
Abstract
Foster children are at risk for developing disorganized attachment relationships (Van den Dries et al., 2009; Vasileva & Petermann, 2018) and behavioural problems (Goemans et al., 2015; Vanschoonlandt et al., 2012). Video-feedback Intervention to promote Positive Parenting and Sensitive Discipline – Foster Care/Adoption (VIPP-FC/A) is an intervention aimed at improving sensitive parenting in order to promote secure attachment relations and reduce behavioural problems. In this study, a Randomized Controlled Trial (RCT) was used in order to examine the effectiveness of VIPP-FC/A in a Flemish foster care sample (n = 100), using questionnaires at three measurement moments. The hypothesis was that VIPP-FC/A would increase foster mothers’ sensitive parenting and decrease the externalizing behavioural problems and insecure attachment behaviour of the foster children and parenting stress of the foster mothers. The intervention effects on these four outcome variables were analysed by constructing four multilevel models. After controlling for the baseline measurement, there was no significant main effect of condition for sensitive parenting, externalizing problems, insecure attachment behaviour and parenting stress. There was however a significant effect of condition and age on insecure attachment behaviour: within the group of youngest foster children (under 30 months), children in the intervention group scored lower insecure attachment scores than children in the control group. Additionally, there was a significant effect of condition and type of foster care on externalizing behaviour problems. In the group of children placed in kinship foster care, children in the intervention group had lower external behavior scores than children in the control group.
Introduction
Foster care for young flemish foster children
Out-of-home care is indicated when the safety, development and/or well-being of children are endangered in a profound way, or when parents cannot take the responsibility to raise their children (Pecora et al., 2009; Van den Bruel & Stroobants, 2016). Family foster care is considered the first option of choice when an out-of-home placement is needed in Flanders, the Dutch speaking part of Belgium (Van den Bruel, 2012). This need for family foster care is even more stressed for the youngest group (0–6 year) of children in need of an out-of-home placement (Van den Bruel & Stroobants, 2016), as a family like home environment supports the child to develop optimally (De Baat & De Lange, 2013). Young children make up a significant part of the new foster placements in Flanders, as 36% of the foster children were under six years old when placed in foster care (Pleegzorg Vlaanderen, 2020).
Flanders has five foster care agencies, each for one province (Van den Bruel, 2012), responsible for the recruitment and screening of foster carers, matching and monitoring the placement. There are different types of foster care: supporting, short-term, long-term and treatment foster care. Supporting foster care aims at offering a short-term break or a part-time stay (e.g. weekends or holidays) in order to support the family, or offers short-term emergency care. Short-term foster care has a maximum duration of 1.5 year, during which intensive efforts are made to improve the family’s situation. If reunification is impossible, a long term out-of -home placement needs to be considered. Long-term foster care creates permanency and continuity for the foster child, although a return home can be considered at any given moment. As adoption after a foster care placement is extremely rare in Flanders, children can be placed in foster care until adulthood. During treatment foster care, the foster child, foster parents and/or parents are given additional treatment and support (Van den Bruel, 2012).
Besides these different types of foster care, kinship and non-kinship care can also be distinguished. Kinship care are placements in the broader family or social network, 72% of all Flemish placements are currently kinship families (Pleegzorg Vlaanderen, 2020).
The need for interventions in foster care
According to the most recent numbers, 9,914 children are living in Flemish foster families (Agentschap Opgroeien, 2022). These children often experienced adversities, putting them at risk for problematic outcomes (Juffer, 2010). Research has shown similar rates of secure attachment relationships between foster children and their foster carers when these were compared to results of research in the regular population, but foster children were found to be more likely to have disorganized attachment relationships (van den Dries et al., 2009; Vasileva & Petermann, 2018). Insecure disorganized attachment is considered the least desirable attachment style, as it is associated with difficulties in dealing with stress, externalizing behavioral problems and psychopathology in later life (Van Ijzendoorn et al., 1999). A secure attachment relationship between children and their attachment figures has a positive effect on the overall development (Van IJzendoorn, 2008) and lowers the chances of foster placement breakdown (Strijker et al., 2008).
Additionally, foster children have more behavioural problems than children of the general population (Goemans et al., 2015; Vanschoonlandt, Vanderfaeillie, van Holen, et al., 2012). Longitudinal Flemish research found problem behaviour to have a direct negative impact on parenting behaviour, leading to less supportive parenting and more negative control (Vanderfaeillie et al., 2012). Behavior problems are associated with breakdown (Leathers, 2006).
Foster caregivers experience more parenting stress than parents of the general population (Bastiaensen, 2001). Neece et al. (2012) found evidence for a bidirectional relationship between parenting stress and child behavior problems in the general population. In the foster care population, research also shows an association between behavior problems and parenting stress (Goemans et al., 2018; Perry, 2015). Parenting stress has a negative impact on foster caregivers' parenting behaviors (i.e., decreased support and increased negative control). Consequently, parenting stress is therefore identified as a threat to the foster care placement (Bastiaensen, 2001; van Oijen, 2010; Vanderfaeillie et al., 2012; Vanderfaeillie & Van Holen, 2010; Vanschoonlandt et al., 2013; Wilson et al., 2004).
Foster children are at risk for developing disorganized attachment (van den Dries et al., 2009) and behaviour problems (Vanschoonlandt, Vanderfaeillie, van Holen, et al., 2012), their foster parents are at risk for higher levels of parenting stress (Bastiaensen, 2001). Sensitive parenting and sensitive disciplining are negatively associated with insecure attachment relations and behavior problems (Vanderfaeillie et al., 2013; West et al., 2020), so interventions are needed to promote sensitive parenting and sensitive disciplining. Early interventions are the best and most inexpensive interventions (Allen, 2011).
In response to the aforementioned challenges, various parenting interventions employing video feedback have been developed with the aim of enhancing parental sensitivity and promoting secure attachment in foster care settings. The Foster Carer-Foster Child Intervention (FFI; van Andel, et al., 2012) is a Dutch program that combines psychoeducation and video feedback. It focuses on reducing stress in foster children by bolstering the emotional availability, parenting skills, and confidence of caregivers. An RCT assessment notably positive effects on parenting skills and the responsiveness of foster children. However, there were no significant differences in stress levels for either caregivers or children (van Andel, et al., 2012).
Among the most widely recognized video-feedback interventions for foster caregivers is Attachment and Biobehavioral Catch-up (Dozier, 2013). Research has demonstrated its effectiveness in enhancing foster caregiver sensitivity (Bick & Dozier, 2013), reducing parental stress (Sprang, 2009), reducing children’s behavioral issues (Dozier, et al., 2006; Sprang, 2009), improving their executive functioning capabilities (Lind, et al., 2017), and reducing diurnal cortisol slopes (Dozier, et al., 2006) as well as avoidant attachment behavior (Dozier, et al., 2009).
Promoting First Relationships (Kelly et al., 2008), is an infant mental health training program that incorporates reflective video feedback. The objective is to improve caregiver sensitivity and understanding of children’s difficult behaviour to enable them to become more secure and behaviourally regulated. In a sample involving foster care, it has been demonstrated to be effective in improving caregivers' sensitivity and understanding of toddlers’ social-emotional needs, ultimately resulting in increased child competence. Nevertheless, there were no enduring post-intervention effects on attachment outcomes (Spieker, et al., 2012).
Video-feedback intervention to promote positive parenting for foster children
Video-feedback Intervention to promote Positive Parenting (VIPP) is an intervention based on Bowlby’s (1969) attachment theory and aims at increasing the sensitivity of caregivers and promote positive child–carer interactions (Juffer et al., 2017a). During the sessions, parent–child interactions are recorded, viewed and discussed with the parents (Juffer et al., 2017b).
VIPP is used for families with infants up to the first birthday. For older children (between one and six), Video-feedback Intervention to promote Positive Parenting and Sensitive Discipline (VIPP-SD) was developed. Additions were added to VIPP-SD to work on the discipline strategies of parents in dealing with difficult child behaviour (Juffer et al., 2017a).
A variant of VIPP-SD for foster children was developed, VIPP-FC/A, by adding two elements to make VIPP-SD more relevant to foster care and adoption situation (FC/A) (Schoemaker et al., 2020). The first was a focus on sensitive bodily contact, in order to promote a secure attachment (Duhn, 2010) and support the stress regulation of both foster parents and foster children (Schoemaker et al., 2018). The second element concerned foster care-specific behaviour of foster children, as foster children often learned to hide their feelings and needs. Their avoidance of proximity and pushing foster parents away can make it more difficult for carers to build a relationship with them (Stovall-McClough & Dozier, 2004). In VIPP-FC/A, foster parents’ attention is drawn to the subtle signals that their foster child gives and ways of responding appropriately to these signals.
The effectiveness of VIPP-FC/A was examined in three studies. The first two examined a sample of Italian mothers and their internationally adopted children, there is a partial database overlap between them. In Barone et al. (2018) (n = 80), VIPP-FC/A was associated with increased emotional availability of the children to their mothers (r = .46) and higher levels of maternal positive parenting (r = .39). In the second study, Barone et al. (2019) (n = 83) found increased sensitivity among mothers in a six-month follow-up of the intervention group (b = 83, p = .001), which contributed to higher levels of emotional availability and decreased externalizing behavioural problems among the children (b = .55, p = .001, b = 2.64, p = .001). The third study involved Dutch foster mothers and their foster children (n = 60). Schoemaker, Juffer, et al. (2020) found no evidence that VIPP-FC/A was effective in improving foster carers’ sensitive parenting or positive attitudes, the researchers suggested that the findings could be explained by a selection bias and subsequent ceiling effect.
The foster parents in their sample generally had high scores of parental sensitivity, sensitive discipline, and parenting attitudes at the pretest, leaving limited room for enhancement. Furthermore, the authors state that there might also be a selection bias at play: the foster families that could have taken advantage the most benefit from a parenting intervention might not have been part of the study sample.
Research question
VIPP-SD has proven to be effective at improving different outcome variables. Juffer, Bakermans-Kranenberg, and van IJzendoorn (2018) conducted a meta-analysis on VIPP(SD), examining 12 randomized controlled trials (RCTs). The overall effect size in the meta-analysis for sensitivity was d = .47, and for attachment, it was d = .36. The combined effect size for improved child outcomes was d = .37, and for reduced child problem behavior, d = .26. Van IJzendoorn et al. (2023) conducted a series of meta-analyses of 25 randomized controlled trials testing the VIPP-SD method. They found combined effect sizes on parenting behavior (d = .37) and attitudes (d = .32), and on child attachment security (d = .47), but not on child externalizing behaviour problems (d = .14).
However, the results on the variant for foster care and adoptive situations are less clear and there-are no studies regarding VIPP-SD, nor VIPP-FC/A in Flanders. The hypothesis was that VIPP-FC/A increases foster mothers’ sensitive parenting and decreases the externalizing behavioural problems and insecure attachment behaviour of foster children and parenting stress of the foster mothers.
Methods
Participants
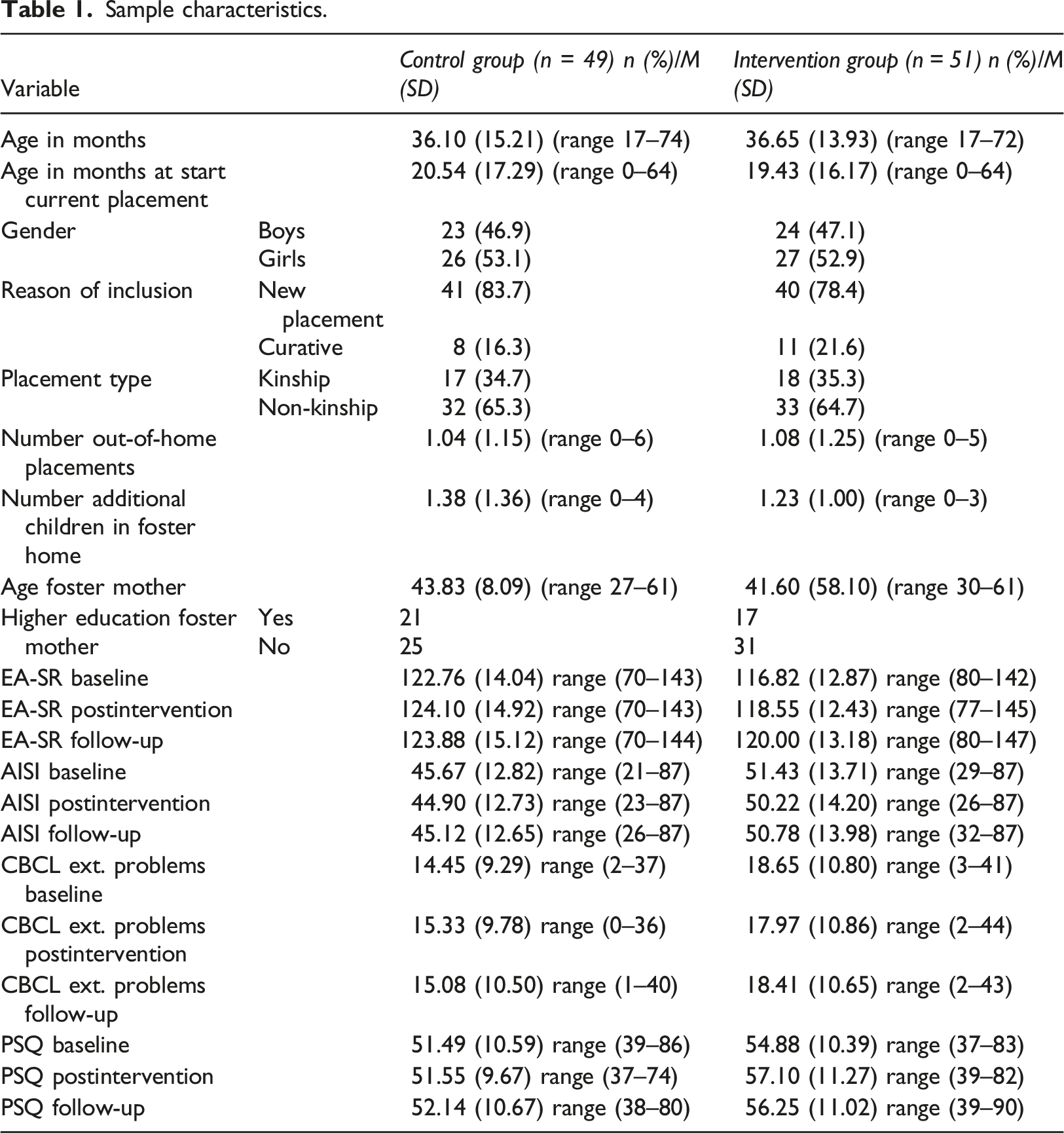
Sample characteristics.
Procedure
All five Flemish foster care agencies agreed to participate to this study. They provided information of the study to the eligible families and returned the informed consents of the participating foster mothers.
Inclusion criteria were: - A foster child between 17 months and six years old at time of inclusion - The foster child was placed in the foster family in the past year (new placements) - It was also possible to be included in the study when the children were already residing in the family for more than one year, when the families or the foster care workers assesses the risk for attachment, parenting or behaviour problems as high (curative) - Placements had to be long-term, children in supporting and short-term foster care were excluded - Foster children had no known cognitive disability, severe motor disability or ASS - Foster mothers had to be able to read Dutch (criterium: ‘able to read and understand a Dutch paper’)
When more than one foster child from the same foster family was eligible, the youngest child was included. Twins were excluded from the study.
After collecting an informed consent, foster care workers filled in a questionnaire regarding characteristics related to the foster child, foster care placement, case history, parents and foster parents (Vanschoonlandt et al., 2012). Foster mothers filled out questionnaires at baseline (T0), postintervention (5 months later; T1) and at follow-up (2 months after T1; T2). All families allocated to the control group were offered the intervention after completing the follow-up questionnaires. The first author sent out the questionnaires by email, families that struggled to answer digitally received the questionnaires by mail. All procedures were approved by the boards of the foster care agencies and by the ethical board of [blinded for review].
The study was designed as a RCT. The control group received treatment as usual. They were offered the care that participants in the control group would typically receive by the foster care workers, including interventions, if they were not enrolled in the trial. To achieve equal distribution between the intervention and control group, randomization by minimization was used. We wanted to ensure that both intervention and control group were comparable on different meaningful characteristics, especially because our sample size was rather small. This approach aims to obtain two comparable groups in terms of gender and age of the foster child (<2.5 years/>2.5 years), reason for inclusion in the study (new placement/curative), type of foster placement (kinship/nonkinship) and previous out-of-home placements (none/at least one), ensuring balanced participant numbers and characteristics across both groups (Taves, 2010). When a child was eligible for this study, the randomization was carried out by the first author. Allocations to the intervention or control groups were done using MinimPy Program .3 (Saghaei & Saghaei, 2011). MinimPy Program .3 is an open-source minimization program that was written in Python programming language. Initially, the first participants are randomly assigned to one of the groups. For subsequent participants, the allocation occurs following a hypothetical assignment to each group, followed by the calculation of an imbalance score. Based on these imbalance scores, the program decides to which group the new participant should be assigned to, with the goal of minimizing the disparity in prognostic factors (Saghaei & Saghaei, 2011).
We included various child and foster care placement characteristics in the randomization with minimization and subsequent analyses because, based on literature, we expected that these characteristics could potentially have an effect on the level externalizing behaviour problems, the quality attachment and/or the effectivity of the intervention. The first characteristic is the gender of the foster children, since in the general population boys exhibit more externalizing behavior problems than girls (Bongers et al., 2003; Inchley et al., 2020). Additionally, some researchers found girls more likely to be securely attached to their foster parents than boys shortly after the placement started (Gabler et al., 2014; Lang et al., 2016). The second factor was the age of the foster children, because in the general population externalizing behaviour problems decrease with age (Bongers et al., 2003).The results according age and externalizing behaviour problems are inconsistent in foster care research (West et al., 2023). Regarding attachment, some research points to younger children having more often a secure attachment shortly after start of the placement (Lang et al., 2016; Ponciano, 2010). Reason for inclusion in the RCT was decided because children who are enrolled in the study because of curative reasons will on average experience more difficulties than regular starting foster care placements. The fourth factor is type of foster care. Kinship foster carers are more often vulnerable because they are older, have more health issues, have a lower educational level, lower income, receive less support and experience more parenting stress (Fuentes-Peláez et al., 2014). In international research, children in kinship foster care have fewer behavioural problems (Holtan et al., 2005; Keller et al., 2001), these differences are not found in Flemish and Dutch research or wereby other variables such as the number of previous placements (Bastiaensen, 2001; Strijker et al., 2003; Strijker & Van Oijen, 2006; Vanschoonlandt, Vanderfaeillie, Van Holen, et al., 2012). The last factor was previous out-of-home placements, because replacements have negative consequences for foster children (Pecora et al., 2009; Van den Bergh & Weterings, 2010; Van Holen et al., 2012). For example, it was found that relocation can increase the behavioural problems of foster children (Herrenkohl et al., 2003; Newton et al., 2000). The maternal educational level was the only factor that was used in the analyses, but was not included in the randomization with minimization. Some researchers showed that parenting interventions can be especially advantageous for mothers with limited education (Mendelsohn et al., 2007). Klein Velderman et al. (2006) point out that parenting information is less available to mothers with a low education, making them interesting candidates for the VIPP-SD intervention
Instruments
Emotional availability–Self report
The Dutch version of the Emotional Availability–Self Report (EA-SR) was used to measure the self-reported parental sensitivity of the foster mothers (Vliegen et al., 2005). The EA-SR is made out of 32 items scored on a 5-point scale (1 = completely disagree, 5 = completely agree). The results of the scores on these 32 items can be grouped into five subscales: affective attunement (mutual factor), parental involvement (child factor), affective quality (mutual factor), intrusiveness (parental factor), and hostility (parental factor), and a total score (Vliegen et al., 2005). The Cronbach alpha coefficient of the total scale was α = .85 in this study.
Attachment insecurity screening inventory 2–5 years
The Attachment Insecurity Screening Inventory 2–5 years (AISI 2–5 years, (Polderman & Kellaert-Knoll, 2008; Wissink et al., 2016) is a questionnaire measuring insecure attachment between caregiver and the child. It contains 20 questions scored on a 6-point scale ranging from never (1) to always (6), in this study scored by the foster mothers. Items can be grouped in three subscales, but only the AISI total insecurity scale was used in this study. Higher scores indicate more attachment insecurity, total scores of 50 and higher are considered clinical. Convergent validity was supported by negative associations with observed attachment security measured with the Attachment Q-Sort (AQS, Waters & Deane, 1985) and total scores on the AISI. The AISI total score discriminates between children with a secure and insecure attachment with their caregivers measured with the AQS, with an AUC-value for mothers of .91 (Wissink et al., 2016). The Cronbach alpha coefficient for the AISI total insecurity scale in current study was α = .72.
We only used the total insecurity scale, as only that scale was used to examine the convergent validity (Wissink et al., 2016). The decision to use the AISI instead of the Strange Situation Procedure (SSP) was based on the reasons for using questionnaires mentioned before. Additionally, the RCT involved repeated measures, with only a two-month gap between the second and third measurements. Using the SSP with such a short time gap could sensitize the children to the procedure.
Parenting Stress Questionnaire
The Dutch version of the Parenting Stress Questionnaire (PSQ, Vermulst et al., 2012) was used to measure parenting stress of foster mothers. The PSQ contains 34 questions scored on a 4-point scale, ranging from (1) not true to (4) very true. Five subscales can be calculated, but only the total scores were used in this study. Higher scores on the PSQ represent higher perceived levels of parenting stress. T-scores under 60 are considered non-clinical, scores between 60 and 63 subclinical and scores of 64 and higher clinical. In this study, the Cronbach alpha coefficient of the total parenting stress scale (over 34 questions) was α = .92. The validity of the PSQ is good (Vermulst et al., 2012).
Child behavior checklist 1,5–5
Behaviour problems of the foster children were quantified using the Dutch translation of the Child Behaviour Checklist (CBCL; (Achenbach & Rescorla, 2000; Verhulst & van der Ende, 2000). The CBCL contains 99 statements regarding behaviour of the child scored by the foster parent on a 3-point scale. The questionnaire provides scores for three broad-band scales: internalizing, externalizing and total problems (Achenbach & Rescorla, 2000). Subclinical scores are scores between 60 and 63, clinical scores are 64 and above. In this study, the internalizing subscale has a Cronbach’s Alpha of α = .93, the Cronbach’s Alpha for the externalizing subscale is α = .87 and for the total score it is α = .96. The validity of the CBCL is considered good (Achenbach & Rescorla, 2000). Only the externalizing problems subscale was used in this study.
VIPP-FC/A intervention
VIPP-FC/A is implemented with one foster (or adoptive) parent and a child in the family’s own home. At the start of each of the seven VIPP-FC/A sessions, short video-recordings are made in which care taker and child are asked to interact as usual during daily situations. These recordings are then viewed by the foster parents and a VIPP-FC/A practitioner, giving micro-feedback to the foster carer. In the first two sessions, the feedback is formulated from the foster child’s perspective. In sessions three and four, focus is on parental sensitivity. The last two sessions are used to review what has been learned. General information about child development is given in all the sessions.
VIPP-FC/A practitioners are foster care workers that had a four days training and did a supervised test VIPP-FC/A intervention. In this study, 16 trained foster care workers delivered the VIPP-FC/A interventions. Each had a degree (bachelor’s or master’s) in social work, psychology or pedagogy. The families receives the whole intervention including seven sessions.
Data analysis
A priori power analysis showed that a sample of 98 foster families resulted in an adequate statistical power (.81; Repeated measures ANOVA within-between interaction, G*Power 3.1.9.7) (Faul et al., 2009), based on an effect size f of .13, two groups, a repeated measures design with three measurement points, and an α = .05. The effect size f = .13 was based on the meta-analytic results of Juffer et al. (2018), who found the smallest effect size of VIPP-SD was the combined effect size for reduced behaviour problems (d = .26).
Data were analysed using Intention-to-treat analysis, which involves analyzing participants based on their initial group assignments. By employing this analysis method, the prognostic balance achieved through randomization is maintained (McCoy, 2017). Figure 1 gives an overview of the occurrence of missing data. The pattern of missingness was explored using a missing data dummy code (missing value = 0, non-missing value = 1) (Cohen & Cohen, 1983). This dummy code was used in t-tests and χ2-tests with the other variables. Results show that gender of the foster childer was significantly associated with the dummy code. That is data of boys was more often missing (χ2 (1) = 8.47, p = .004). In addition to the efforts done to minimize missing data, ‘Last Observation Carried Forward’ method (LOCF) was used. LOCF is a common statistical approach for analysing longitudinal repeated measures data with missing observations (Whittaker et al., 2006). In a LOCF-analysis, a missing value is replaced by that subject’s previously observed value, meaning the last observation is carried forward. The combined dataset, consisting of observed and imputed data, is then analysed as if there were no missing data present. There has been some criticism on the use of LOCF and in literature it is stated that it should be used with caution (Whittaker et al., 2006). Using LOCF is however a more conservative method than running a multiple imputation algorithm to deal with these missing data (O’Neill & Temple, 2012). It was preferred over running a multiple imputation algorithm in this study because of this more conservative approach, we were cautious not to overestimate a possible treatment effect. LOCF was applied to 16 families at T1 and 29 families at T2. 100 families were included in the analyses after LOCF. Overview of participants.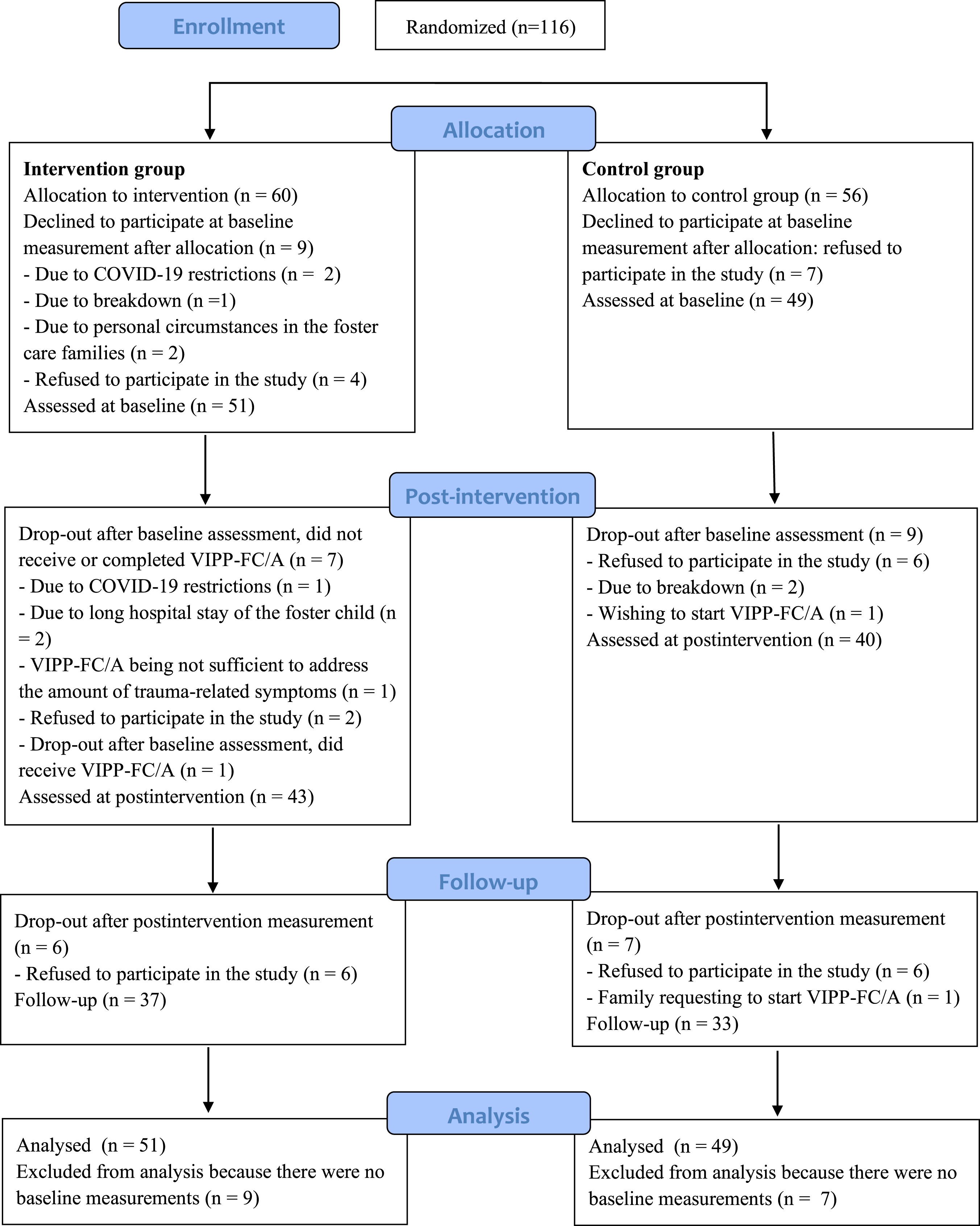
Demographic background variables and baseline outcomes of the intervention and control group were compared using t-tests and χ2-tests.
The intervention effects of VIPP-FC/A on sensitive parenting (EA-SR), insecure attachment behavior (AISI), behavior problems (CBCL) and parenting stress (PSQ) were analyzed by constructing 4 multilevel models, one for each outcome variable. Because of the baseline differences for EA-SR, AISI and CBCL between intervention- and control group, all models were constructed as longitudinal covariance analysis models (Lydersen, 2022; Twisk, 2021). The baseline measurements were added as independent variables instead of as parts of the outcome variables (Lydersen, 2022; Twisk, 2021), thus only the post-intervention (T1) and follow-up (T2) data were included as dependent variables.
Note that using multilevel modelling, a distinction is made between level 1 and level 2 predictor variables. In current study, the level 1 variables are Time (T1 = post-intervention, T2 = follow-up) and the baseline measurements of the outcome variable. The level 2 explanatory predictor variables are condition (intervention, control group), reason for inclusion (new foster care placement or foster parents/social workers requesting VIPP-FC/A for curative reasons), age (younger or older than 30 months), duration of current placement (continuous variable), placement type (kinship, non-kinship), gender of the foster children (male of female), previous placements of the foster children (yes, no) and higher education of the foster mother (yes: holding a college or university degree or no).
A stepwise, bottom-up model building approach was adopted (Hox et al., 2018). The first model was the intercept-only model (M0), which gives a benchmark value of the deviance. In the second model (M1), the level 1 explanatory variables were added (i.e., Time and the baseline values). In the third model (M2), the level 2 explanatory variables and cross-level interactions were added. Fourthly, we assessed if the slopes of the level 1 variables have a significant variance component between groups in the random coefficient model (M3). No evidence was found for the presence random slopes.
At each step, variables were added to the model on a variable-by-variable basis with an alpha-to-enter of .05. Variables that became unsignificant were removed from the model (alpha-to-remove = .10). Because of its theoretical importance, the main effects of Time and Condition and the two-way interaction of Time and Condition were always kept in the model. Model improvement at the end of each step was assessed using AIC values. For all models, the intraclass correlation (ICC) is computed.
All model assumptions were met. A p-value below .05 was considered significant. Analyses were performed in R version 4.3.0, using the lme4 (Bates et al., 2009), lmerTest (Kuznetsova et al., 2017) and car (Fox et al., 2023) packages. The figures were generated using sjPlot (Lüdecke et al., 2023).
Results
Baseline differences
Despite the design using minimization to randomly assign and balance participants’ characteristics across control and intervention groups, there were significant differences for three outcome variables at the baseline measurement. The scores of the EA-SR were higher in the control group (M = 122.76, SD = 14.04) than in the intervention group (M = 116.82, SD = 12.87), t (98) = 2.20, p = .030. For the externalizing problem scale of the CBCL, the scores were higher in the intervention group (M = 18.65, SD = 10.80) than in te control group (M = 14.45, SD = 9.29), t (98) = 2.08, p = .040. The scores on the AISI were higher in the intervention group (M = 51.43, SD = 13.71) than in the control group (M = 54.67, SD = 12.82), t (98) = −2.17, p = .033. This indicates more external problems and insecure attachment behavior in the intervention group than in the control group, and higher sensitive parenting in the control group. There were no significant differences between PSQ-scores of the control (M = 51.49, SD = 10.59) and intervention group (M = 54.88, SD = 10.39) at baseline, t (98) = −1.60, p = .113. Because of the baseline differences for EA-SR, AISI and CBCL between intervention- and control group, baseline imbalances were adjusted for by constructing the models as longitudinal covariance analysis models (Lydersen, 2022; Twisk, 2021). Although there were no significant differences for the baseline PSQ-scores, the model was also constructed as longitudinal covariance analysis model to promote consistency, and because the PSQ was scored by foster mothers of the same sample where there are clearly significant differences between both condition on several variables.
Intervention effects of VIPP-FC/A
Multilevel mixed models were constructed to assess the intervention effects for each dependent variable. More details on the model building process for each multilevel model can be found in Appendix 1.
Sensitive parenting behavior
Final multilevel models for EA-SR, AISI, CBCL external problems and PSQ as dependent variables.
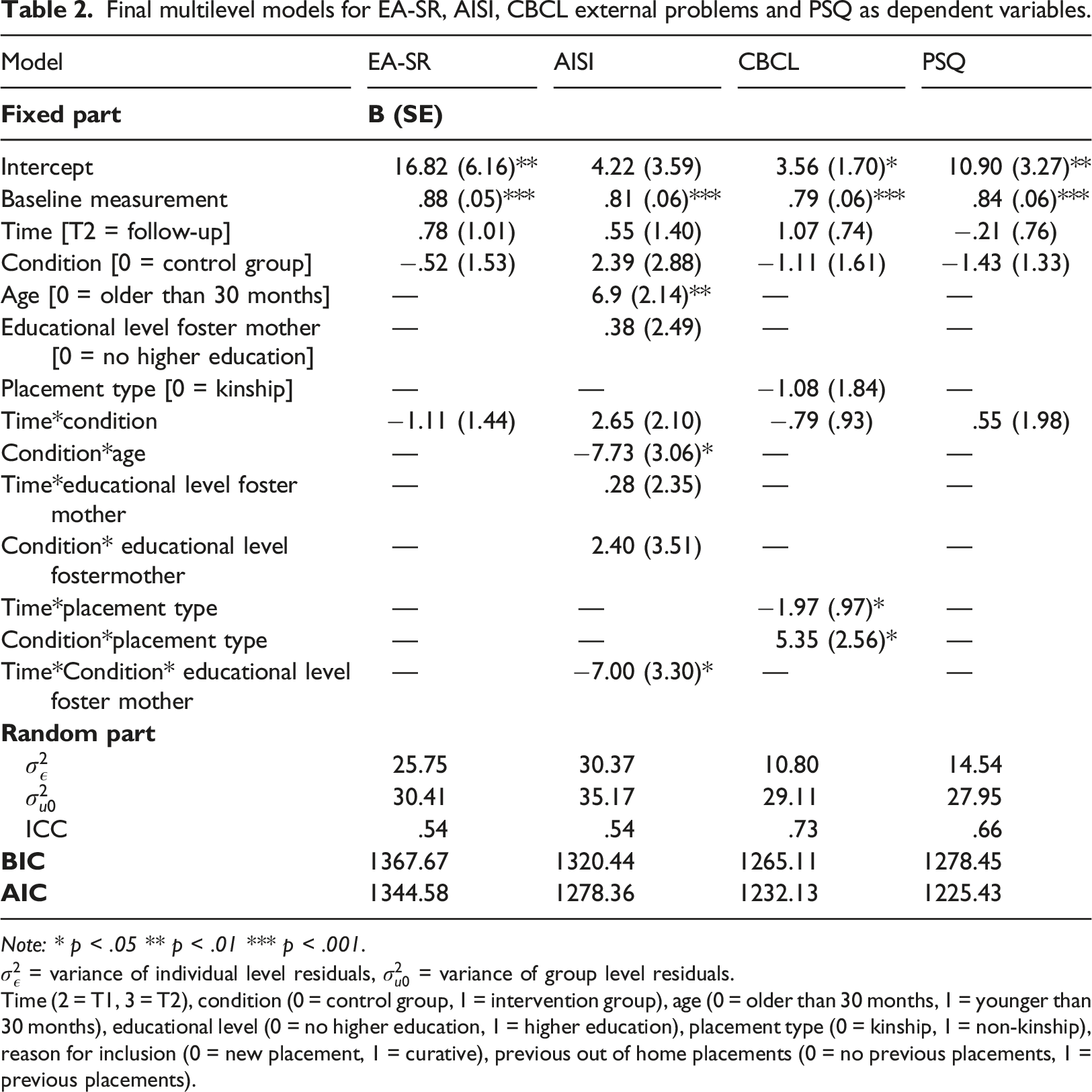
Note: * p < .05 ** p < .01 *** p < .001.
Insecure attachment behaviour
Based on the information presented in Table 2, there was no significant effect of time (
There was no significant effect of condition ( Predicted values of AISI for age and condition.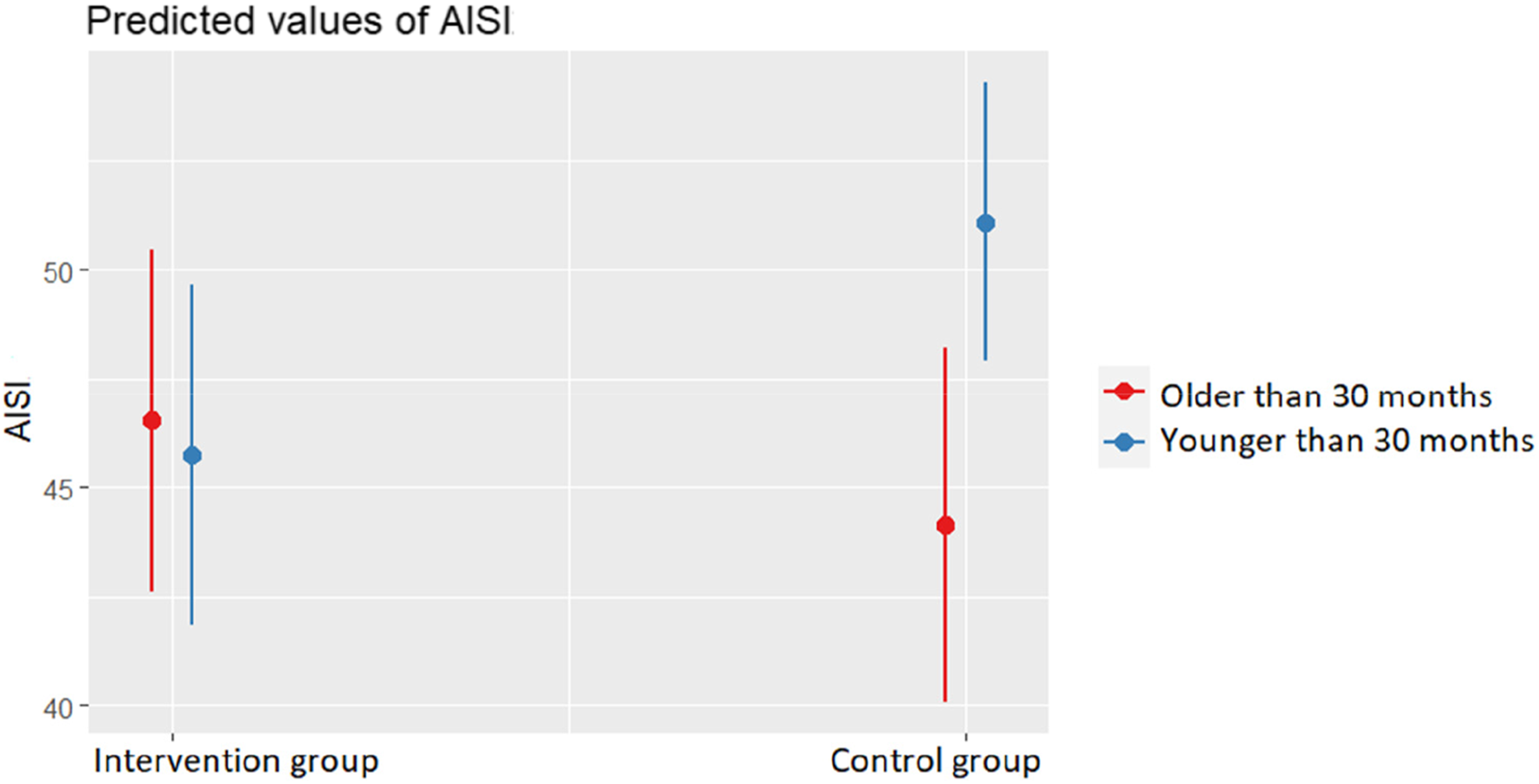
Additionally, Figure 3 shows a significant three-way interaction of condition, time and educational level ( Predicted levels of AISI for time, condition and educational level.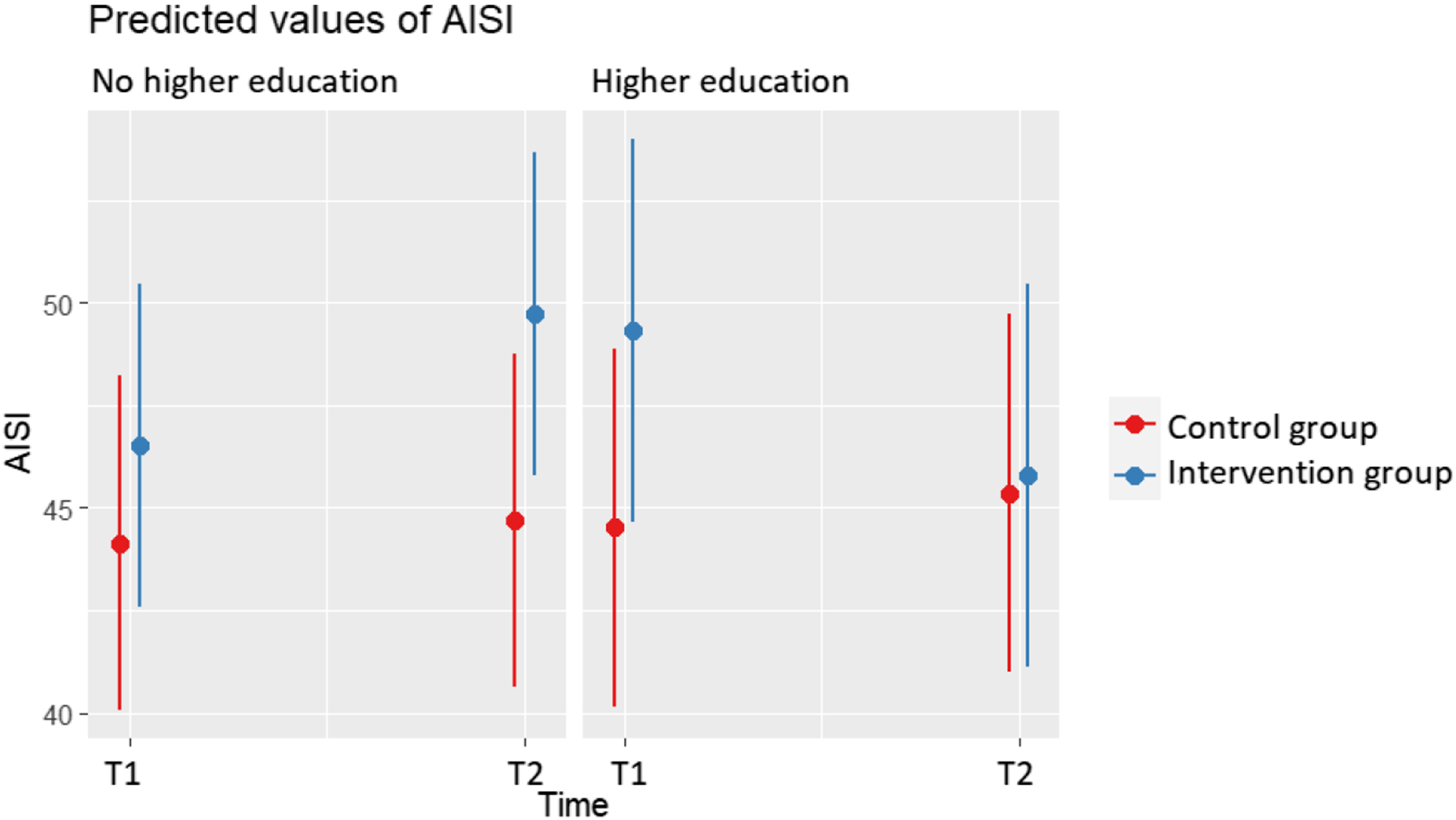
Externalizing behaviour problems
The baseline score was predictive for externalizing behavior scores ( Predicted values for CBCL with time and type of foster care.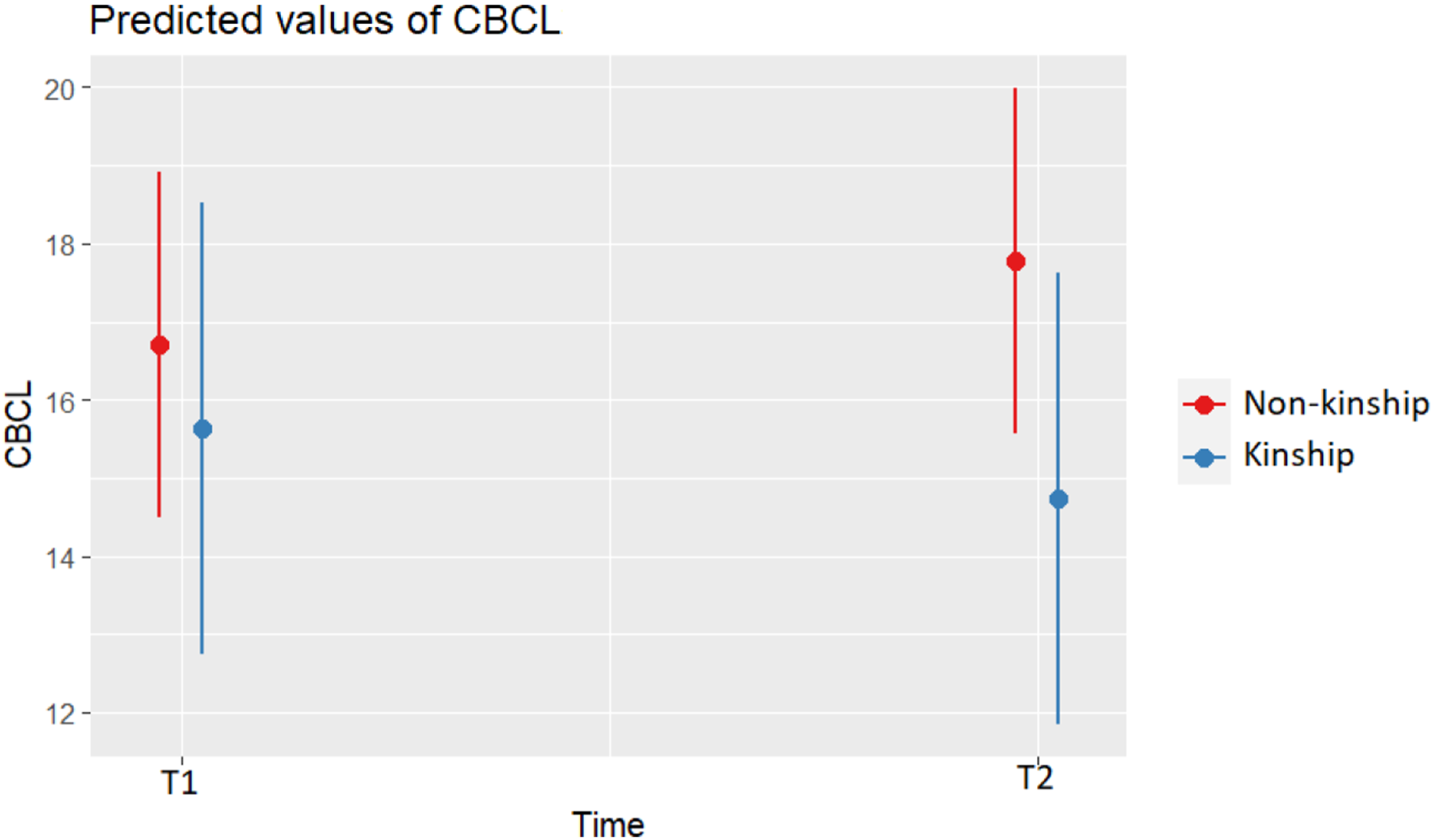
There was no significant effect of condition ( Predicted values for CBCL with condition and type of foster care.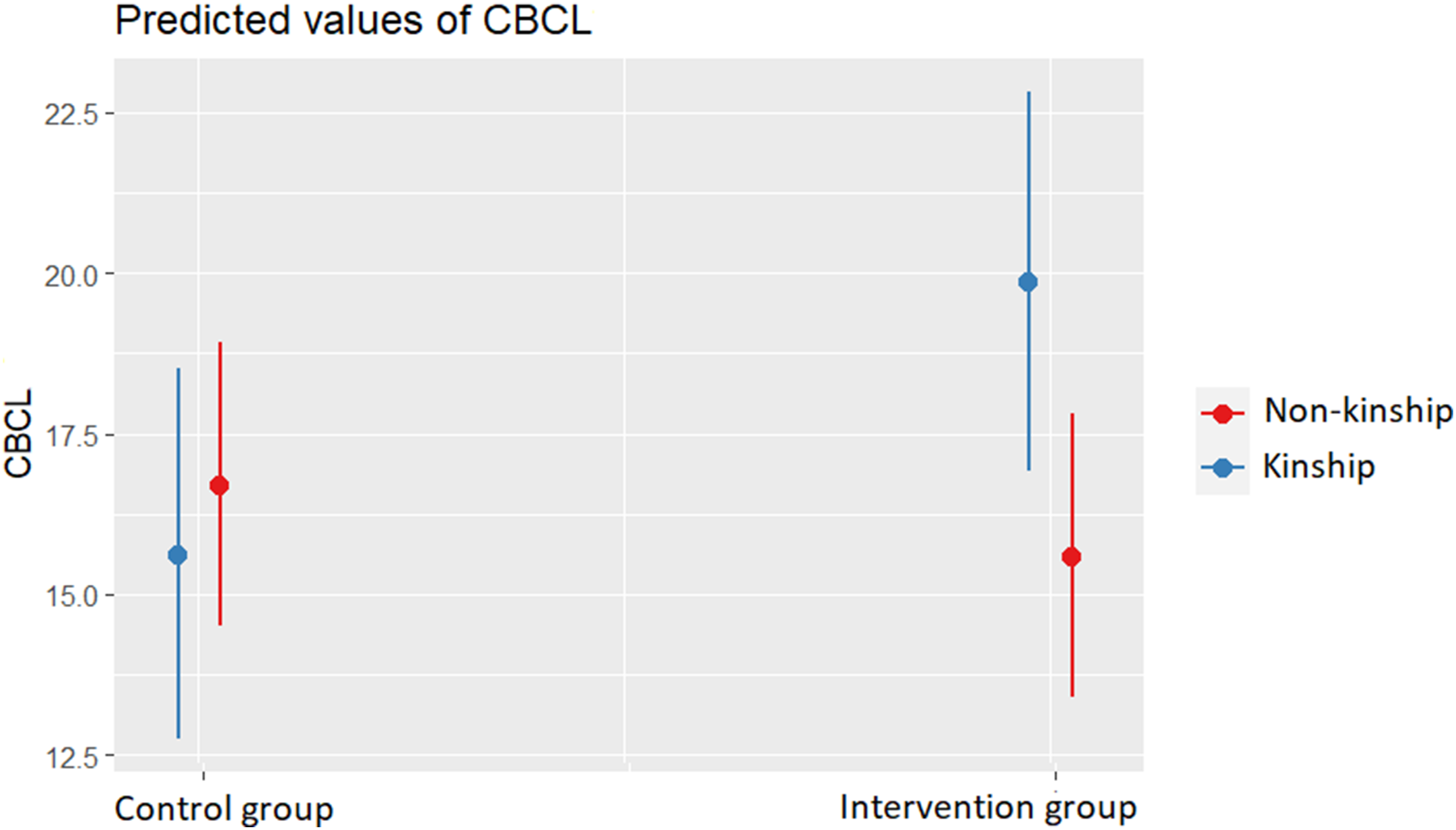
Parenting stress
As indicated in Table 2, there was no significant effect of time (
Discussion
In this study, a RCT of VIPP-FC/A was conducted. It was hypothesised that VIPP-FC/A would increase foster mothers’ sensitive parenting and a decrease of foster mother’s parenting stress. Moreover, it was expected to result in a decrease of externalizing problems behaviour and insecure attachment behaviour of the foster children. Contrary to the hypothesis, there were no main intervention effects for sensitive parenting, externalizing problems, insecure attachment behaviour and parenting stress. There was a significant effect of condition and age on insecure attachment behaviour: within the group of foster children under 30 months, children in the intervention group had lower insecure attachment scores. There was also a significant effect of condition and type of foster care on externalizing behaviour problems. In the group of children placed in kinship foster care, children in the intervention group had lower external behavior scores than children in the control group.
No significant intervention effects of VIPP-FC on sensitive parenting were found. This was a rather unexpected result since a meta-analysis of van IJzendoorn et al. (2023), combining the results of 25 RCT’s testing VIPP-SD, found a small combined effect size on parenting behavior (r = .18). Barone et al. (2019) also detected increased sensitivity among mothers of adopted children in the VIPP-FC/A intervention group (b = 83, p = .001). On the other hand, this result was in line with research conducted by Schoemaker, Juffer, et al. (2020), who found no evidence that VIPP-FC/A was effective in improving foster carers’ sensitive parenting. Foster parents go through a pre-placement selection process and are suppported in positive parenting by social workers throughout the placement. This may result in parenting behavior high in sensitive parenting, which may lead to a ceiling effect. Indeed, Schoemans found high scores on parental sensitivity and sensitive discipline in her sample, indicating little room for improvement (Schoemaker, Juffer, et al., 2020). In our study, foster parents had a mean score of 122.76 (SD = 14.04, range 70–143), at baseline in the control group and 116.82 (SD = 12.87, range 80–142) in the intervention group, while the maximum score for the EA-SR is 160. Another explanation could be the use of the EA-SR instrument. The EA-SR was developed for parents of infants, while the children included in our sample group were older. Moreover, it is a self-reported questionnaire, requiring high levels of introspection and self-knowledge (Vliegen et al., 2009), which could complicate the ability of foster parents to assess their own parental sensitivity.
There was also no main intervention effect for insecurity of attachment between foster children and the foster mothers. We did expect a intervention effect, as the most recent meta-analyses of van IJzendoorn et al. (2023) on VIPP-SD found a small combined effect size on attachment security (r = .23). Schoemaker, Juffer, et al. (2020), on the other hand, did not find any intervention effect of VIPP-FC on quality of attachment between foster children and their foster mothers.
There was however a significant effect of condition and age on insecure attachment behaviour. Within the group of foster children under 30 months, children in the intervention group had lower insecure attachment scores. There was no significant difference between both conditions for the group of foster children of 30 months old. A possible explanation is that the attachment behavior of older children may be less susceptible to change through the VIPP-FC/A intervention. This suggestion is not supported by Schoemaker, Wentholt, et al. (2020), who found no effectiveness of intervention programs for adoptive and foster parents in improving attachment security but also showed that the intervention effects were not moderated by age of the children. Another possibility is that the intervention is less suited for older foster children, as they are more aware of the presence of a VIPP-intervener and the filming, and might behave more social desirable. By not showing their typical behaviour, foster parents might have more trouble implementing the feedback of the VIPP-intervener in their day-to-day life. Contrary to our results, Van Ijzendoorn et al. (2023) in their meta-analysis even found that age of the child did moderate the effectiveness of VIPP-SD, showing stronger effect on attachment in studies with older children (F(14) = 7.48, p = .016).
There was no main intervention effect for externalising problem behaviour of the foster children. Although VIPP-FC aims at diminishing externalising behaviour problems, the results of research of VIPP on problem behaviour is not clear. In the meta-analysis on VIPP-SD (van IJzendoorn et al., 2023), there was no combined effect for externalizing behaviour problems. Schoemaker, Juffer, et al. (2020) were also not able to find an effect of VIPP-FC/A on behaviour problems in their foster care sample. In contrast, Barone et al. (2019) did find decreased externalizing behavioural problems among the children in a study of VIPP-FC/A in a sample of adopted children and their mothers (b = 2.64, p = .01). Van Ijzendoorn et al. (2023) suggested that the effects of the intervention might need more time, referring to Van Zeijl et al. (2006), who found a sleeper effect on externalizing problem behaviour.
There was a significant effect of condition and type of foster care on externalizing behaviour problems. In the group of children placed in kinship foster care, children in the intervention group had lower externalizing behavior scores than children in the control group. This could be due to the pre-existing bond with the child, making foster parents more emotionally investing in their foster child. In addition, non-kinship families receive pre-placement training (Shlonsky & Berrick, 2001), which is likely to be non-existent or limited for kinship families. Therefore, it would be possible that the intervention has a greater effect on the sensitive disciplining of kinship foster caregivers, resulting in a reduction in behavioral problems.
Parenting stress of the foster parents was included because foster parents are known to experience higher levels of parenting stress (Bastiaensen, 2001), which is associated with behaviour problems (Goemans et al., 2018) and difficulties in the attachment relationship between foster children and their foster carers (Gabler et al., 2014; West et al., 2022). There was no main intervention effect of VIPP-FC on parenting stress.
No main intervention effects on the various outcome variables were found. While VIPP-SD has been found to be effective in various at-risk populations, it may not be as effective in foster care situations. This might be due to the population of foster children. Foster children often experience complex social adversity that triggers various developmental mechanisms, which are not limited to the development of maladaptive attachment (Tarren-Sweeney, 2014). Flemish research showed that 85% of the foster children had to deal with at least one traumatic experience besides separation from their primary caregivers (Vanderfaeillie et al., 2014). It might be necessaire to add a specific more trauma-informed part to VIPP-FC/A, in order to fit this foster care sample more.
Another Flemish foster care specific aspect is the temporary nature of the placement. Adoption after a foster care placement is extremely rare in Flanders and although long-term foster care aims at creating permanency, a return home can be considered at any given moment (Van den Bruel, 2012). This can complicate the development of an attachment relationship between foster carers and foster children, cause anxiety for both foster children and foster parents and unconsciously might implicate the engagement of foster parents.
Limitations
Gathering information about families who declined to participate in the study proved to be challenging. Due to the lack of reliable data on non-response rates, the representativeness of the sample could not be assessed. All foster families who participated in the study did so voluntarily, which could introduce a positive selection bias, particularly since the intervention (VIPP-FC) involves filming families, which could be intimidating for those who are struggling with their foster children.
The use of questionnaires instead of observations can be considered a limitation. Nevertheless, questionnaires were used because the researchers had reservations about the feasibility of having foster parents bring the children to a laboratory setting, as it could be a time-consuming and burdensome task, potentially deterring their involvement in the study. The families lived across five provinces, which made asking them to come to a laboratory setting in one central location an important barrier. One of the strengths of VIPP-FC/A is precisely that it is delivered in the home setting. The use of questionnaires in this research did limit the diversity in responses and the kind of data collected. Additionally, all the information was obtained solely from foster mothers, which could potentially lead to concerns regarding common method variance (Podsakoff et al., 2003). Some of the questionnaires required self-reflection, which may have produced different results than direct observations. Furthermore, there is a risk of response bias in studies reliant on questionnaires (Edwards, 1990). As mentioned earlier, the children in our sample were older than the intended age range of the EA-SR and some children in the study were slightly younger than the intended age range for the AISI questionnaire (24 months), which could also affect the results obtained using these questionnaires.
The use of the AISI to assess attachment behavior could also be considered as a limitation. Foster children are more likely to have disorganized attachment relationships with their foster parent (van den Dries et al., 2009; Vasileva & Petermann, 2018). Since this is the least desirable attachment style, an intervention effect of VIPP-FC/A could be a huge benefit. We only used the total insecurity scale, as only that scale was used to examine the convergent validity (Wissink et al., 2016).
The significant dropout rate can be seen as a limitation, as can the fact that families were not blinded to assignment to control or intervention group. Despite all efforts to maximize chances of randomization, the outcome measures at the baseline measurement were not equal for both groups. The scores in the control group were higher for the EA-SR and lower for both the externalizing problem scale of the CBCL and on the AISI were higher in the intervention group, indication more external problems and insecure attachment behaviour.
Suggestions for further research
The findings regarding the effect of VIPP-FC/A for the youngest group of foster children are promising, so it is necessary to do more research in a larger group of young foster children (under 2.5 years). Using the SSP would also provide insight into possible effects of VIPP-FC/A on disorganized attachment behaviour.
The sample consisted of more non-kinship families than kinship families, whereas this is currently reversed in the foster care population. Research with a similar proportion of kinship families as in the population is recommended so that the effect seen on behavioural problems can be revisited. In further research it should be considered to measure sensitive disciplining, as we would expect more sensitive disciplining of foster parents to result in a decrease of behavior problems.
The theoretical basis of the intervention suggests that sensitivity in parenting of foster carers can influence the quality of attachment between foster children and their carers. However, the study did not find any effect of VIPP-FC/A on sensitivity. Nonetheless, an effect of the intervention on insecure attachment behaviour was observed in the youngest group of foster children. More research into the effects of VIPP-FC/A on sensitive parenting is therefore indicated, preferably by adding observations of foster mothers and their foster children.
Similar research also parental attitudes towards parenting and self-efficacy of parents into account. In futhur research, this concepts could be included as outcomes. It might be interesting to include internalizing behaviour problems as well.
The abovementioned additional research should clarify whether additional indications are needed, such as offering the intervention to young foster children or families in network foster care.
Conclusion
In this study the effectiveness of VIPP-FC/A in a Flemish foster care sample was assessed. The intervention effects on these four outcome variables were analysed by constructing four multilevel models. After controlling for the baseline measurement, there was no significant main effect of condition for sensitive parenting, externalizing problems, insecure attachment behaviour and parenting stress. There was however a significant effect of condition and age on insecure attachment behaviour: within the group of youngest foster children (under 30 months), children in the intervention group scored lower insecure attachment scores than children in the control group. Additionally, there was a significant effect of condition and type of foster care on externalizing behaviour problems. In the group of children placed in kinship foster care, children in the intervention group had lower external behavior scores than children in the control group.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.