
Abstract
Childhood adversity can include traumatic experiences and exposure to other risk factors; consistently predicting poorer psychosocial outcomes in adulthood. Relatively little research has investigated the impact of cumulative risk exposure in childhood. Using data collected in a specialist clinical setting, we investigated the associations between risk exposure, psychopathology and psychosocial functioning. Participants were children attending the Attachment and Trauma service at Great Ormond Street Hospital in London (N = 132, M = 10.25, SD = 3.35). Data was collected via routine clinical practice during multi-disciplinary assessments. Data was collected on developmental and trauma history, psychopathology, and functioning (CGAS), using standardised measures, clinical interviews, and observations. All children had experienced at least one risk factor, with 78% reporting multiple exposures, including witnessing interpersonal violence (52%), neglect (48%), and physical abuse (42%). Other risk exposures included exposure to alcohol (17%) and substances (24%) in-utero, as well as social risk factors such as multiple foster placements in some cases. In this sample, 65% of children met criteria for at least one psychiatric diagnosis (Anxiety = 31%, PTSD = 28%, Depression = 8%). High levels of functional impairment were found, with 52% of children falling into the highest categories of ‘obvious’ or ‘severe’ problems. Multiple risk exposure significantly predicted PTSD (OR 9.64 (1.1, 83.7)), but did not predict anxiety, depression, or functional impairment. This study highlights the rates of cumulative risk exposure in this clinical sample. The findings demonstrate the importance of detailed and accurate clinical assessments in ascertaining trauma histories in children with known histories of adversity and maltreatment. There are implications for assessment and treatment, such as the importance of clear guidelines on treating PTSD in children with complex trauma histories.
Introduction
It is well established that trauma and adversity in childhood represent significant risk factors for poorer physical and mental and psychosocial outcomes in adulthood (Felitti, Anda, Nordenberg et al., 1998; McKay, et al., 2021). Risk factors in childhood are multifarious and can include forms of trauma such as abuse and maltreatment (e.g. physical abuse, sexual abuse, emotional abuse, and neglect), witnessing violence, or being exposed to other life-threatening or frightening events. Some children face additional complexities related to in-utero exposure to drugs and alcohol, which is also associated with developmental difficulties and poorer outcomes (Easey, et al., 2019; O’Connor, 2014). Literature consistently demonstrates that having these types of experiences in childhood is associated with poorer mental health in adulthood (Chiesa, et al., 2016; McKay et al., 2021; Shevlin, et al., 2008). Whilst there is relatively less literature on the more immediate effects on the mental health of children in the years following exposure to risk factors, evidence suggests that children are at significantly higher risk of developing mental health difficulties such as Post-Traumatic Stress Disorder (PTSD) following trauma exposure compared to adults (Lewis et al., 2019).
The impact of adversity and trauma in childhood can be complex, with a range of mental health, psychosocial, conduct and behavioural difficulties seen (DeJong & Wilkinson, 2019; van der Kolk, 2005). Children exposed to trauma may also be at increased risk of a complex range of difficulties, including those presumed to be of predominantly genetic origin like intellectual disability and neurodevelopmental differences (Ford, et al., 2007). Furthermore, in some cases, children face the additional complexity and adversity of being removed from their birth family and either being looked after (e.g. in foster care or residential care) or adopted. Looked after and adopted children are at higher risk of poorer mental health and psychosocial outcomes (Ford et al., 2007; Greeson, et al., 2011), partly due to the likelihood of having experienced childhood trauma (McSherry & McAnee, 2022). Research also suggests that factors related to being removed from the birth family, such as having multiple foster placements, are associated with higher levels of risk (Newton et al., 2000; Unrau et al., 2008).
In some cases, individuals are exposed to multiple adverse experiences, with research in adults demonstrating an effect of cumulative exposure in childhood on mental health diagnoses in adulthood, including a meta-analysis study suggesting a dose-response effect whereby being exposed to multiple types of maltreatment increased the odds of mental disorder in adulthood (Karatzias, et al., 2017; McKay et al., 2021; Shevlin et al., 2008). Research in children on the impact of cumulative risk is less well established. Some studies have shown that experiencing cumulative trauma in childhood increases risk of diagnosable psychiatric disorders in childhood, such as depression and PTSD (Briggs, et al., 2013; Dierkhising, et al, 2013; Klasen, et al., 2010; Suliman, et al., 2009). A further study suggested that cumulative trauma exposure is associated with symptom complexity in children (Hodges, et al., 2013).
Children who have a history of experiencing multiple traumas are likely to be at highest risk, and go on to develop the most complex mental health difficulties. It is important to improve our understanding of the specific impact of cumulative risk exposure in order to inform effective assessment and treatment interventions. However, research in UK samples using clinical data is sparse in the current literature, with previous studies commonly relying on self-report measures in adulthood (e.g. Chiesa et al., 2016). The reliance on self-report measures is disadvantageous in that it can lead to inaccuracies in measuring mental health diagnoses such as PTSD (Moradi, et al., 2012; Ono et al., 2016), with a lack of agreement often reported between self-report and clinical diagnostic assessments (Cuipers, Hofmann, & Andersson, 2010; Eaton, et al., 2000; Jeong, et al., 2018). There is additional complexity in the assessment of children’s mental health, with discrepancies between child and parent-report commonly cited (Bajeux, et al., 2018; Grills & Ollendick, 2003; Rothen, et al., 2009; Salback-Andrae, et al., 2009), suggesting that using comprehensive clinical assessments may be a more accurate way to gather data on psychopathology.
Being able to examine data collected from children who have experienced multiple risk factors and who are presenting with complex mental health difficulties in clinical practice would increase our understanding of the impact of cumulative childhood adversity in this highly vulnerable group. The present study used data gathered from a naturalistic, clinical sample of trauma-exposed children referred to a national and specialist National Health Service (NHS) clinic in the UK, to address the following aims: 1. To describe the mental health and functional impairment of this sample. 2. To describe the rates of risk exposure and rates of cumulative trauma in this sample. 3. To investigate associations between risk exposure, psychopathology, and functional impairment in this sample.
Method
Setting and participants
The present study took place at Great Ormond Street Hospital for Children, London. Participants were children who attended a specialist outpatient service for individuals presenting with complex psychological difficulties who have experienced historical trauma and adversity. Families attended the clinic for a multi-disciplinary assessment, which typically included assessments of the child’s developmental history, mental health, attachment, trauma history, and neurodevelopmental conditions.
As part of the induction into the service, families could opt in to give consent for their data to be used in retrospective research studies. For each family, a final assessment report was produced which included details of the child’s early history, trauma exposure, findings from standardised measures and any psychiatric diagnoses given. Information was gathered from a variety of sources, including parent/carer interview, child interview, social care referral notes, standardised measures, standardised clinical interviews, and observations.
Design
A retrospective approach was used, with data being collected from case records of families who had attended the clinic in the past six years. Data for each participant was collected at one time point and was as such cross-sectional.
Measures
All data used in the present study was gathered as part of routine clinical assessments. Information regarding risk exposure was gathered routinely on assessment via family interview and/or social care reports, or information given by the referring party. Psychiatric diagnoses were considered for every case seen in clinic, using all of the information gathered as part of the MDT assessment. This included a standardised interview (Development and Well-Being Assessment; DAWBA), clinical interviews, clinical observations, cognitive assessments, self-report measures, and data from referral notes, including social care reports in some cases. Decisions about diagnoses were made by the multi-disciplinary team and detailed in the final assessment report. Diagnoses fell into three distinct categories: depression, PTSD, and anxiety disorders. Demographic information was also gathered, as well as additional data regarding each child’s care status, age at which they were removed from birth family (where applicable), number of foster and adoption placements (where applicable).
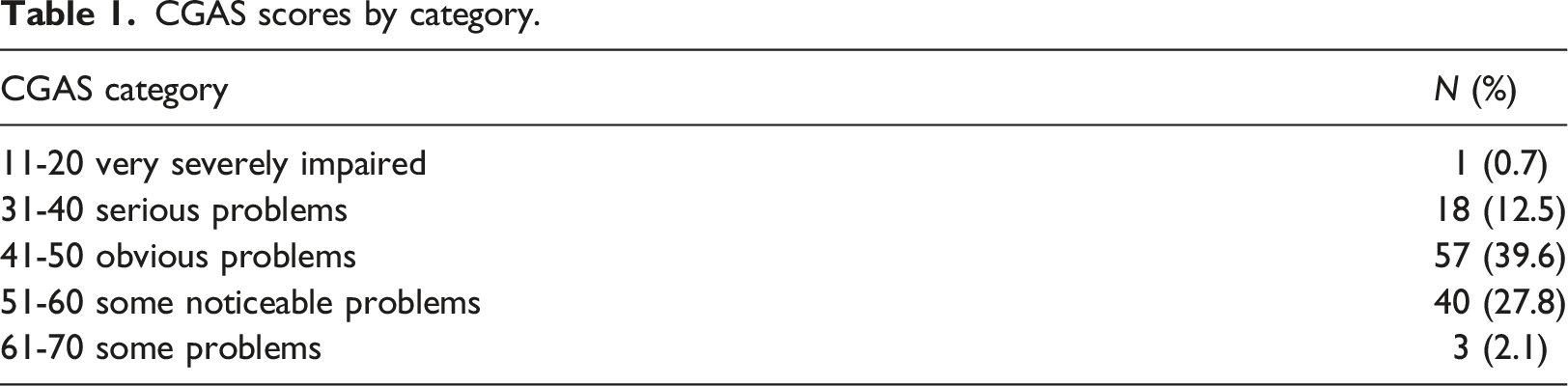
A child’s functioning was measured using the Children’s Global Assessment Scale (CGAS; Shaffer, et al., 1983). The CGAS is a clinician-rated estimate of current functioning in 6–17 year olds. A single score of 1–100 is given by assessing clinicians based on a range of criteria regarding the child’s psychological and social functioning. Scores are categorised with higher scores indicating better functioning, ranging from extremely impaired (score 1-10) to doing very well (score 91-100).
Procedure
Case records for all families attending clinic in the past six years were checked with those who did not give consent for data to be used in retrospective research excluded. Case records for the remaining cases were screened for relevant data. Data was collected from the assessment reports for each family, with additional information taken from the referral form and social care reports. Psychiatric diagnoses were made using ICD-10 criteria following the multi-disciplinary assessment using the range of data gathered within the assessment, and were detailed in the final assessment report. Information about trauma and risk exposure was gathered within the clinical assessment from family interviews or from social care reports, and was also detailed in the final assessment report, as were CGAS scores for each participant.
Analysis
The analyses were conducted in three phases. First, t-tests were used to determine if there were differences in the child’s age, their age when removed from birth family, and number of foster/adoption placements between those with/without anxiety, depression or PTSD. Second, gender differences on individual and cumulative risk were assessed using chi-square statistics. Third, three separate binary logistic regression models were used to predict diagnoses of anxiety, depression or PTSD. The predictor variable was cumulative risk exposure (1–5+) and the reference category. The results are reported as odds ratios.
Results
Demographic information
In total, data was collected for 132 participants. The mean age at assessment was 10.25 years (SD = 3.35; Range 4 – 17 years) and there were more males (n = 78, 59.1%) than females (n = 54, 40.9%). Most of the participants were adopted (n = 82, 62.6%) with the remaining living with their birth family (n = 19, 14.5%), in foster care (n = 15, 11.5%), Special Guardianship Order (n = 13, 9.9%), or in residential care (n = 2, 1.5%). The mean age when removed from birth family was 1.82 years (SD = 2.45; Range 0 – 10 years), and the mean number of foster/adoption placements was 2.49 (SD = 2.18; Range 0–19).
Rates of psychiatric diagnosis and levels of functioning
In total, 86 participants (65.2%) met criteria for at least one psychiatric diagnosis. There were no significant differences between males and females in the rates of anxiety (n = 40, 31.3%), depression (n = 10, 7.8%), or PTSD (n = 36, 28.1%).
The mean age of participants with a diagnosis of depression (M = 13.80 years, SD = 1.68) was significantly older than those without (M = 9.91 years, SD = 3.32; t(125) = 3.65, p < .001), but there were no significant difference in age when removed from birth family or number of foster/adoption placements. Those with a diagnosis of PTSD were removed from their family significantly later (M = 2.90 years, SD = 2.51) than those without PTSD (M = 1.42 years, SD = 2.33; t(107) = 2.90, p < .01), but there were no significant difference in age when removed from birth family or number of foster/adoption placements. Participants with and without a diagnosis of anxiety did not differ on age, age when removed from birth family or number of foster or adoption placements.
CGAS scores by category.
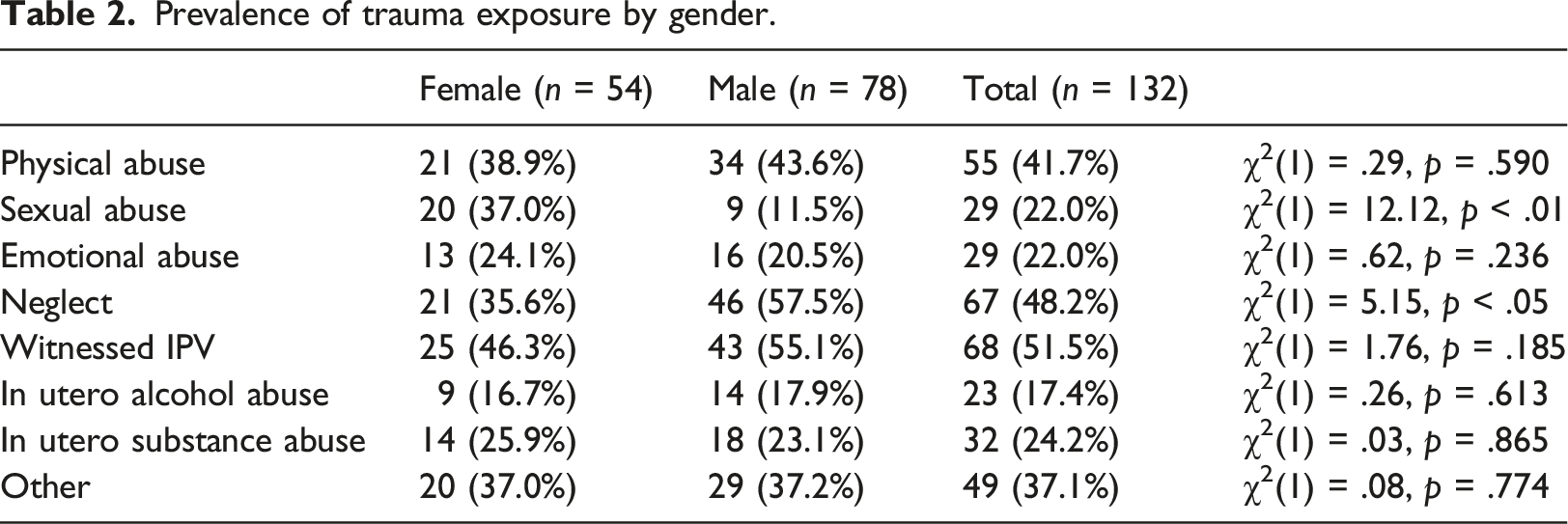
Rates of risk exposure
Prevalence of trauma exposure by gender.
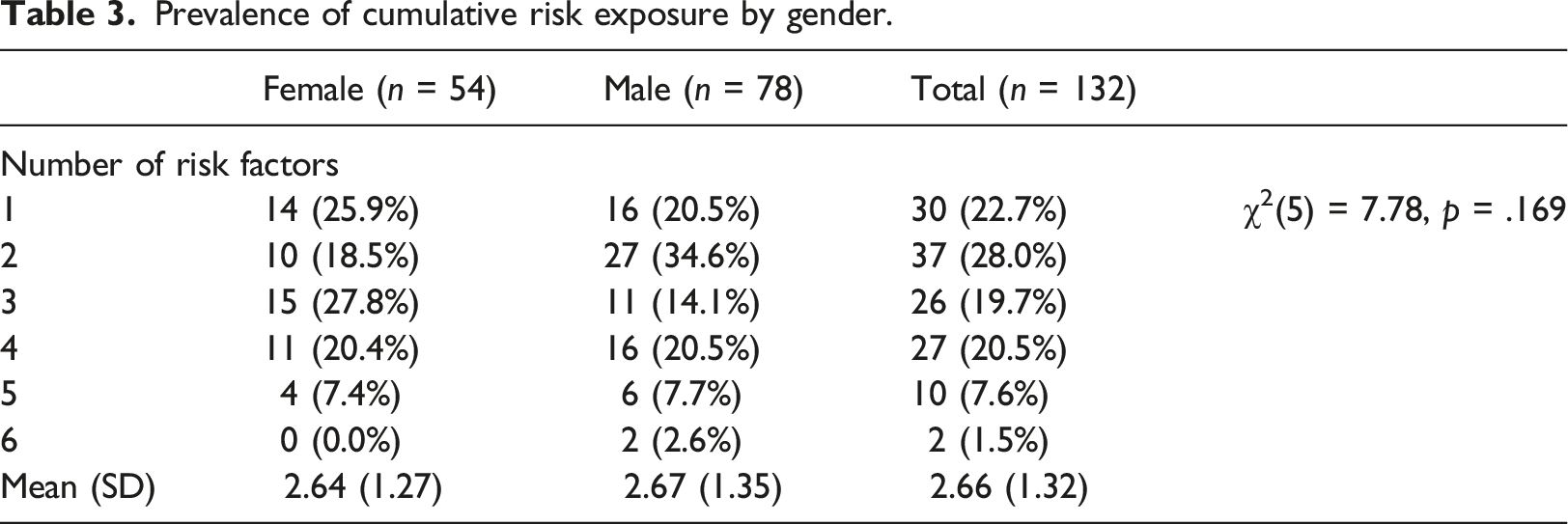
Prevalence of cumulative risk exposure by gender.
Associations between risk exposure, psychiatric diagnoses and functioning
Associations between cumulative risk exposure and anxiety, depression and PTSD.
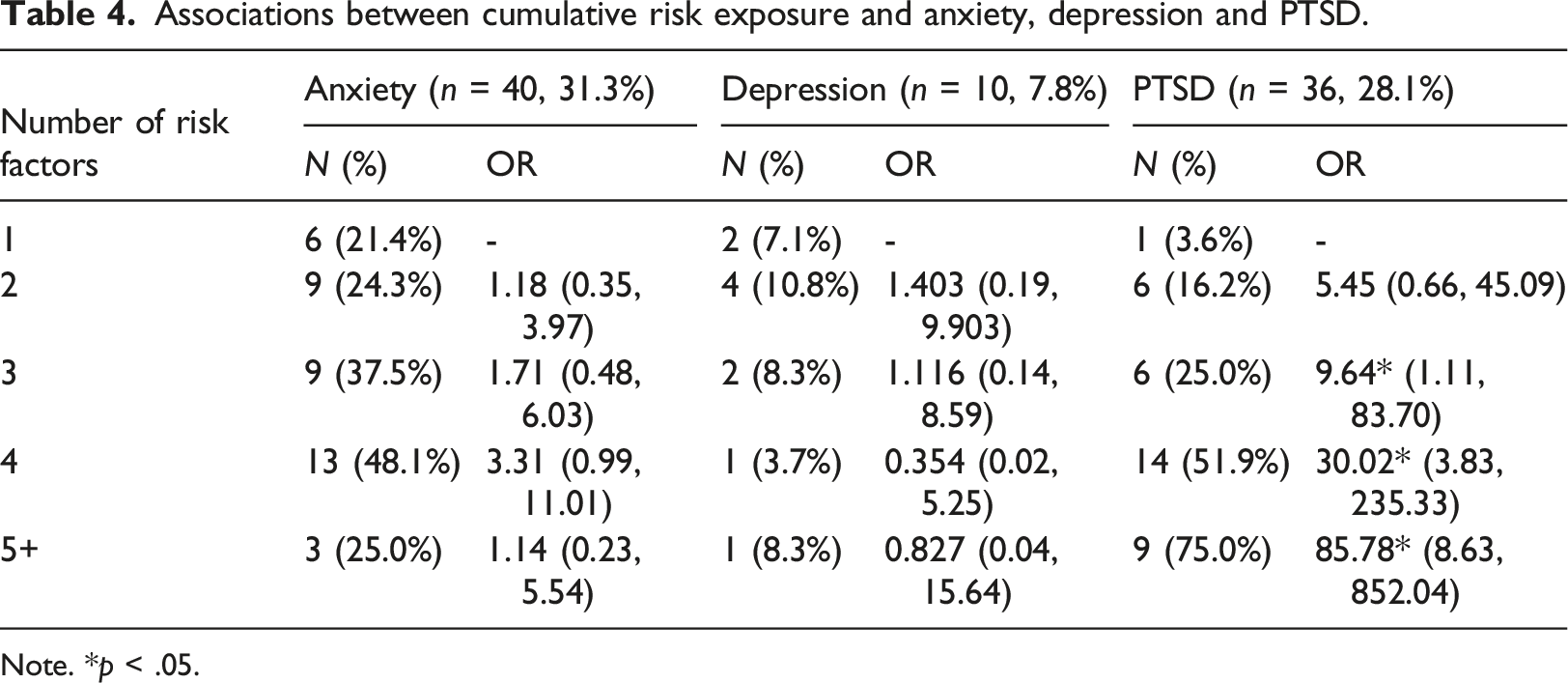
Note. *p < .05.
A one-way ANOVA was used to compare the effect of number of risk factors experienced on functioning as measured by the CGAS. Findings suggested there was not a statistically significant difference in functioning between participants experiencing different numbers of risk factors (F (4, 107) = .956, p = .435).
Discussion
The present study outlines one of very few investigations using a clinical sample of children who have experienced developmental trauma and been exposed to multiple risk factors. There are even fewer, if any, studies adopting this method of using data gathered from clinical assessments in childhood to assess the impact of trauma, risk and adversity, without relying on self-report measures.
The findings show that within this clinical sample, a high number of children (78%) had experienced multiple risk factors. The majority (65%) met criteria for at least one psychiatric diagnosis, most commonly anxiety disorders and PTSD, with those diagnosed with PTSD more likely to have been removed from birth family at an older age. Multiple risk exposure was associated with increased risk of PTSD, but not functional impairment or other psychiatric diagnoses. In terms of functional impairment, most participants (52%) fell into ‘obvious’ or ‘severe’ problems categories, suggesting significant functional impairment across the sample.
The present findings support existing literature which has found that multiple risk exposures increases the odds of psychiatric morbidity (Agorastos, et al., 2014; McKay et al., 2021; Shevlin et al., 2008). However, most existing research relies on self-report in adulthood. The current study suggests that the mental health impact following multiple risk exposures has its onset in childhood. Evidence from other countries supports this finding (Greeson et al., 2011).
In order to meet diagnostic criteria for PTSD, an individual must have been exposed to a traumatic event. The children in this sample are likely to have been at higher risk due to their relative trauma exposure. They may also have experienced trauma in social and family contexts that lacked protective factors and left them more vulnerable to developing PTSD and others morbidities, such as experiencing ongoing threat (prior to removal), being more likely to have family history of psychopathology (Knappe, et al., 2009; McLaughlin et al., 2012), increased chance of insecure or disorganised attachments (Hillman et al., 2020; McAuley & Young, 2006), or lack of social support (Harandi, et al., 2017). It is likely that those who had been removed from their birth family at a later age had been exposed to a higher number of traumas which would explain the higher rates of PTSD diagnosis in this group.
Regarding psychosocial functioning, findings from this study suggest that the children presenting in clinic had significant functional impairment, although level of functioning was not related to multiple risk exposure. Childhood functional impairment has been found to be an important predictor of psychosocial problems in childhood and early adulthood, such as psychiatric morbidity, suicide and criminality (Ellersgaard, et al., 2018; Lundh, et al., 2016). Notably, Lundh et al. (2016) found that children with CGAS scores up to 60 were most at risk for future adversity, and in the present study, only three children had scores higher than 60, suggesting that this is a highly vulnerable group.
The collective findings from the present study highlight the risks of cumulative risk exposure by underlining its associations with psychiatric morbidity. Children and young people experiencing anxiety, depression, PTSD, and functional impairment face an inevitable impact on their well-being and quality of life, and are also more likely to experience mental health and psychosocial difficulties in adulthood (Engqvist & Rydelius, 2006; 2007; McKay et al., 2021). This emphasises the importance of identifying at-risk children early in order to prevent multiple risk exposures as much as possible. Past research has suggested that only a small proportion of children with PTSD access formal support (Lewis et al., 2019). Demonstrating the impact of cumulative trauma in childhood also shows the importance of effective interventions for this at-risk group.
The findings have implications for clinical practice in demonstrating the importance of taking accurate histories on assessment to determine risk exposure. The findings suggest that where cumulative trauma exposure is observed, it would be important to assess for PTSD. This can be a challenging process in light of the complex presentation of difficulties commonly seen in children with multiple trauma histories (DeJong & Wilkinson, 2019). In cases of multiple trauma exposure, complex-PTSD is more likely to occur (Hyland, et al., 2017), which has implications for treatment. Current treatment guideline in the UK recommend trauma-focused CBT or EMDR for children and adolescents, but also advocate the involvement of families and carers (National Institute for Health and Care Excellence [NICE], 2017). However, guidelines for treating complex-PTSD in children are less well-defined, with some frameworks proposing a phased approach, incorporating stabilisation and emotion regulation work before commencing trauma-focused aspects of therapy (Blaustein & Kinniburgh, 2019; McFetridge, et al., 2017).
Limitations
The present study benefited from using clinical data from comprehensive MDT assessments in measuring the outcome variables, which added reliability and validity over and above self-report measures. The sample was also representative of children and families typically presenting to healthcare services where the child has experienced developmental trauma. However, the sample was not representative of the wider population and was, by definition of being referred to a specialist trauma service, limited to those who were experiencing trauma-related difficulties.
One of the major limitations of the study was its reliance on discrete, diagnostic categories to describe complex psychopathology and psychosocial phenomena in children. Diagnostic criteria are insufficient in their ability to convey the complexity of the needs of this vulnerable population experiencing multiple traumas and other risk factors. There are also uncertainties regarding the applicability to children of diagnoses mostly validated in adult populations. Future research ought to consider more sensitive analyses which can investigate with more sensitivity different symptoms and measures of dysfunction in this population, as well as considering the possible moderating effect of neurodevelopmental factors.
Future research is urgently needed to consider the applicability of diagnoses such as PTSD (including the new complex-PTSD category), depression, and anxiety, in child populations, including those who have multiple risk factors such as those in this study. This study raises the question of whether functional impairment is a more helpful frame of reference in this population. Additionally, many children in this sample were exposed to alcohol and substances in-utero, and future research is required to investigate the long-term impact of this exposure.
Conclusion
Rates of cumulative risk exposure were high in this sample. Experiencing multiple risk factors in childhood significantly increased the risk of developing childhood PTSD. The study highlights the rates of cumulative risk in this group of children as well as the rates of psychopathology and functional impairment. The findings demonstrate the importance of detailed and accurate clinical assessments in ascertaining trauma histories in children with known histories of adversity and maltreatment. This has important implications in the assessment and treatment of this population for practitioners in this field.
Footnotes
Acknowledgments
We would like to thank all families who agreed for their date to be used in retrospective research such as this project. We would also like to acknowledge the work of all members of staff past and present working in the Attachment and Trauma Team at Great Ormond Street Hospital.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.