
Abstract
It is well known that individuals with out-of-home care (OHC) experience tend to have lower educational attainment than their peers in young adulthood, and a number of interventions have been implemented to increase their higher education outcomes. However, the timing of their higher education completion, and whether they experience educational recovery over the life course, is largely unknown. Using longitudinal Swedish data from a birth cohort of more than 13,000 individuals, this study examined OHC experienced individuals’ chances of having a higher education, here defined as a record of postsecondary education of two years or more, in midlife (age 50) and whether the timing of completion differs between them and a group of individuals who had child welfare contact (CWC) without being placed, and a group of general population peers. Results from multivariable logistic regressions corroborated prior findings that individuals who have been placed in OHC were less likely to have completed higher education compared to their general population peers. However, among those who did, they were more likely to have completed it later in life. Overall, there were no differences between the OHC group and the CWC group, both groups may thus not only benefit from specific support but also from more general inclusive education policies that allow for life-long learning.
Introduction
Issues related to the developmental outcomes of individuals with involvement in the child welfare system continues to remain at the core of social work research, policy and practice agenda (Courtney & Thoburn, 2009; Martínez, Cobo, Herrera, & Herrera-Viedma, 2015Martínez et al., 2015). A continually growing body of research shows that individuals who have experienced out-of-home care (OHC, foster family and residential care) tend to have poorer school performance than their peers (O’Higgins et al., 2015; Trout et al., 2008) and are less likely to have completed a higher (i.e. postsecondary) education in young adulthood (Gypen et al., 2017; Kääriälä & Hiilamo, 2017). This is particularly concerning given the importance of education for future life chances (Esping-Andersen, 2005). Consequently, child welfare and educational researchers, policymakers, and professionals have shown an increased interest in ways of improving OHC children’s school performance and facilitating higher education enrollment and completion through specific interventions (Evans et al., 2017; Randolph & Thompson, 2017). From a life course perspective, higher education participation has been seen as a key marker in the transition from adolescence to adulthood (Pallas, 2003). In this transition, the traditional pathway is usually defined as compulsory school completion, postsecondary degree attainment, employment, family formation and parenthood (Bozick & DeLuca, 2005). Yet, deviations from this order are widespread and taking alternative routes and delaying the pursuit of higher education completion seem particularly common among socioeconomically disadvantaged and marginalized groups (Bozick & DeLuca, 2005; Milesi, 2010).
Young people with OHC experience constitutes one of society’s most disadvantaged groups (Gypen et al., 2017; Kääriälä & Hiilamo, 2017). Previous studies have shown that they face many challenges in their transition into adulthood (Häggman-Laitila et al., 2019). Obstacles specifically linked to higher education participation include factors related to academic qualifications and preparation, mental health, social network and supportive relationships as well as finances and housing (Geiger & Beltran, 2017; Gillum et al., 2016). Consequently, previous studies have reported lower enrollment rates and/or delayed enrollment compared to peers (Courtney et al., 2011; Gillum et al., 2016; Harrison, 2020; Pecora et al., 2006). Still, enrollment is only the first step to having a higher education. Noted obstacles also seem to lead to higher attrition rates in terms of both permanent exits (i.e. drop-outs) and temporary withdrawals (i.e. stop-outs) which is also reflected in slower graduation rates (Day et al., 2013; Day et al., 2021; Harrison, 2020; Pecora et al., 2006).
Qualitative life course studies have identified a wide range and diversity in OHC experienced individuals’ educational trajectories to higher education later in life (e.g. Brady, 2020; Brady & Gilligan, 2019). Quantitative studies focused on educational outcomes in young adulthood (approximately ages 18–30) also indicate a delayed pursuit of higher education completion by this group (e.g. Day et al., 2013; Harrison, 2020). This implies that higher education completion rates among individuals who have been placed in OHC might increase over time. They might experience educational recovery later in life within education systems that allow for non-traditional pathways and has tolerance for educational late blooming (Levin & Levin, 1991; Pallas, 2003). Still, this is an empirical question. Since long-term quantitative data are largely unavailable, past research has hitherto not been able to examine higher education completion beyond young adulthood and the timing of higher education over the life course.
Using longitudinal Swedish data of a cohort of more than 13,000 individuals, the purpose of this study is to further our understanding of the timing of higher education completion over the life course in OHC experienced individuals. This is achieved by first, examining their chances of having a higher education (i.e. a record of postsecondary education of two years or more) in midlife (age 50) and, second, examining whether the timing of completion differs between them and their peers. As far as we can tell, such data and design are unique in an international perspective.
Apart from having a truly long-term follow-up, which allows for a life course perspective on educational attainment, this study adds to prior research in a number of ways. We study OHC experienced individuals’ educational outcomes in a context which is believed to enable life-long learning, especially among disadvantaged groups. The Swedish child welfare system does not include any mandatory interventions for children ageing out of the OHC system and the education system does not include policies specifically targeting individuals who have experienced OHC. Yet, the education system is organized to facilitate advancement and transitions between different parts and includes general inclusive policies such as adult education, and grant-aided university/university college studies which are free of charge (Halldén, 2008). This could enable educational recovery for individuals who have been placed in OHC and other disadvantaged groups. Furthermore, to address potential heterogeneity within the larger OHC group it is divided into two groups based on the first placement (0–12 years and 13–19 years). Younger children are more often placed due to family circumstances while teenagers are more commonly being placed due to their own behavior, which may affect their educational outcomes (O’Higgins et al., 2017). Moreover, we include alternative comparison groups of individuals who came in contact with the child welfare system (at ages 0–12 and 13–19, respectively) without being placed. Previous Swedish studies have found that individuals who have experienced OHC are more educationally disadvantaged than individuals who have received in-home services (e.g. Vinnerljung et al., 2010), while other studies who have used comparison groups with similar backgrounds have found no differences or even better outcomes among the placed children (e.g. Sinclair et al., 2020; Wall-Wieler et al., 2019). It is thus unclear to what extent educational outcomes may differ between individuals with different types of child welfare involvement, but by including a comparison group which is believed to share a similar background to children placed in OHC, we can to some extent account for selection processes underlying a placement. In doing so, we may be better equipped to inform efforts aimed at improving higher education outcomes in individuals for whom society, acting in loco parentis, has assumed responsibility.
Methods
Data come from the Stockholm Birth Cohort Multigenerational Study (SBC Multigen), which was created through a probability matching of two anonymized data materials: the Stockholm Metropolitan Study (SMS) and RELINK53. The SMS consists of all individuals born in 1953, who were living in the greater Stockholm metropolitan area in 1963 (n = 15,117). Survey and register data were collected until 1986, when the SMS was deidentified. RELINK53 is defined as all individuals born 1953 living in Sweden in 1960, 1965 and/or 1968 and their family linkages (n = 2,390,753). It includes register data from 1953 to 2018. Based on variables identical to both data materials, 14,608 individuals from SMS were matched with RELINK53, resulting in the SBC Multigen (see Almquist et al., 2019 for details on the matching process).
The study population consists of the 13,094 cohort members who were alive at age 50 (2003) and had information on all included variables (n = 579 were lost due to mortality and n = 935 due to incomplete data), reducing the effective sample with around 10%.
The creation of the SBC Multigen and the current study were approved by the Stockholm Regional Ethical Review Board (no. 2016/481–31/5; 2017/34–31/5). Informed consent was not required due to the anonymized nature of the data material.
Variables
The outcome is higher education, which was operationalized into two variables. The first is a binary variable reflecting whether the cohort members had a record of postsecondary vocational or academic education of two years or more at age 50 (2003): (1) ‘Yes’; (0) ‘No’. The second is a categorical variable, which indicates the timing of the higher education completion among those who had a record thereof: (1) ‘Higher education at age 30’ (−1983); (2) ‘Higher education ages 31–40’ (1984–1993); and (3) ‘Higher education ages 41–50’ (1994–2003). The variables were based on a combination of information about postsecondary education in educational registers in the SMS (periodical data; 1977, 1980, and 1983) and the Longitudinal Integration Database for Health Insurance and Labor Market Studies in RELINK53 (yearly data; 1990–2003). It should be noted that there are some differences in how higher education was recorded in these registers, which may have resulted in an underestimation of the number of cohort members who had a higher education at age 30, and consequently an overestimation of completion rates at ages 31–40. Yet, this would have affected all cohort members, across all study groups, equally.
The education system was repeatedly reformed into a more egalitarian system during the upbringing of the 1953 cohort (Halldén, 2008). However, compared to today, their schooling included more tracking and it was far less common that they proceeded directly to upper secondary education following compulsory school completion. Still, in the late 1960’s, a tuition-free adult education system was introduced which enabled cohort members to complete and/or make up their qualifications in adulthood. While admission to higher education in Sweden sometimes is based on work experience, academic qualifications were – and still are – the basis for applications to university/university college studies. The adult education system could thus act as a springboard for further studies.
The group variable child welfare involvement was created based on records of child welfare measures and decisions in the municipal Social Registers between birth and age 19 (1953–1972). Mutually exclusive groups were coded as follows: 1. ‘Out-of-home care 0–12 years’: Individuals who had their first placement in OHC before age 13. Almost 84% were placed due to family circumstances, around 4% were placed due to their own behavior, and the rest had registered placement decisions based on both types of causes. Around one fifth were placed in family-based foster care, three in five were placed in residential care, and one fifth experienced both placement types. While placement duration is often unspecified in the registers, it is estimated that most experienced short-term placements (<2 years); 2. ‘Out-of-home care 13–19 years’: Individuals who had their first placement in OHC as teenagers. Close to 14% were placed due family circumstances, around 85% were placed due to their own behavior, and the rest had registered placement decisions based on both types of causes. Around 30% were placed in family-based foster care, 40% were placed in residential care, and 30% experienced both placement types. As noted above, placement duration is often unspecified, but it is estimated that most experienced short-term placements (<2 years); 3. ‘Child welfare contact (CWC) 0–12 years’: Individuals who were first investigated by the child welfare services before age 13, but never placed in OHC during childhood. Around 24% received in-home services, the rest were registered as not substantiated investigation; 4. ‘Child welfare contact 13–19 years’: Individuals who were first investigated as teenagers, but never placed in OHC. Around 12% received in-home services, the rest were registered as not substantiated investigation; 5. ‘General population (GP)’: Individuals without any child welfare involvement.
The Swedish child welfare system during the childhood years of the 1953 cohort was characterized by more interventionist ideas compared to the present system in which more focus is put on family preservation and in-home services. This is reflected in the OHC prevalence in the 1953 cohort of almost 9% with mostly younger children in comparison to around 5% in national cohorts born 1990–1995 where most had their first placement during their teens (Berlin, 2020). As today, child welfare involvement could be caused by parental neglect, mental health problems and alcohol misuse as well as children’s own antisocial behavior. But reasons were also related to teenage and/or lone parenthood (mother), poverty, and unsatisfactory housing (Vinnerljung, 1996). In recent years, reasons related to abuse, maternal drug misuse, and family violence are more frequent (Khoo et al., 2012).
Household occupational status and sex are used as control variables. Household occupational class is well-known to influence educational attainment (Breen & Jonsson, 2005) as well as OHC placement (Franzen et al., 2008). Information on household occupational class at birth (1953) was coded into a binary variable reflecting whether or not the cohort member had a working-class background: (1) ‘Yes’ [i.e. ‘working-class, unskilled worker’ + ‘working-class, skilled worker’]; (0) ‘No’ [i.e. ‘lower-middle class, entrepreneur’ + ‘lower-middle class, officials and non-agricultural employees’ + ‘upper and upper-middle class’]. The variable was based on data retrieved from the Delivery Records or the Stockholm Population Register and reflects the position of the head of the household, mostly the biological father. Females typically outperform males in the educational system (Buchmann et al., 2008; O'Higgins et al., 2017) and seem to have better long-term outcomes after OHC (e.g. Vinnerljung, 1996). The cohort member’s biological sex at birth (1953) was therefore included as a covariate and is indicated by the categories: (1) ‘Female’; (0) ‘Male’.
Statistical analyses
The statistical analyses were carried out in three steps. First, descriptive statistics for the full sample and by child welfare involvement were conducted. Second, to examine the association between child welfare involvement and the chances of having a higher education at age 50, a set of binary logistic regression models were estimated. Lastly, to assess how child welfare involvement was associated with the timing of higher education completion, multinomial logistic regression analysis was performed. Both logistic regression models report odds ratios (OR) along with 95% confidence intervals (CI).
Logistic regression analysis is widely used in the social sciences, typically when we are interested in assessing the effect of a particular independent variable on a dichotomous or polytomous dependent variable net of observed confounding factors. In linear regression analysis, controlling for confounding factors and interpretations of controlled coefficients are well understood. However, inherent problems with interpretations of controlled coefficients (e.g. OR) from logistic regression models are less understood (Karlson et al., 2012). The difference between uncontrolled and controlled coefficients in logistic regression models may be the result of confounding but also because of rescaling (Williams, 2009). Rescaling is here understood as a situation where the size of a coefficient of a variable of interest depends on the error variance of the model and, accordingly, on which other variables are included in the model (Karlson et al., 2012). Since the error variance in logistic regression is fixed (Winship & Mare, 1984), coefficients from a bivariate logistic regression model and a multivariate logistic regression model are not necessarily measured on the same scale and are therefore not comparable. Accordingly, we cannot simply compare and interpret crude and adjusted logistic regression coefficients because we cannot distinguish between the magnitude of confounding relative to the magnitude of rescaling.
To circumvent logistic regression’s inherent problems related to rescaling bias, all regression models were estimated using the Karlson/Holm/Breen (KHB) method, thereby facilitating comparisons between crude and adjusted ORs. The KHB method ensures that the crude and adjusted ORs presented are measured on the same scale and thereby are unaffected by the rescaling bias that arise in cross-model comparisons of logistic regression models. (Karlson et al., 2012).
Furthermore, following each regression model, pairwise comparisons of margins across the different types of child welfare involvement were conducted to examine whether the two OHC groups differed significantly from their CWC group counterpart (i.e. the younger OHC group was contrasted to the younger CWC group while the teen OHC group was compared to the teen CWC group). This control-by-design strategy was used in an attempt to further account for selection processes underlying placement in OHC.
All analyses were performed using Stata/MP 16.0 (StataCorp LP, College Station, TX). The logistic regressions were estimated using the khb command (Kohler et al., 2011) and the pairwise comparisons were done with the pwcompare command.
Results
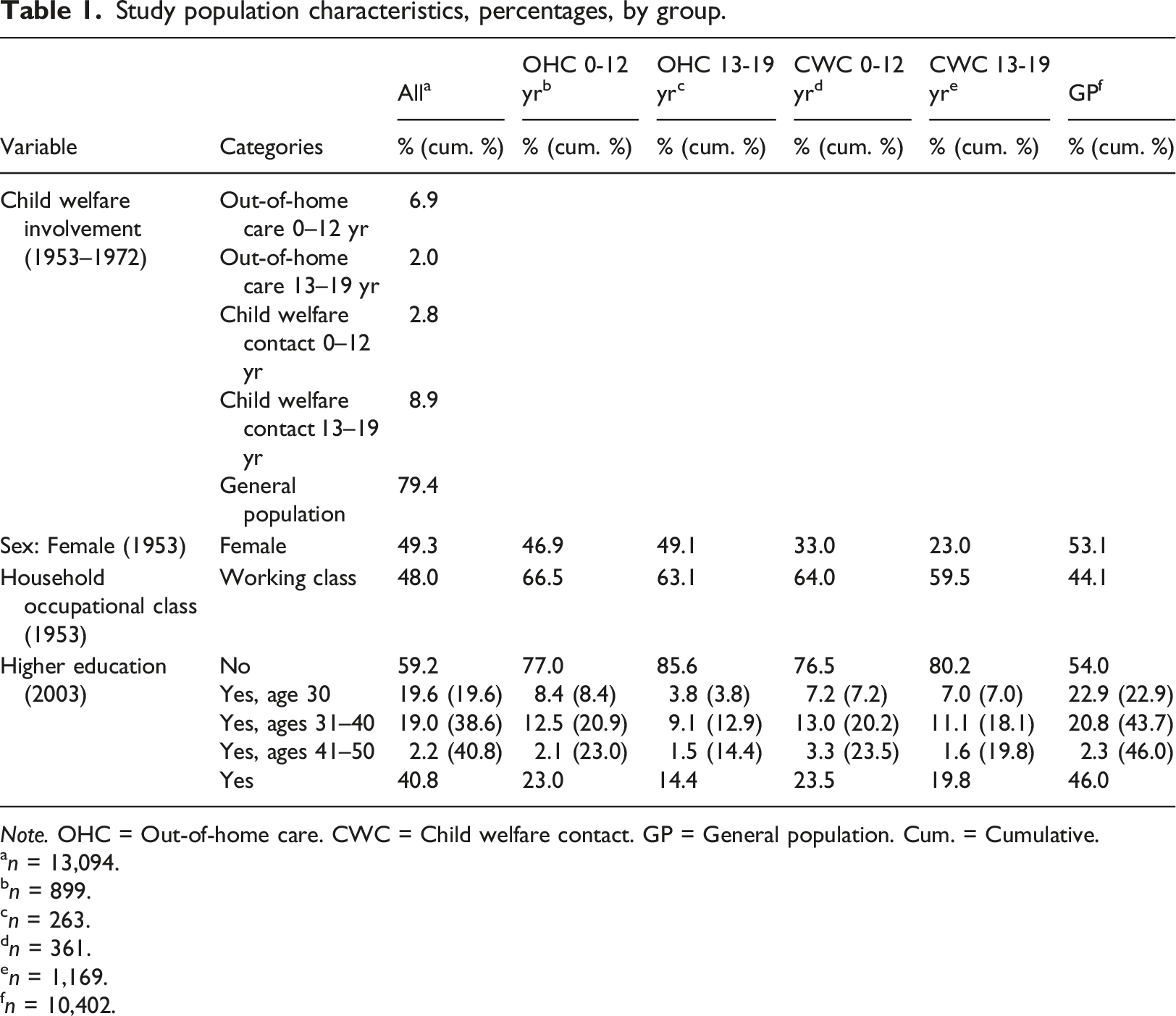
Study population characteristics, percentages, by group.
Note. OHC = Out-of-home care. CWC = Child welfare contact. GP = General population. Cum. = Cumulative.
an = 13,094.
bn = 899.
cn = 263.
dn = 361.
en = 1,169.
fn = 10,402.
Females constituted around 53% of the GP group. In contrast, females were somewhat underrepresented in both OHC groups (47% and 49%). Furthermore, females only made up a third (33%) in the younger CWC group and less than a fourth (23%) in the teen CWC group. A minority (44%) of individuals in the GP group came from a working-class background compared to around two-thirds (67% and 63%) of those placed in OHC, which was rather similar to the distribution in the CWC groups (64% and 60%).
At age 30, 23% in the GP group had a higher education, compared to 8% in the younger OHC group, 4% in the teen OHC group, and 7% in both CWC groups. One fifth (21%) of individuals in the GP group had completed a higher education at ages 31–40. Corresponding numbers in the younger OHC and CWC groups were 13%, while the share in the teen OHC and CWC groups were 9%, and 11%, respectively. Across all groups, around 2%–3% had completed a higher education at ages 41–50. Accordingly, at age 50, a total of 46% in the GP group had a higher education, compared to around 23% in the younger OHC and CWC groups, 14% in the teen OHC group, and 19% in the teen CWC group.
Associations between child welfare involvement and having a higher education at age 50. Results from KHB binary logistic regression analysis (n = 13,094).
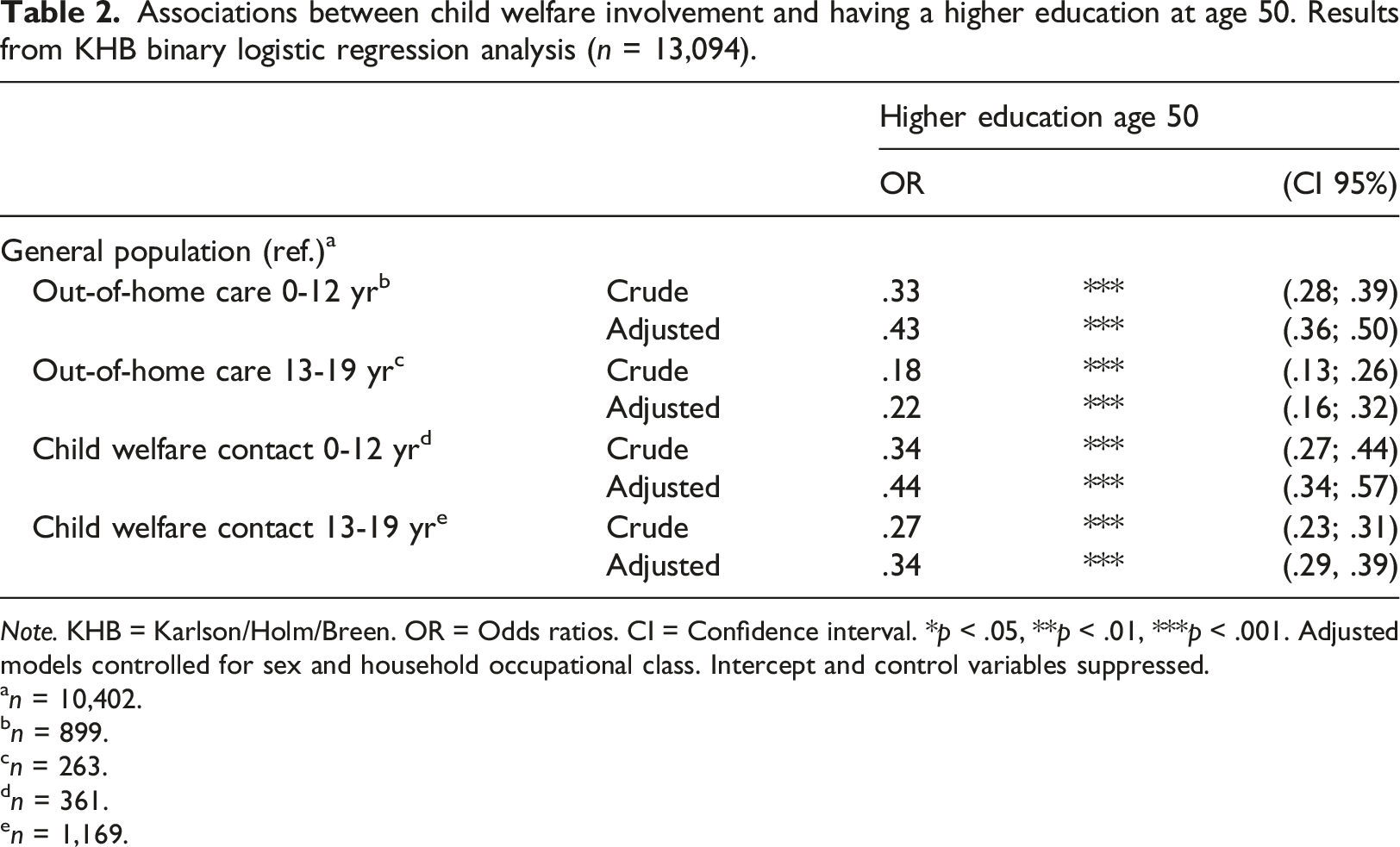
Note. KHB = Karlson/Holm/Breen. OR = Odds ratios. CI = Confidence interval. *p < .05, **p < .01, ***p < .001. Adjusted models controlled for sex and household occupational class. Intercept and control variables suppressed.
an = 10,402.
bn = 899.
cn = 263.
dn = 361.
en = 1,169.
Results from the pairwise comparisons across the different types of child welfare involvement showed that the odds of having a higher education at age 50 did not significantly differ between the younger OHC and the younger CWC groups (p > .10, estimates not shown in table). The teen OHC group, however, had around 33% lower odds (OR = .67, p < .05) compared to the teen CWC group (not shown in table).
Associations between child welfare involvement and the timing of a higher education completion across the life course. Results from KHB multinomial logistic regression analysis (n = 5,348).
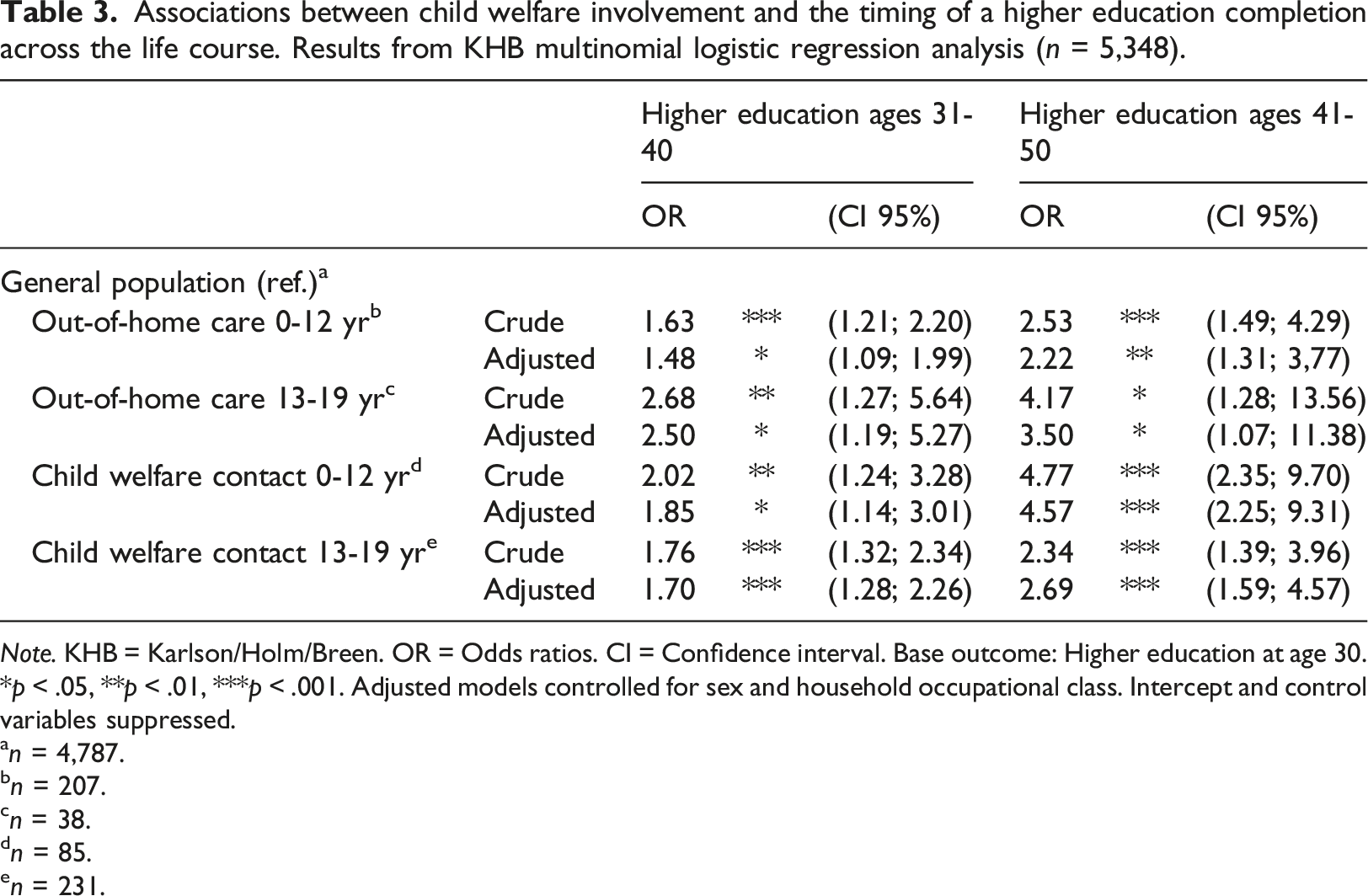
Note. KHB = Karlson/Holm/Breen. OR = Odds ratios. CI = Confidence interval. Base outcome: Higher education at age 30. *p < .05, **p < .01, ***p < .001. Adjusted models controlled for sex and household occupational class. Intercept and control variables suppressed.
an = 4,787.
bn = 207.
cn = 38.
dn = 85.
en = 231.
Lastly, although there was a trend towards earlier higher education completion in the younger OHC group in comparison to the younger CWC group, the pairwise comparisons showed no statistically significant difference between completion at either ages 31–40 (p > .10) nor ages 41–50 (p > .10) instead of completion at age 30. Conversely, there was a trend towards later completion in the teen OHC group as compared to the teen CWC group, but the timing of higher education completion did not significantly differ between these two groups either (p > .10 respectively, estimates not shown in table).
Discussion
This study examined OHC experienced individuals’ chances of having a higher education in midlife (age 50) and whether the timing of completion differed between them and their general population peers as well as a group of individuals who had come in contact with the child welfare system without being placed in care. First of all, the results showed that individuals placed in OHC were less likely to have a higher education in midlife in comparison to their general population peers. This is in line with previous findings of OHC experienced individuals’ educational attainment in young adulthood (Gillum et al., 2016; Gypen et al., 2017; Jackson & Cameron, 2014; Kääriälä & Hiilamo, 2017). This was particularly true for those with a first-time placement in their teens, that is a group of children mainly placed due to own behavior as opposed to those in the younger OHC group, which were mainly placed due to family circumstances. This too reflects previous studies (O'Higgins et al., 2017). The key finding, however, is that the number with completed higher education did increase over time. Moreover, among those who had a higher education, individuals who had experienced OHC were more likely to have completed it after the age of 30 and even more so after the age of 40. The current study thus confirms previous indications of a delayed pursuit of higher education completion among individuals who have been placed in OHC in studies based on qualitative data and quantitative studies with shorter follow-ups (Brady, 2020; Day et al., 2013; Harrison, 2020). The study also extends prior studies by suggesting that they may experience educational recovery over the life course. Furthermore, the association between OHC experience and completion later in life was even stronger among those first placed as teenagers.
Children placed in OHC, tend to come from disadvantageous backgrounds, which in turn may affect their educational outcomes (O'Higgins et al., 2017). To account for selection processes underlying a placement, we included alternative comparison groups consisting of those who came in contact with the child welfare system without being placed for the first time before the age of 13 and as teenagers, respectively. Descriptive statistics showed that these groups were similar in terms of household occupational class, but females were underrepresented in both CWC groups. Previous studies which have compared children in OHC to children from similar backgrounds (e.g. children who have received in-home services) have reported mixed results (e.g. Sinclair et al., 2020; Vinnerljung et al., 2010; Wall-Wieler et al., 2019). In the current study, the chances and timing of higher education in the younger CWC group were overall similar to the younger OHC group. The teen OHC group was less likely to have a higher education at age 50 in comparison to the teen CWC group, but the timing of higher education completion was similar. Irrespective of a placement, children who come in contact with the child welfare system thus seem to exhibit similar educational pathways.
We know from general educational research that socioeconomically disadvantaged and marginalized groups are more prone to delay higher education completion (Bozick & DeLuca, 2005; Milesi, 2010). Moreover, previous studies have shown individuals who have experienced OHC face many challenges in their transition into adulthood, including obstacles related to higher education completion (Geiger & Beltran, 2017; Gillum et al., 2016; Häggman-Laitila et al., 2019). By this background, it might be reasonable to expect that individuals who have been placed in OHC would be educationally left behind in their twenties and early thirties. While this study indicates that their attainment to some extent improves over the life course, there are likely costs and lower returns associated with such delays. Taken together, this may call for specific support to individuals who have experienced OHC. Independent living services may support their educational progress during their transition to adulthood (Kim et al., 2019). Campus-based programs may also hold promise in supporting a more on-time completion (Geiger & Beltran, 2017; Randolph & Thompson, 2017).
However, in terms of higher education completion, the term ‘better late than never’ can be applied. Qualitative life course studies have identified a wide range and diversity in OHC experienced individuals’ educational trajectories to higher education later in life (e.g. Brady & Gilligan, 2019). Regardless, the possibilities of such pursuit are dependent on the educational system’s tolerance for educational late blooming (Levin & Levin, 1991; Pallas, 2003). As previously noted, the Swedish educational system, which is the context of the current study, does not include policies specifically targeting individuals who have been placed in OHC. It is, however, known to be an inclusive system with general policies which allow for alternative pathways into higher education and reduced costs for attendance (Halldén, 2008). Hence, the educational recovery over the life course exhibited in both the OHC and CWC groups might be partly attributed to the characteristics of this system. This implies that education polices directed at reducing educational inequality, such as adult education and reduced costs for higher education, may benefit individuals, who in one way or another have been involved with the child welfare system, in their efforts of making up for lost ground.
Strengths and limitations
To the best of our knowledge, this is the first study to examine OHC experienced individuals’ chances and timing of higher education completion over a 50-year follow-up. We used comprehensive longitudinal data on a birth cohort which includes a large number of individuals with OHC experience. The data furthermore enabled us to differentiate between individuals who have experienced OHC based on their first-time placement. Moreover, they could not only be contrasted to their general population peers, but also to children who were investigated by the child welfare system without being placed – that is children whom are more alike on both observable and unobservable factors.
However, the longitudinal design also has some inherent limitations in terms of generalizability and comparability of measurements across time. In Swedish child welfare, family preservation has attained a stronger focus and the tendency to place children in OHC has declined since the upbringing of the current cohort. Hence, it could be expected that children placed today represent an even more selected group. Due to societal changes they would also be expected to be more diverse with regards to cultural or migration backgrounds. This might imply that today’s children in OHC are more educationally disadvantaged compared to their general population peers and to children with other types of child welfare involvement. The 1953 cohort grew up in a time of educational expansion, but the characteristics of the Swedish educational system during their adulthood were largely the same as it is today. It therefore seems likely that younger cohorts of individuals who have been placed in OHC and other disadvantaged groups also pursue higher education later in life in comparison to the general population. Nonetheless, more studies on younger cohorts and from different contexts are needed to confirm the generalizability of the findings in this study.
Other limitations needed mentioning are related to the data. As already noted, there are differences in how higher education was recorded in the two registers used. This may have resulted in an underestimation of higher education completion at age 30, and consequently, an overestimation of completion rates at ages 31–40. However, such potential data limitation would affect all cohort members, across all study groups, equally. The relative differences between cohort members can thus be expected to be stable. Nonetheless, yearly data throughout the follow-up would have provided a more detailed picture of the timing. Additionally, we lack data on alternative pathways to higher education, any internal education from employers as well as enrollment rates. Information on enrollment would have enabled us to study those who may have started without completing their education as well as the progression and periods of stopping out along the way.
Another limitation is the lack of insights into characteristics associated with higher education completion at different times over the life course, in other words, what separates the early bloomers from the late bloomers and from the vast majority that did not have a higher education. However, by creating two OHC groups based on their first-time placement, we have been able to shed some light on how placement characteristics can be related to different educational pathways.
Conclusions
Delayed higher education completion and educational late blooming seems to be more common for OHC experienced individuals, and those first placed as teenagers in particular, than for their general population peers. However, individuals who have experienced OHC seem to exhibit similar educational trajectories as individuals who were investigated by the child welfare services but never placed. Although the evidence base substantiating the effectiveness of specific support to individuals who have been placed in OHC is scarce (Evans et al., 2017; Geiger & Beltran, 2017; Randolph & Thompson, 2017), such programs may still increase the numbers that complete their education in young adulthood. More general inclusive education polices can allow more individuals with OHC experience and other types of child welfare involvement to engage in life-long learning.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Vetenskapsrådet; 2017–01476.