
Abstract
It is well-known that experiences of out-of-home care (OHC; foster-family care and residential care) are linked to criminal behavior. Less is known how criminal activity in the OHC population develops over the life course and to what extent such development is characterized by desistance or persistence. Using population-based longitudinal register data for more than 740,000 Swedish men and women, of which around 2.5% have experience of OHC, followed until age 40, results from group-based trajectory modelling and multinomial regression suggest that OHC-experienced individuals with various timing and duration of placement, especially men first placed as teenagers, have substantially elevated likelihood for persistent offending compared to peers without OHC experience. However, most OHC-experienced followed pathways characterized by desistance. Our findings have implications for understanding the dynamics of offending in OHC populations and underscores the necessity for interventions that can prevent the onset of criminal careers, as well as disrupt or modify the ongoing paths of offending within this disadvantaged group of individuals.
Introduction
A large body of literature identifies placement in out-of-home care (OHC; foster-family care and residential care) as a risk marker for later criminal behavior (Gypen et al., 2017; Yoon et al., 2018). Similar research on child maltreatment, which extends beyond OHC-experienced individuals (not all maltreated children enter OHC, and not all OHC-experienced individuals were maltreated), provides strong evidence linking child abuse and neglect to future offending (Malvaso et al., 2018). Behind these findings, however, there is a substantial heterogeneity which not only might be attributed to the diversity of data sources and methods, but also to the fact that neither the experience of OHC nor offending behavior are static phenomena.
Developmental and life-course criminologists have long argued for the relevance of viewing offending as a dynamic behavioral process that evolves across age (Farrington et al., 2018), alongside the necessity of exploring early-life factors that might set individuals off on desisting or persisting trajectories (Shaw & Gross, 2008). Given the vast literature on how offending may develop over the life course (e.g., Laub & Sampson, 2003; Matsuda et al., 2022; Moffitt, 1993), a surprisingly limited number of studies have reported how OHC experience is associated with offending trajectories. Among the few studies that do exist, all are based on crude indicators of OHC experience, small and/or high-risk samples, and where the follow-up typically does not extend beyond young adulthood (Yang et al., 2017, 2021; Ryan et al., 2007; Tärnhäll et al., 2023). This generally also holds for related studies on the developmental course of offending among abused and neglected individuals.
Using comprehensive longitudinal register data from a national cohort of more than 740,000 Swedish men and women born in 1972–1979, of which around 2.5% have had various childhood experiences of OHC, the purpose of this study is to describe offending trajectories from age 15 (age of criminal responsibility) until age 40 in Swedish individuals with and without childhood experience of OHC. Using group-based trajectory modelling (GBTM) and multinomial logistic regression analyses on trajectories of offending, we ask how many and what types of offending trajectories can be identified and to what extent these are characterized by desistence and persistence. We also look at whether and to what extent OHC-experienced individuals with various timing and duration of placement are disproportionally found across trajectories, also when a rich set of confounding factors related to the birth parents are accounted for.
Our study overcomes a number of limitations in prior work. Unlike earlier work based on small/high risk or local samples, our approach yields nationally representative findings. Moreover, we distinguish between diverse subgroups within the heterogeneous OHC population, including those entering the system at a young age versus those placed in adolescence. While existing research suggests elevated risks of persistent offending until young adulthood for individuals with OHC experience, it is unclear if this persists over an extended follow-up of around 15 years. It is plausible that those initially on a persistent trajectory might actually cease criminal behavior, aligning with theories on the age-crime curve (Le Blanc, 2020) and desistance (Laub & Sampson, 2003).
Additionally, previous studies have primarily focused on offending trajectories of youth aging out of care, leaving the nature of offending trajectories among other OHC subgroups, such as those entering the child welfare system at a younger age, largely unexplored. Furthermore, few datasets have been extensive enough to analyze long-term offending patterns in a substantial number of female offenders who were previously placed in OHC. Consequently, comprehensive analyses of female-specific offending trajectories until midlife are practically non-existent. Against this backdrop, and in accordance with feminist pathways researchers proposing gender-specific offending patterns (Wattanaporn & Holtfreter, 2014), we present results from sex-stratified analyses.
Method
This study utilizes national comprehensive longitudinal register data. Sweden has a long tradition of national registers with high quality data on offending, health as well as socioeconomic indicators covering the entire population. Since data can be linked through the individual’s personal ID-number which follows each resident from birth to death, it is possible to identify and follow individuals through time within these registers. The registers have long follow-up periods, and include virtually all citizens. Through the Multigenerational Register (held by Statistics Sweden) members of the same birth family can be identified and linked.
Study population
For the purposes of this study, data for eight birth cohorts from 1972–1979 who were alive and residing in Sweden in 1985 according to the Population and Housing Census (held by Statistics Sweden) are used (n = 835,206). We then collected data from the other registers up to the cohort member’s age of 40. This population constitutes a special window in the registers since they include the first birth cohorts in Sweden to have complete data on OHC placements from time of birth to age 18. Due to incomplete data (internal dropout rate 10%), however, the analytical sample corresponds to 747,932 individuals (51%/49% men/women) of which 2.3% (n = 16,862) have experience of OHC (OHC men: n = 8,805/52%; OHC women: n = 8,057/48%). The study was approved by the Swedish Ethical Review Authority in 2020 (no. 2020–00250).
Outcome
The observation window starts when the individuals reached the age of criminal responsibility. Consequently, this study employs yearly prevalence of conviction from age 15 to age 40 according to the Conviction Register (held by the Swedish Council for Crime Prevention) to depict offending trajectories across the life course. This means that data relate to convictions in the period 1987–2019. Prevalence is calculated so that individuals who have had at least one recorded conviction at a given year of age are counted as one (1) and all the others as null (0). Although conviction data typically may be considered a back-end-measure of offending (Andersen & Skardhamar, 2017), Swedish conviction data have a broad coverage of criminal offences and comprise court sentences, fines awarded by the prosecutor and waivers of prosecution implying the guilt of the defendant. Since Swedish police and prosecutors are bound by the legality principle (i.e., the authorities must arrest or prosecute whenever they believe that an offence has occurred), conviction data have a rather high degree of coverage in relation to crimes committed. In addition, Swedish police do not have a sanctioning mandate other than to impose fines for minor offences such as speeding. As a consequence of this, these minor offences are thus not included in convictions data (Nilsson et al., 2017).
Placement in OHC
Using data from the Child Welfare Intervention Register (held by the National Board of Health and Welfare), individuals with OHC experience were categorized into four mutually exclusive groups that depict various combinations of timing and duration of placement (cf. Triseliotis, 1989; Vinnerljung et al., 2007). Given the addressed birth cohorts, OHC data cover the period 1972–1997. The types of placement were used to divide the cohort members into four groups: Early short. Placed for the first time before age 13 and with less than one year totally in OHC before reaching the age of majority (age 18) (mean duration, years = .25, standard deviation/SD = .25; mean age when first placed = 4.85, SD = 4.06); Early intermediate. Placed for the first time before age 13 and with one to five years in OHC before reaching the age of majority (mean duration, years = 2.63 SD = 1.17; mean age when first placed = 6.35, SD = 4.23); Long term. Placed for the first time before age 13 and with more than five years in OHC before reaching the age of majority (mean duration, years = 11.12, SD = 4.19; mean age when first placed = 5.29, SD = 3.75) and; Teenage placement. Placed for the first time at age 13 or later, regardless of total time spent in OHC before reaching age of majority (mean duration, years = 1.58, SD = 1.40; mean age when first placed = 15.84, SD = 1.52).
Reasons for placement in the Early short, Early intermediate and Long-term groups typically include abuse/neglect due to parental behaviors. The Long-term placement group is special since it identifies a population of children that remained in care for a substantial part of their childhood, thereby referring to children that ‘grew up’ in the child welfare system and, accordingly, the society – acting in loco parentis – has assumed far-reaching responsibilities for their well-being and development. In this group, the vast majority ‘age out’ of care (Berlin et al., 2011), Note that the Teenage placement group significantly differs from other groups. While Early short, Early intermediate, and Long-term placements usually result from parental abuse/neglect, many enter the Teenage placement group due to juvenile delinquency and/or substance misuse (i.e., their own antisocial behavior) (Vinnerljung et al., 2001). Given this background, and to compare with OHC population in countries like the US and UK (where such teens are typically handled in the juvenile/youth justice system), it could be argued to exclude this category. However, as teenage placement has long been the prevailing OHC type in Sweden (Berlin, 2020), such an approach would introduce bias, limiting the representativeness of the current OHC sample.
Confounding factors
Descriptive statistics. Sample characteristics by OHC experience, stratified by sex.
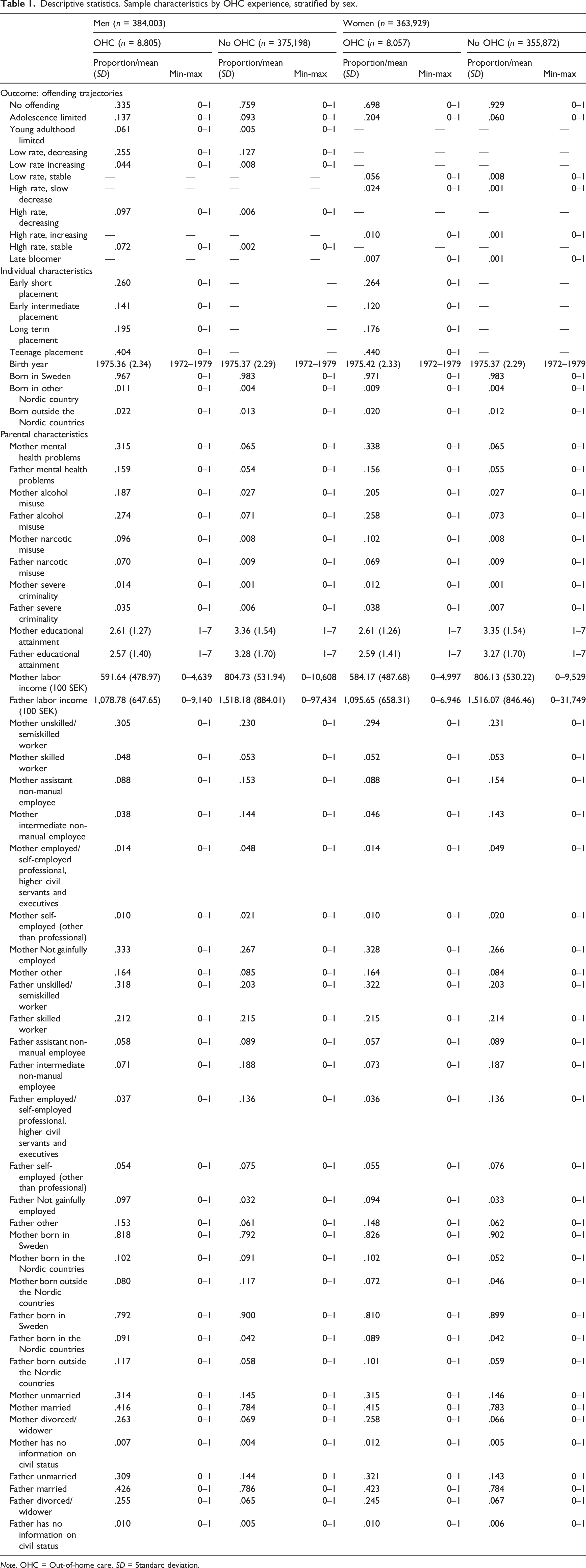
Note. OHC = Out-of-home care. SD = Standard deviation.
Confounders relating to the psychopathological characteristics of each parent were also incorporated. Data from the Patient Register (held by the National Board of Health and Welfare) and the Conviction Register were used to create a set of binary indicators of mental health problems (at least one hospitalization with a psychiatric diagnosis according to standardized ICD-codes), alcohol misuse (at least one hospitalization due to alcohol attributable causes according to standardized ICD-codes), narcotic misuse (at least one hospitalization due to narcotic attributable causes according to standardized ICD-codes), and severe criminality (at least one conviction that resulted in a sentence to probation, prison or psychiatric care).
Due to data limitations, confounders relating to parental civil status and occupational class refer to conditions when the cohort members were between 4 and 8 years old. Parental labor income refers to conditions when cohort members were between 9 and 13 years old. Parental education was measured in 1990, i.e., when cohort members were between 11 and 18 years old. Accordingly, we are to some extent violating the common approach of using pre-care characteristics as controls. In addition to the fact that it is difficult to identify pre-care characteristics for the non-OHC placement group, the utilized measurements may nonetheless offer sufficient proxies for pre-care parental circumstances for the OHC groups. For example, since parenthood tends to be negatively associated with further educational participation (Henz, 2021), parental educational attainment is most likely a rather stable measurement.
Concerning measurements of parental mental health problems, alcohol misuse, narcotics misuse, and severe criminality, we use the entire observation period. Here, it should be noted that hospitalization due to mental health problems or substance misuse requires a certain degree of severity, most often preceded by long-term difficulties. It is therefore likely that such register indicators reflect environmental conditions in the birth homes of the cohort members. The same applies to criminality: in the Swedish court system, probation or prison sentences often follow a series of less severe measures. In essence, although the observation time for these control variables might not be ideal, we contend that they sufficiently capture parental psychopathology.
Statistical analyses
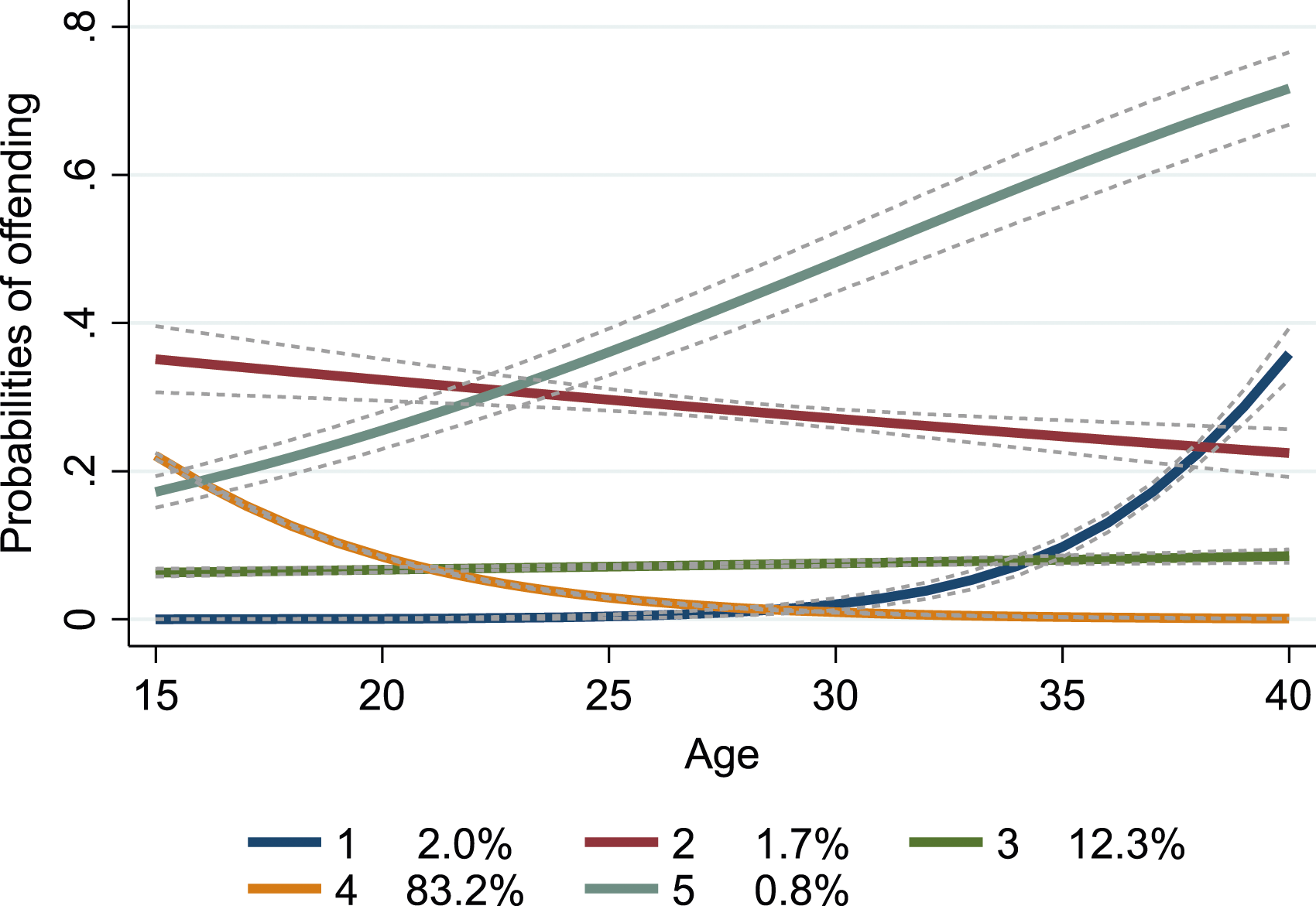
Two types of statistical analysis were performed using Stata 17/SE-version (StataCorp LP, College Station, TX). First, GBTM was employed to group individuals with at least one offending into trajectories using the traj plugin (Jones & Nagin, 2013). The number of trajectories were assessed by fitting several logit models using the intercept (0), linear (1), quadratic (2) and cubic (3) functions. Combined with graphical analyses, and whether the identified trajectories allowed for meaningful interpretations, the most suitable model was selected by considering the following criteria as a whole: (i) a model with a Bayesian Information Criterion (BIC) closest to zero; (ii) mean values of posterior probabilities of the assignment to the trajectory group (entropy>.7 for all groups suggests that individuals are well classified). Against this backdrop, a model with six trajectories which combined quadratic and cubic functions was preferred for men while a model with five trajectories with a linear function was preferred for women. Group labels were informed by prior literature and a visual examination of the shape, peak age, and length of the trajectories as depicted in Figures 1 and 2. Offending trajectories across ages 15–40 among men with at least one offending (n = 96,203). Results from group-based trajectory modelling. 1 = ‘Low rate, increasing (n = 3,417)’; 2 = ‘Low rate, decreasing (n = 49,864)’; 3 = ‘High rate, decreasing (n = 2,988)’; 4 = ‘Adolescence limited (n = 36,263)’; 5 = ‘Young adulthood limited (n = 2,224)’; 6 = ‘High rate, stable (n = 1,447)’. Offending trajectories across ages 15–40 among women with at least one offending (n = 27,745). Results from group-based trajectory modelling. 1 = ‘Late bloomer (n = 557)’; 2 = ‘High rate, slow decrease (n = 484)’; 3 = ‘Low rate, stable (n = 3,397); 4 = ‘Adolescence limited (n = 23,083)’; 5 = ‘High rate, increasing (n = 224).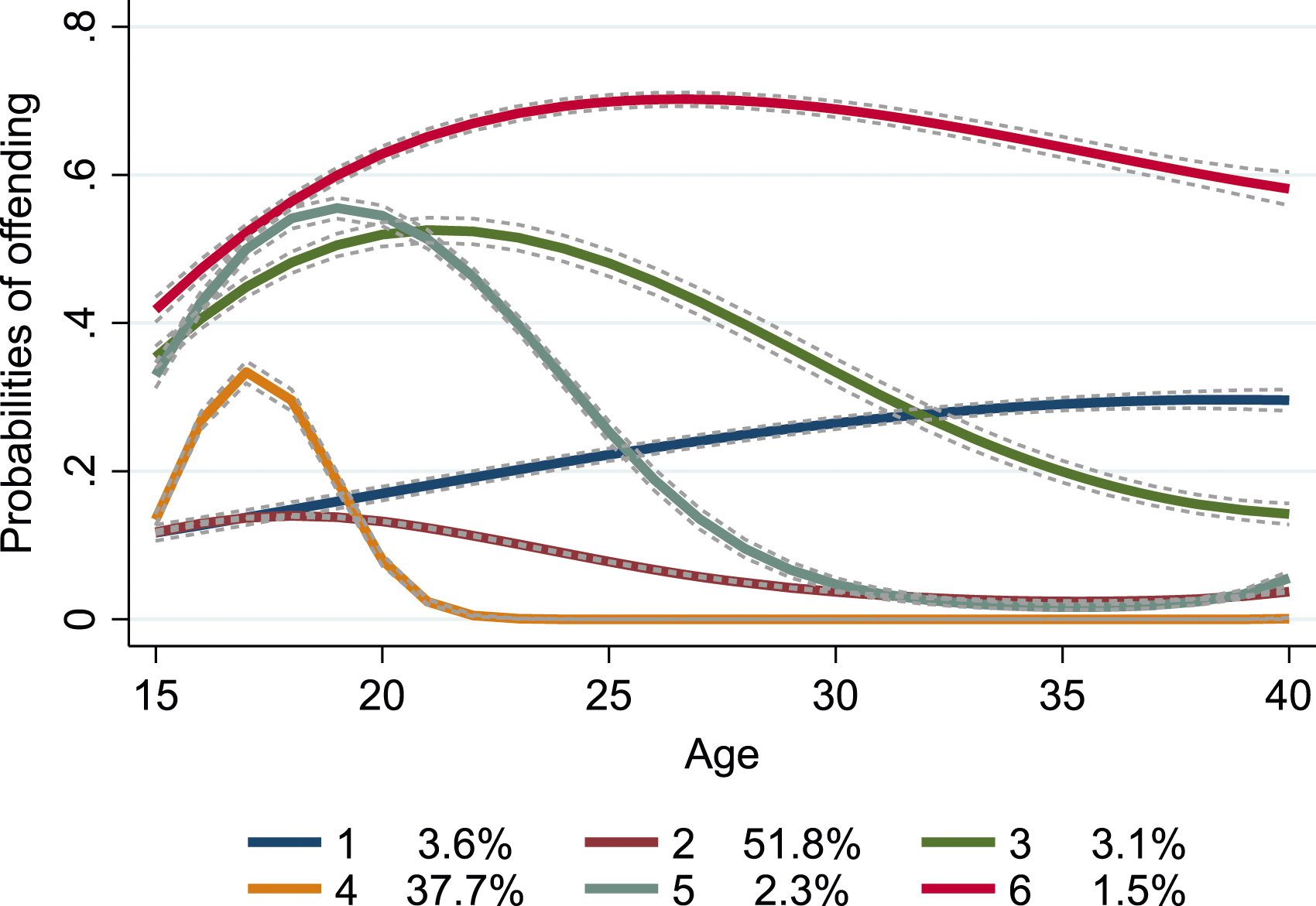
Second, a multinomial logistic regression model was used to examine the associations between OHC groups and the trajectories. Here, all individuals without any offending served as the base outcome. The results show the relative odds among those with various OHC experiences versus those without any such experiences to follow the identified trajectories as opposed to being in the base outcome (i.e., no offending).
To allow for sex-specific responses to OHC exposure as well as sex-specific offending trajectories hypothesized in prior literature, men and women were analyzed separately.
Results
Descriptive statistics by OHC experience reported in Table 1 show that having at least one recorded offending is far more prevalent in the OHC population: around 66% and 30% in men and women respectively. Corresponding for figures for their non-placed peers are 24% and 7%. With the exception for OHC men, it is clear that the vast majority did not have any recorded offending. For both men and women, ‘teenage placement’ was the most common form of OHC, followed by ‘early short’, ‘long term’, and ‘early intermediate’. Examining the demographic and socioeconomic circumstances of the parents of the cohort members, it is clear that the OHC group is strongly selected. For example, parents of the OHC group tend to have higher prevalence of being unmarried, not being gainfully employed, and having lower income. Moreover, issues linked to psychopathology such as mental health problems are notably more prevalent in this group.
Figures 1 and 2 visualize the offending trajectories and report the proportion of individuals following each trajectory among individuals with recorded offending (i.e., the non-offender group is excluded). Figure 1 illustrates the offending trajectories across ages 15–40 among men. Around half of the convicted men followed a trajectory characterized by low-rate probabilities that started decreasing in late adolescence (Trajectory 2; ‘Low rate, decreasing’; 51.8%). The second most common trajectory reflected offending that was limited to adolescence, peaking around age 17 (Trajectory 4; ‘Adolescence limited’; 37.7%). Next, we found a trajectory characterized by low rate-probabilities that gradually increased across the measurement period (Trajectory 1; ‘Low rate, increasing; 3.6%). Two of the less common trajectories – Trajectory 5 (‘Young adulthood limited’; 2.3%) and Trajectory 3 (‘High rate decreasing’; 3.1%), demonstrated relatively high probabilities of offending during adolescence and young adulthood but then diverged after age 20: in the former, the probabilities gradually dropped close to zero in the period before age 30 whereas the decrease was slower and less evident for the latter. Finally, the least common trajectory (Trajectory 6; ‘High rate, stable’; 1.5%) showed a persistently high level of offending. As shown in Table 1, it is clear that OHC-experienced men are disproportionally found in all the trajectories.
In Figure 2, offending trajectories across ages 15–40 among women are shown. The most common trajectory was characterized by relatively high probabilities in middle adolescence but then gradually decreasing across age (Trajectory 4; ‘Adolescence limited’; 83.2%). Second, we found a group of convicted women following a trajectory with a low stable rate of offending (Trajectory 3; ‘Low rate, stable’; 12.3%). Third, a group of late onset offenders was found (Trajectory 1; ‘Late bloomer’; 2%), individuals had a zero probability of offending until around age 30, when the probabilities increased rapidly). The second least common group reflected a slow decrease – from relatively high levels – across the whole measurement period (Trajectory 2: ‘High rate, slow decrease; 1.7%). Lastly, .8% of the convicted women fell into a trajectory that started at a relatively high level and for which there was a steep increase in probabilities of offending across age (Trajectory 5; ‘High rate, increasing’). Like the OHC-experienced men, OHC women are disproportionally found in all trajectories (Table 1).
One of the six trajectories (‘Adolescence limited’) in men, representing nearly 38% of the offenders, followed a clear desisting trajectory. Two other trajectories (‘Low rate, decreasing’ and ‘Young adulthood limited’) may also be interpreted as following a desisting pathway, although the probabilities for offending never reached nil. Taken together, these three categories add up to around 93% of the male offenders. A similar pattern was found in women where 83% followed the clearly desisting trajectory ‘Adolescent limited’. As shown in Table 1, it is clear that most OHC men and women followed desisting pathways.
Although at different levels, three trajectory groups in men (‘High rate, stable’, ‘High rate, decreasing’, ‘Low rate, increasing’) and three groups in women (‘High rate, slow decrease’, ‘High rate, increasing’, ‘Low rate, stable’) persisted in offending from adolescence, through young adulthood and into midlife. In total, these persistent trajectories roughly represent 7% and 15% of the male and female offenders respectively.
Crude and adjusted associations between OHC placement and trajectories of offending across ages 15–40 among men. Results from multinomial logistic regression (n = 384,003).
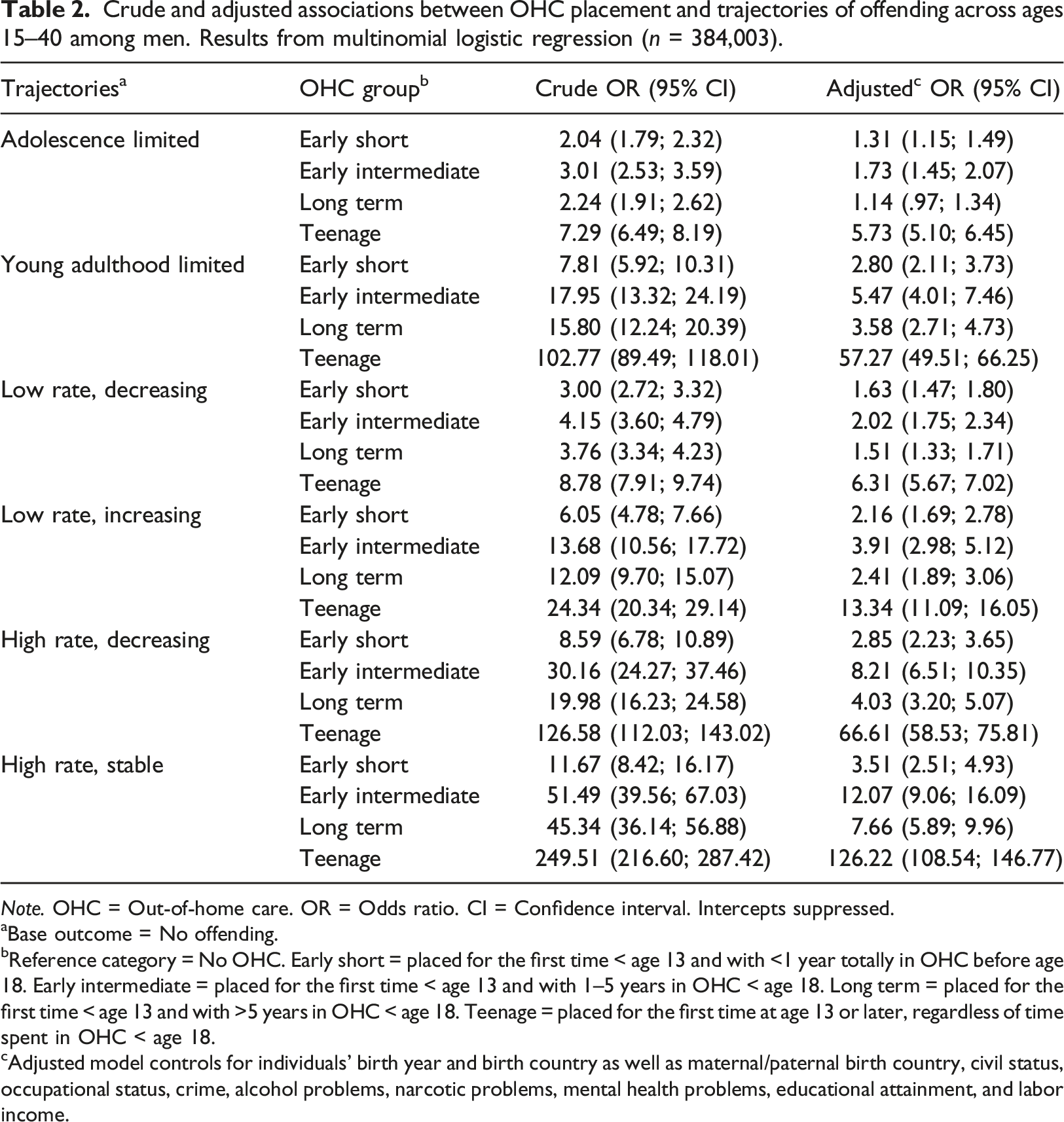
Note. OHC = Out-of-home care. OR = Odds ratio. CI = Confidence interval. Intercepts suppressed.
aBase outcome = No offending.
bReference category = No OHC. Early short = placed for the first time < age 13 and with <1 year totally in OHC before age 18. Early intermediate = placed for the first time < age 13 and with 1–5 years in OHC < age 18. Long term = placed for the first time < age 13 and with >5 years in OHC < age 18. Teenage = placed for the first time at age 13 or later, regardless of time spent in OHC < age 18.
cAdjusted model controls for individuals’ birth year and birth country as well as maternal/paternal birth country, civil status, occupational status, crime, alcohol problems, narcotic problems, mental health problems, educational attainment, and labor income.
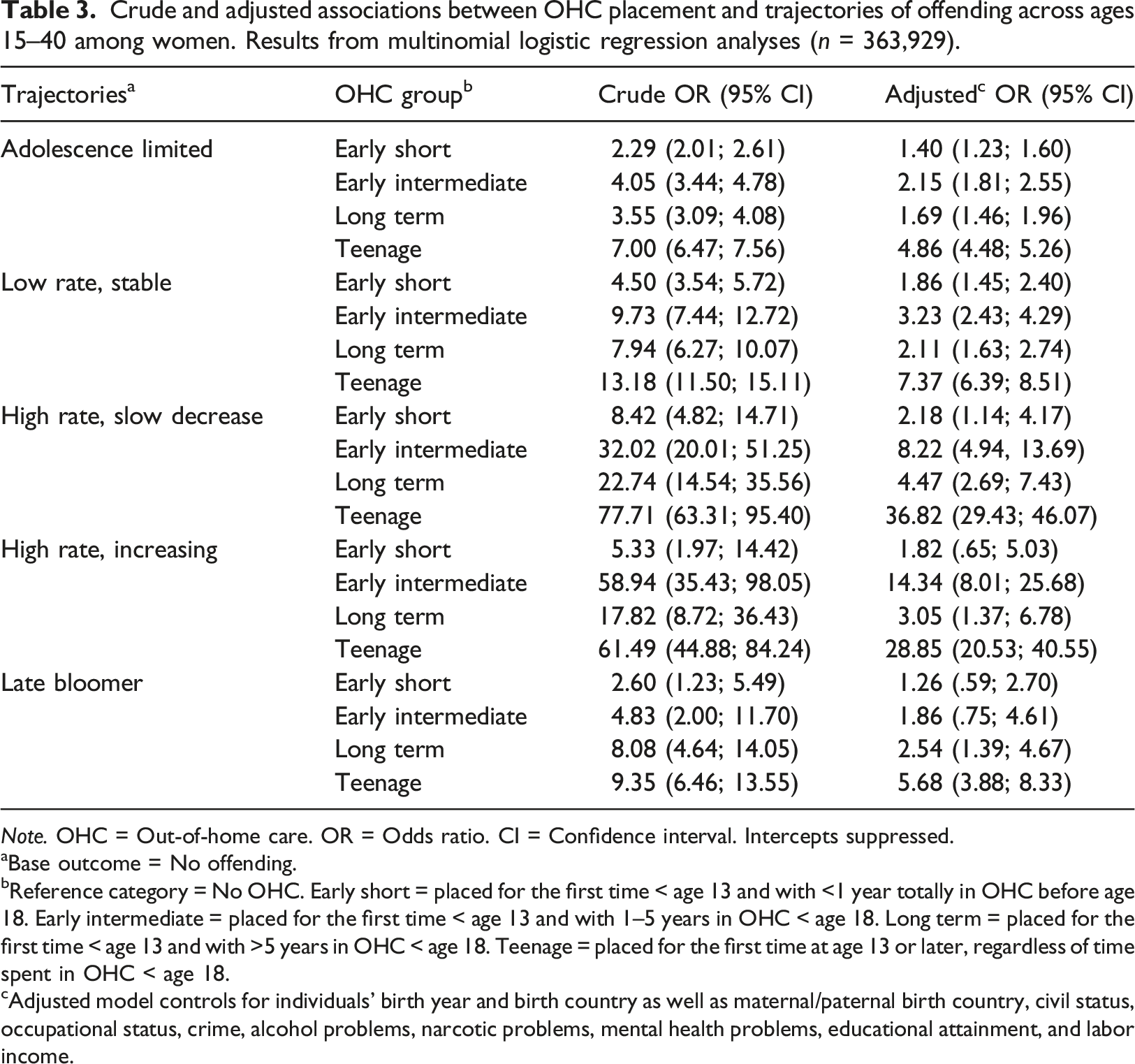
Crude and adjusted associations between OHC placement and trajectories of offending across ages 15–40 among women. Results from multinomial logistic regression analyses (n = 363,929).
Note. OHC = Out-of-home care. OR = Odds ratio. CI = Confidence interval. Intercepts suppressed.
aBase outcome = No offending.
bReference category = No OHC. Early short = placed for the first time < age 13 and with <1 year totally in OHC before age 18. Early intermediate = placed for the first time < age 13 and with 1–5 years in OHC < age 18. Long term = placed for the first time < age 13 and with >5 years in OHC < age 18. Teenage = placed for the first time at age 13 or later, regardless of time spent in OHC < age 18.
cAdjusted model controls for individuals’ birth year and birth country as well as maternal/paternal birth country, civil status, occupational status, crime, alcohol problems, narcotic problems, mental health problems, educational attainment, and labor income.
Adjusting for individual and parental characteristics undeniably resulted in the strength of the associations becoming substantially reduced. Reduction in ORs varied between approximately 36%–83%, but mostly all of them remained statistically significant (p < .05) and at non-negligible elevated levels. However, with the exception of following the ‘High rate, slow decrease’ trajectory, women who had experienced short placement before their teens had low to negligible elevated odds for following all type of trajectories (ORs = 1.26–1.86). Negligible associations were also found in corresponding men for following the ‘Adolescence limited’ (OR = 1.31) and ‘Low rate, decreasing’ (OR = 1.63) trajectories. Yet the associations for following the other trajectories were more sizable (ORs = 2.16–3.51). The size of the associations for the long-term group mostly mimicked the short-term group rather than the intermediate group, especially in men. However, men and women who ‘grew up’ in care demonstrated around three to seven-fold elevated odds for following various forms of high-rate persistent trajectories. However, the size of the associations for the teenage group clearly stand out: men who were first placed in their teens had almost 126 times the odds of following the most persistent pathway. A similar pattern was also found in women who had around 29 times the odds of following the ‘High rate, increasing’ trajectory. The second largest association among men in the teenage group refer to following the ‘High rate, decreasing’ trajectory (OR = 66.61). Corresponding association in women refers to following the ‘Late bloomer’ trajectory where a nearly six-fold elevated odds was found.
Discussion
To our knowledge, this population-based study was the first to describe offending trajectories beyond young adulthood in individuals with diverse childhood experiences concerning the timing and duration of OHC. Using comprehensive data from a nationwide cohort of Swedish men and women, followed in national social and crime registers from birth until age 40, results from sex-stratified GBTM revealed six groups in men and five groups in women. Multinomial logistic regression analyses showed that OHC-experienced had elevated likelihood to follow all type of offending groups rather than the non-offending group. OHC-experienced were disproportionally found to follow persisting offending trajectories, thereby being in accordance with prior studies addressing this population (Tärnhäll et al., 2023; Yang et al., 2017, 2021).
However, and in contrast to prior work, most OHC men and women followed desisting pathways. This highlights the advantage of having a follow-up that extends beyond young adulthood, as individuals initially on a persistent trajectory may actually discontinue engaging in criminal behavior (see Laub & Sampson, 2003; Le Blanc, 2020). A longer follow-up, along with a massive sample size, also allowed for the identification a small group of late bloomers (see Matsuda et al., 2022) among women, in which individuals with OHC experience also were disproportionally found. The associations were moreover particularly pronounced for those men and women who were first placed in teenage years. Since this group typically consists of adolescents placed in OHC for reasons related to juvenile delinquency or other forms of antisocial behavior (Vinnerljung et al., 2001), this falls in with previous Swedish studies demonstrating that this group have dire outcomes as young adults, almost regardless of outcome measure (e.g., Vinnerljung & Sallnäs, 2008). However, before this study, little has been known of persistency of offending until midlife, especially in women.
Among individuals placed before their teens, the odds regarding unfavorable trajectories for the intermediate group were typically higher compared to the long-term group. Several UK studies comparing long-term outcomes for children returning to birth families with peers who aged out of foster-family care have found better outcomes for the former group (e.g., Biehal et al., 2015; Wade et al., 2010). If our results are associated with poorer home environment for the reunited children and/or a protective effect of long-term care is unfortunately beyond the scope of our data to analyze.
Strengths and limitations
Strengths of this study include its longitudinal design, the massive cohort sample of Swedish men and women born 1972–1979, a follow-up time that extends beyond emerging/young adulthood, the use of national register data with limited attrition, and robust controls of confounders related to the birth home. Not the least, the sample includes a sizeable number of OHC-experienced individuals with different timing and duration of placement. However, all register-based studies have limitations and ours does not represent an exception to this rule.
Apart from the fact that administrative records of offending may underestimate the prevalence of offending behaviors, register-based studies typically provide an ‘aerial view’ of complex developmental and life-course processes. Data that could be vital for our understanding of the criminal careers of OHC-experienced individuals such as genetic factors and personality traits are often outside the scope of nationwide register-based studies. Indicators of the birth parents’ substance misuse, narcotics misuse and severe criminality were moreover observed throughout the entire observation period. Although an extended observation period such as ours has its merits because, for example, hospitalization due to mental health problems often occurs after many years of difficulties, the indicators of parental psychopathology remain short on precision.
Another limitation refers to the lack of more detailed data on whether OHC children have experienced stable/nonstable placements and/or high-/low-quality care. We also lack information on reasons for placement, meaning that we are referred to the assumption that children entering care in younger age typically do so due to parental problems. Such data would more likely have promoted our understanding of OHC-experienced criminal careers across the life course. Yet another potential limitation arises from the fact that the analyzed birth cohorts are from the 1970s, potentially not reflecting the current demographic diversity of children entering OHC. In contrast to the 1970s, when approximately 7% of the population was foreign-born, Sweden has since transformed into a multi-ethnic nation, with around 20% of the population now born in another country (Statistics Sweden, 2022). Although foreign-born individuals have long been overrepresented in social services’ work with families, the number of children and families with migration backgrounds has risen (Socialstyrelsen, 2010). However, due to the need to wait 30–40 years to analyze offending trajectories until midlife for the OHC population born in the 2010s and 2020s, these shifting demographics affect the generalizability of findings in this study in unknown ways.
During the 1980s and 1990s, there was a strong increase in the use of (mostly private/for profit) residential care for children of all ages, in contrast to the intentions of legislators (Vinnerljung et al., 1999). This has since settled into a relative stabile pattern. Since evaluations of Swedish residential care are non-existent – both now and in previous decades – we have scant data to help us speculate on the effects for our cohorts. One reasonably large follow-up study (n > 700) found poorer outcomes in young adult age – including offending – for teenagers born 1975–1978 placed in residential care compared to foster-family care, after adjustment for anti-social behavior before placement (Vinnerljung & Sallnäs, 2008). This could indicate that these changes have not been beneficial for children/youth receiving OHC.
Given that all studies include trade-offs, an additional possible limitation reflects the choice of using yearly binary indications of all-type offending. The Conviction Register allows for counting the number of yearly offences as well as for distinguishing between types of offending (e.g., violent, property) and types of penalty (e.g., prison, probation). However, delving deeper into these circumstances was beyond the scope of this study. As far as we are aware, this study is the first to use national and population-based register data in a longitudinal design to describe sex-specific patterns of desisting and persisting trajectories of offending from adolescence until midlife in OHC populations with various experience of timing and duration of placement. Doing so, it has arguably established the phenomenon which expresses sufficient regularity to require and allow further explanation (cf. Merton, 1987). By such background, future research may therefore wish to capitalize on the high granularity of offending data to further the understanding of how criminal careers in OHC populations may vary due to e.g. degree and nature of versatility in crime, and penalties.
Implications
The results of this study should be of interest for both policymakers and practitioners in child welfare settings. Society has invested heavily to improve the life chances of individuals with OHC. This particularly holds for the long-term OHC group since such individuals have ‘grown up’ in care, implying that they have had the society as parent during a substantial part of their upbringing. Irrespective of whether the results allow for causal interpretations, OHC experience is not only a well-known risk marker for future offending, but – as shown in this study – also a strong marker for entering persisting offending trajectories. However, these results should not overshadow the fact that most OHC men and women with recorded offending followed desisting pathways, thereby aligning with developmental life-course theories which posit that, eventually, the vast majority of offenders desist from crime (Le Blanc, 2020; Sampson & Laub, 2003). Hence, while individuals with OHC experience are overrepresented in subgroups of chronic offenders, a majority of them seem to fare reasonably well in midlife with respect to criminal behaviors.
In light of above, there are a number of policy relevant issues that cannot be ignored. The social and economic burdens of offending for the individual and the society are widely acknowledged. Considering the dismal results concerning the group entering care in adolescence, action from policymakers should be taken to improve OHC for this group. As far as we know, few – if any – residential care facility has been evaluated. This means that society sends a large number of teenagers annually into treatment without having any knowledge if the care is beneficial, has null effects or is harmful. From the literature, it is reasonable to assume that the two latter alternatives are dominant. Empirically supported alternatives exist, are cost efficient, but only marginally used (Åström et al., 2020).
Given the recurring appeals for identifying entry points for prevention and intervention, it is worth emphasizing that poor school performance is a strong predictor of criminal behavior (Vinnerljung et al., 2010). In a national cohort study of long-term OHC youths transitioning to adulthood, poor primary school performance accounted for 55% of the significantly elevated risk of crime observed in this group (Berlin et al., 2011). This effect remained even after accounting for indicators of parental psychopathology (similar to the variables used in this study). Therefore, providing effective educational support during primary school could serve as a promising avenue for preventing criminal behavior among children in the child welfare system.
Conclusions
This study provides a solid empirical basis for claiming that individuals with OHC experience have substantially elevated risks of facing persisting offending from adolescence, through young adulthood into midlife. These results emphasize the need for interventions that may prevent the initiation of criminal careers as well as interrupt or alter persisting offending trajectories in this group of disadvantaged individuals, and for repeating previous calls for evaluations of OHC treatment targeting adolescents (e.g., Sallnäs & Vinnerljung, 2009). Research using nationwide samples including a sizeable OHC population from other countries is nevertheless needed to more firmly determine the external validity of the findings reported in this study.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Swedish Research Council for Health, Working Life and Welfare (Forskningsrådet om Hälsa, Arbetsliv och Välfärd) (grant number 2019-00057).