequency of service contact in the subsequent year – neither in the unadjusted model nor when adjusting for age, sex, and placement stability for GP (OR = 0.80, CI [0.34–1.90], p = .610), CAMHS (OR = 1.25, CI [0.48–3.25], p = .650), specialist somatic health care services (OR = 1.26, CI [0.44–3.60], p = .661), EPS (OR = 1.48, CI [0.53–4.15], p = .459), or special education (OR = 2.51, CI [0.88–7.22], p = .886).
The survey also included a question about whether children had been offered, but declined, service contact, as we assumed that this information would be available to the carers. Post-hoc analyses were conducted to determine if recommendations were not followed due to children rejecting service contact. Four children declined contact with CAMHS, while three or fewer children rejected contact with other services. Excluding these participants from the analysis did not affect the statistical significance of the results. Finally, some of the factors adjusted for were significant independent predictors of service use. For example, the regression model showed that being male and older in age were associated with receiving special education (OR = 5.65, CI: [1.52–20.98], p = .010, and OR = 1.38, CI: [1.18–1.62, <.001). Since these findings fall outside the study’s main aim, they will not be discussed further in this paper. For more details, we refer to Supplemental Table 2.
Discussion
Although the children in this study had received a specialized health assessment, through which extensive service needs were identified, the recommendations for follow-up did not translate to their service use. Apart from municipal health clinics, the recommendations did not impact the children’s service use in a statistically significant way. These are low-threshold services, accessible to foster carers and children themselves, providing health-follow ups for all children. Our findings indicate that the assessment has had an effect in terms of early intervention, which may serve as an important steppingstone in receiving health care and detecting further needs. Although not related to service recommendations at baseline, the high use of GPs is promising, as they may play an integral role in the health care delivery to this child population and provide consistency in care (Karatekin et al., 2018).
It is disconcerting to note that service recommendations indicating more severe difficulties and pathology were not related to service use at follow-up. Although there may be an effect of assessment on service use that our study lacks sufficient power to detect, the low percentage of service contact with recommended specialized services is disturbing. Only around 40% of the children had been in contact with recommended specialized mental health and somatic health care services, and with recommended EPS. These services are inaccessible to children and foster carers without a formal referral from the CWS or the GP. Research with at-risk youths has shown that when a caregiver is unable to access or manage services, immediate barriers to obtaining or maintaining care arise, which the youths may have limited agency to overcome (Staudt, 2007).
When a government organization carries the parental responsibility for such an extreme high-risk group of children, one might expect strict adherence to recommendations from specialized multi-disciplinary health assessments. However, our findings seem to point toward the opposite: a systematic neglect even when their needs are detected and documented. It is worth reflecting on the ethical aspects of conducting a comprehensive health assessment and identifying needs, and communicating the findings to the children and carers, when the recommendations are not followed through. The assessment itself may raise hopes and expectations for help among children and carers, and the lack of follow-up on what was recommended may contribute to a sense of disempowerment (Haune et al., 2024). It is noteworthy that the CWS reported “considered too vulnerable due to recent placement and/or unstable living situation” as a reason for not referring children for assessment, as described in Figure 2 (Myrvold et al., 2020). This rationale has previously been associated with, and criticized in, CAMHS practices (Lehmann & Kayed, 2018; Minnis et al., 2006). In our view, perceived vulnerability or placement instability should not hinder formal assessment of needs in this high-risk population. This finding highlights the importance of making the health assessment statutory; otherwise, many children’s needs will remain undetected and unmet (Randsalu & Laurell, 2018).
Overall, our findings are in accordance with previous studies of assessment models: a sizable proportion of children for whom service referrals are recommended do not receive them. A comprehensive health assessment for children in OOHC is an important starting point in addressing the needs of these children, but it is not sufficient for improving service access and service use. This raises questions as to why services were not delivered: Did the CWS not refer the children to the recommended services? Were referrals not accepted by the services? Or are there barriers in the communication and/or collaboration between the CWS and other services?
Understanding the gap
Below, we discuss possible explanations for the gap between service recommendations and service contact found in this study.
Firstly, service provision to this child population is challenging. High service needs across a range of services (Haune et al., 2023) and high levels of comorbidity (Lehmann et al., 2013) and chronicity (Chambers et al., 2010) add complexity to planning, interagency collaboration, and service delivery. This leads us to a fundamental question: Who is responsible for the health care needs of children in OOHC? The CWS has the formal and judicial responsibility in loco parentis (‘in the place of parents’), the caregivers provide the daily care, while the birth parents often still have parental responsibility. This tripartite responsibility may contribute to ambiguity, misunderstandings, and failure to advocate for the child (Hill & Watkins, 2003; Tarren-Sweeney, 2010b).
A potential explanation for the lack of service contact, is that the CWS did not follow up on the recommendations. The assessment reports were often content-rich, and information may have been ‘lost in translation’ between the assessing health care personnel and the receiving CWS caseworker. The recommendations may have been perceived as unclear, imprecise or incorrect, they may not have been followed-up due to limited capacity, or they may not have been read at all. The CARE assessment, being the first of its kind in Norway, may not have been widely recognized by all caseworkers, potentially leading to ambiguity regarding the status of its recommendations. Five years after the onset of the CARE study, multi-disciplinary health assessments became a national, government initiative (Child Welfare Act, 2023; § 4-3a), and the assessment reports will perhaps gain more influence as a result.
The instability of key adults may also have affected the follow-up on recommended referrals. The handover of information from one CWS caseworker to another has previously been reported as a concern (Nathanson et al., 2009), which may be relevant in the current study. Although we do not have data on caseworker stability, the high turnover rate among CWS caseworkers is well known (Gopalan et al., 2020, The Norwegian directorate for children, youth and family affairs, 2022). Placement changes and instability of carers have also been reported to increase the risk of children not receiving necessary services (Hambrick et al., 2016). However, in the current study, with approximately 50% of the children having changed caregiver at least once within the past 12 months, we did not find that this influenced service use in a statistically significant way.
Challenges with inter-agency communication and collaboration between CWS and other services may explain why more children did not receive the recommended services. The complex needs of these children cannot be addressed in a vacuum, through siloed service delivery (Modderman et al., 2023). Combined mental and somatic conditions require multi-referrals and necessitate clear routines for coordinating services and interagency collaboration. Lack of routine and complex symptomatology may destabilize the working relationship and influence referral practices (Bunger et al., 2024). Moreover, services such as CAMHS have a history of employing intake criteria that limit or even block access, for reasons such as having the ‘wrong’ diagnosis, not having a stable placement, or being in residential care, which may influence referral and collaboration (Lehmann & Kayed, 2018; Minnis et al., 2006; Randsalu & Laurell, 2018; Tarren-Sweeney, 2010a).
Implications for practice and policy
Regarding further development of assessment practices, our results highlight the need for an implementation strategy to be integrated into the assessment model to facilitate the transition from assessment to service access. A collaborative post-assessment follow-up session may be needed to ensure a full understanding of the nature and importance of recommendations, clarify areas of responsibility, and enhance user involvement. A comprehensive health care plan for each child is recommended, with assessment results fully integrated. Educational needs should be included in this plan, as it has been identified as a key factor in improving long-term outcomes (Forsman et al., 2016). Clear deadlines for recommended referrals should follow the assessment (Horwitz et al., 2000; Simms et al., 2000). Involving foster carers in assessment and treatment planning may also be important (Pasztor et al., 2006). Finally, children themselves should be involved in assessment results, plan for follow-up and other issues related to their health and development (Haune et al., 2024; Ruff & Harrison, 2020; Smales et al., 2020).
Improved referral rates and service access require clear policies and procedures for service planning and delivery, as well as effective collaboration between CWS and other service providers. Governments may underestimate the systemic changes needed to address the complex and severe health challenges faced by children in OOHC, and studies call for specialized organizational solutions to meet these needs (Mensah et al., 2020; Tarren-Sweeney, 2010b; Zlotnik et al., 2015). The practice and policy for health care provision to children in OOHC in England has been identified as the most successful in Europe (Vinnerljung & Hjern, 2018). Although not directly transferable to the Norwegian system, key elements from the English model should be considered in the further development of practice and policy in Norway: For example (i) the use of designated health care personnel responsible for providing health services to children in OOHC and (ii) the establishment of clear national guidelines for local authorities on how to implement assessments, deliver follow-up health care services, and monitor compliance (National Institute for Health and Care Excellence, 2021; Department for Education & Department of Health, 2015). This may be particularly important given the substantial self-governing authority of Norwegian municipalities, which can make the implementation of national policy initiatives challenging.
Future initiatives should include fidelity monitoring to ensure that each component of the assessment, with particular emphasis on follow-up of recommendations, is implemented as intended. Additionally, future research should explore effective strategies for interagency collaboration and organizational solutions, as well as whether the services provided lead to improvements in mental and physical health, and educational attainment.
Strengths and limitations
One of the strengths of this study is the comprehensive and standardized nature of the assessment, which adds weight to the identified needs and the subsequent recommendations. Moreover, the inclusion of several services provides a broad understanding of the impact of the assessment and service use. There are relatively few international studies of service use after assessment, and in a Norwegian context, this study is unique. The findings should, however, be considered in the light of several limitations. There may be an effect of assessment on service use that our study has insufficient power to detect. A larger sample size would have provided greater statistical power to our findings. Thus, the results must be considered exploratory, and interpreted with caution. In addition, there was known variation in referral rates for assessment between local CWS offices. Without data on real-world attrition, it is difficult to estimate how representative the participants are of the target population, and to what extent selection bias may affect the generalizability of the findings.
Furthermore, as we do not report the potential health benefit for the children, we can only assess whether the child was in contact with the service, and not whether the child received helpful aid. The carers are often those who take the child to the services and are therefore presumably a valid source when assessing service contact, but there may be services received (such as school health services) that the carers are not aware of.
Moreover, there are no measures of ethnicity in this study. Finally, different legislation, practices and organization of services between nations may limit the generalizability of the study. However, this does not undermine the contribution of the findings to the concerning overall picture of the neglected needs of children in OOHC.
Conclusion
The current study provides the first published Norwegian data examining the outcomes of a routine health assessment for children in OOHC in terms of service utilization. For most services, including those indicating more severe mental and physical health problems, service contact was not related to the recommendations from the health assessment. This clearly indicates that identifying needs and recommending service referrals was not sufficient in addressing the unmet service needs of the children. These findings show that this high-risk child population continues to be underserved by the system and point toward a need for improved interagency collaboration and specialized organizational solutions for children in OOHC. This calls for further system development addressing health monitoring and treatment planning, referral practices and service provision.
Supplemental Material
Supplemental Material - From health assessment to service use: Do children in out-of-home care receive recommended services?
Supplemental Material for From health assessment to service use: Do children in out-of-home care receive recommended services? by Monica Haune, Alexander Nissen, Suraj Thapa, Trine M. Myrvold, Øivin Christiansen and Einar R. Heiervang in Developmental Child Welfare
Footnotes
Authors’ note
This work was performed on the Services for Sensitive data, TSD (Tjeneste for Sensitive Data) facilities, owned by the University of Oslo, and operated and developed by the TSD service group at the University of Oslo’s IT Department (USIT).
Acknowledgements
We would like to acknowledge and thank the children, carers and CWS officers who contributed to the study. We also thank the clinicians, coordinators, and managers involved in the assessment teams for their efforts. Finally, we would like to thank project coordinator Anne Åbyholm-Brodal.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Norwegian Research Council (Grant number 256598/H10).
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.