
Abstract
Children and young persons (CYPs) in out-of-home care often demonstrate a variety of needs resultant from their early adverse experiences and complex family backgrounds. In Singapore, the Child and Adolescent Needs and Strengths (CANS) assessment tool is used to capture the individual’s needs and strengths for case planning. This study had two aims: first, it sought to test whether CYPs who entered residential care with higher level-of-care (LoC) scores on the CANS tool, indicative of higher needs or more intensive services required, were more likely to experience a critical incident. Second, it aimed to test the various needs separately with the occurrence of critical incidents to delineate the impact of each individual need on critical incident. Using a sample of 488 CYPs aged between 5 years and 17 years who were residing in 13 voluntary children’s homes in Singapore, the study found that 46.3% of the sample had experienced a critical incident. The results showed that CYPs with higher LoC scores were more likely to have a critical incident, although this comparison was only significant between the lowest and highest LoC scores. Child-related issues such as the presence of self-harm and risk of suicide, behavioral problems, emotional problems, sexual behavior, delinquency, and poor caregiver bond at entry to residential care were also observed to be significantly associated with the occurrence of critical incidents. The findings and implications are discussed accordingly.
Introduction
Critical incidents among children and young persons in out-of-home care
Children and young persons (CYPs) in welfare systems often present with a wide variety of needs stemming from the financial and traumatic experiences they have gone through with their families (August, Realmuto, & Gewirtz, 2007). Subsequently, these CYPs have a higher tendency to exhibit physical, cognitive, emotional, behavioral and social problems, as well as mental health issues (Halfon, Mendonca, & Berkowitz, 1995; Perry, 2001; Price-Robertson, Rush, Wall, & Higgins, 2013). To further intensify the situation, CYPs in out-of-home care who experienced critical incidents (e.g., aggression, property damage, and self-harm) have been reported to have longer admissions and poorer outcomes (Barton, Rey, Simpson, & Denshire, 2001).
To date, there is a paucity of research that relates to the factors that are likely to bring about critical incidents among CYPs in out-of-home care. It is important to study the factors that are associated with the occurrence of critical incidents in these CYPs to promote better child outcomes in residential care. The concept of critical incident in the current article refers to the observable occurrences of a child’s behavior and functioning that do not meet the rules and standards of society and/or that lead to the welfare of the child being compromised. Some examples of critical incidents may include physical harm to self or others, acts of delinquency, mental health issues, behavioral problems, and emotional problems.
Factors that contribute to critical incidents
Childhood experiences play an important role in contributing to CYPs growth and development and may have lasting consequences that affect the child’s life into adulthood (Gilbert et al., 2009).
Traumatic experiences can contribute to the occurrence of critical incidents. When a child experiences maltreatment (e.g., physical, sexual, emotional abuse, or neglect), it can cause detrimental effects like mental health problems, increased likelihood of substance use, increased risk-taking and self-harm behaviors, and criminal-related acts (Gilbert et al., 2009; Miller, Esposit-Smythers, Weismoore, & Renshaw, 2013). These detrimental effects and its negative consequences can potentially last into adulthood. In particular, teachers and mothers reported that children who were physically maltreated before the age of five exhibited higher levels of internalizing and externalizing behaviors compared to children who were maltreated at an older age (Keiley, Howe, Dodge, Bates, & Pettit, 2001). In addition, when parents experienced conflict with the law or incarceration, their children and adolescents have also been reported to exhibit increased antisocial behaviors that violated societal norms or to have conduct problems (e.g., persistent lying, delinquency, and fighting) (Boch & Ford, 2018; Murray, Farrington, & Sekol, 2012). The negative effects that arise out of childhood maltreatment and traumatic experiences contribute to the occurrence of critical incidents.
The environment and quality of relationships that CYPs develop while growing up can also affect the occurrence of critical incidents. CYPs are more likely to have behavioral problems and get into trouble with the law when they come from dysfunctional families. Juvenile offenders are often found to have poor communication with their parents and lack attachment with their families (Choi & Lo, 2004). The lack of parental involvement and supervision is evident as parents are often unaware of their child’s behavior and actions until their child’s arrest. Apart from antisocial behavior and conduct problems, dysfunctional relationships and the lack of communication within the family may also lead adolescents into engaging in self-harm behaviors (Brown & Plener, 2017; Yates, 2004). Besides external factors, adolescents are also more likely to engage in self-harm behaviors when they have internal issues such as mental health problems (e.g., depression, anxiety), suicidal ideation, need for attention, and poor emotional regulation (Brown & Plener, 2017; Jacobson & Gould, 2007; Yates, 2004). Therefore, it is critical to identify the needs and experiences of CYPs to provide the appropriate support and reduce the risk of critical incidents occurring in the out-of-home care setting.
Overview of Singapore’s out-of-home care setting
Singapore is an independent island state in Southeast Asia with a total population of 5.6 million according to Singapore Department of Statistics (DOS, 2017). The Ministry of Social and Family Development (MSF) bears the statutory responsibility of protecting children from abuse and neglect in Singapore under the Children and Young Persons Act (2013). When placement in kinship care is not possible, CYPs are placed in the out-of-home care setting, which comprises either foster care or one of the 19 voluntary children homes (VCHs) across the island. VCHs are residential care facilities operated by voluntary welfare organizations which receive government funding to provide shelter, care, and services for CYPs. As of 2016, there were 430 CYPs in foster care, whereas 643 CYPs were placed in residential care (MSF, 2017).
Understanding the needs of children and adolescents
CYPs in the out-of-home care have often undergone a series of events that led them to being moved out of living with their families. Thus, they have a complex set of needs that are related to their experiences. Early identification of their needs and the provision of evidence-based interventions are crucial for reducing the occurrence of critical incidents, maintaining the positive effects of successful interventions (Guralnick, 1997; Sim, Li, & Chu, 2016) and ensuring the healthy development of these vulnerable children into adulthood (Cicchetti & Toth, 2000).
The Child and Adolescent Needs and Strengths (CANS) tool is designed as an objective, evidence-based communication tool to provide a common language for professionals across multiple disciplines to communicate about each child’s severity of needs and the utility of their strengths. The CANS tool can be used to facilitate case workers in decision-making for appropriate services and placement to enhance service delivery and support systemic improvements to child welfare services to achieve optimal child outcomes in the long-term (Lyons, Weiner, & Lyons, 2004; Winters, Collett, & Myers, 2005).
Adaptation of the CANS tool for Singapore
The CANS assessment tool was originally developed in the U.S. and has been used across many states in America for child welfare services and other sectors such as mental health monitoring, screening for risks of developing trauma symptoms, and placement decisions in the juvenile justice systems (Dunleavy & Leon, 2011; Fawley, Shalla, Griffin, & Lyons, 2004; Griffin et al., 2011; Kisiel, Fehrenbach, Small, & Lyons, 2009; O’Donnell & Lurigio, 2008; Stoner, Leon, & Fuller, 2015).
In Singapore, the CANS assessment tool was adapted and localized to assess the needs and strengths of CYPs, facilitate case management, and track the progress and occurrence of critical incidents in the out-of-home care setting. For example, the CANS tool has identified that CYPs placed in residential care generally had higher needs compared to CYPs in foster care and that the needs of CYPs varied with their age (Liu et al., 2014). In addition, local research has also identified that higher strengths identified at baseline was predictive of lower needs in CYPs 1 year later in multiple areas such as behavioral and emotional needs and general life functioning (Sim et al., 2016). With these, the tool is able to profile the needs of CYPs and guide decisions on service provision with the hope to reduce the critical incidents experienced.
In addition to the individual CANS rating scale, a localized version of the CANS levels-of-care (LoC) algorithm was also developed to differentiate CYPs with different levels of need in the Singaporean context as the out-of-home care CYPs had demonstrated a much lower prevalence of risky behaviors, as well as behavioral and emotional problems compared to those in the U.S. (Liu et al., 2014). The LoC algorithm classifies CYPs into three levels to determine the complexity of needs and intensity of care required by a child: high, moderate, and low.
In Singapore, the child’s placement decisions and the intensity of services are then allocated in accordance to the tier of LoC assigned to the CYPs. Research found that adolescents assigned to residential placements concordant with CANS LoC recommendations were reported to experience more positive changes over time, especially in behavioral and emotional problems (Chor, McClelland, Weiner, Jordan, & Lyons, 2012). With the use of LoC, the progress of CYPs can be tracked to assess whether different service providers and various interventions programs are effective at improving child outcomes, such as a reduction in the occurrence of critical incidents. This provides an objective recommendation for placement decisions and service planning by state workers and providers (FFTA, 2005).
Current study and aims
The earlier years following the successful adaptation of CANS assessment tool focused on understanding the profiles of clients in out-of-home care (Liu et al., 2014; Sim et al., 2016). Thus far, there has been no study which examined the relationship between CANS LoC with child outcomes such as the occurrence of critical incidents during their residential stay.
The first aim of this study was to examine whether CYPs with a higher CANS LoC were more likely to experience a critical incident. As a higher CANS LoC is indicative of higher needs, it was expected that higher LoC would be associated with greater instances of challenging behaviors and critical incidents that required remedial action or interventions (Daleiden, 2004; Osborn & Bromfield, 2007).
In addition to only relying on CANS LoC as a predictor of critical incidents in out-of-home care, the second aim of this study was to examine the associations of individual child issues, prior or at point of entry to the VCH, with the occurrence of critical incidents. This enables us to delineate the impact of each issue with critical incidents. It was expected that CYPs with a history of traumatic experiences, poor relationships, and behavioral problems were at a higher risk of critical incidents (Barton et al., 2001; Gilbert et al., 2009; Miller et al., 2013).
Method
Participants
The present study obtained data from 13 VCHs (of the 19 VCHs) in Singapore. These VCHs were selected based on their willingness to participate in the study. Of these 547 CYPs from 13 VCHs, we excluded 59 (10.8%) CYPs who were not between the age of 5 years and 17 years and those without a complete CANS assessment. This resulted in a total of 488 (89.2%) CYPs for the final analysis. Ethics approval was obtained from the MSF Singapore before the commencement of the study.
Measures
CANS tool Singapore version
In this study, the Singapore version of CANS tool was used. The Singapore CANS tool as well as the algorithm to determine an individual’s LoC were adapted by a group of experienced Singaporean psychologists and child protective professionals in close consultation with Dr. John Lyons who developed the tool. The algorithm takes into consideration an individual’s needs from a wide range of domains. Details of the Singapore version CANS tool have been previously described (Liu et al., 2016). The tool consists of seven domains (i.e., life functioning, school, child behavioral and emotional problem, trauma, child risk behavior, strengths, and caregiver). Within each domain, each item used a four-level rating system to classify different levels of need. These ratings indicated different actions ranging from 0 (no evidence of a need and no need for action), 1 (mild degree of need and the need for monitoring or prevention), 2 (moderate need which requires action), to 3 (severe need requiring immediate or intensive action). Ratings of 0 and 1 were classified as nonactionable needs, whereas ratings of 2 and 3 were classified as actionable needs (Liu et al., 2016). The reliability of the Singapore CANS tool has been examined and previously reported (Liu et al., 2016). For each CYP entering care, the CANS assessment was performed at the point of entry to the VCH.
Self-harm or suicide risk was defined as present if CANS items “self-harm” and/or “suicide risk” were rated as 2 or 3. Behavioral problem was defined as present if any of the items (i.e., hyperactivity, oppositional, conduct, and substance use) in the CANS behavioral needs domain was rated as 2 or 3. Emotional problem was defined as present if any of the items (i.e., psychotic symptoms, depression, anxiety, eating disturbance, anger control, and adjustment to trauma) in the CANS emotional needs domain was rated as 2 or 3. Sexual behavior was defined as present if the CANS items “sexual aggression” or “sexually reactive” were rated as 1, 2, or 3. Delinquency was defined as present if the CANS item “delinquency” was rated as 1, 2, or 3. Caregiver bond was defined as present if any of the following items in the caregiver domain was rated as 2 or more: (1) supervision, (2) child’s bond with caregiver, (3) involvement with care, (4) empathy for child, and (5) knowledge.
LoC score
Singapore’s CANS LoC algorithm is a localized version of the LoC algorithm adopted from the U.S. (Lyons et al., 2004). In brief, the determination of CANS LoC score was computed based on a combination of CANS items from the domains (excluding the caregiver domain). It takes into account multiple aspects of a child’s needs including (but are not limited to) areas such as life functioning and risk behaviors. There are three LoC: LoC 1 represents low needs/basic services, LoC 2 represents moderate needs/services, and LoC 3 represents high needs/intensive services. Hence, a higher LOC rating would indicate that the individual had more actionable needs requiring more intensive or immediate action.
Critical incident
To code for the occurrence of critical incidents, data extraction was focused on identifying difficult and unacceptable behaviors and the negative consequences recorded in each child’s case files. Critical incidents that occurred within the 4 years following the CYP’s baseline CANS assessment were obtained from each CYP’s file.
The technique used to code critical incidents in this study was adopted from the critical incident technique method developed by Flanagan (1954). Previously, it had been used in the field of social work (Mills & Vine, 1990) and residential care (Wong, Skitmore, Buys, & Wang, 2014) and had also been utilized as an outcome measure in a study on intervention effectiveness (Nunno, Holden, & Leidy, 2003). Critical incidents were collected from behavioral inventories such as the Child Behavior Checklist, the Teacher Report Form, and the Child Hostility Inventory.
In this study, a critical incident was defined as the first occurrence of any of the following events: (1) health-related event (e.g., surgery, asthma attacks), (2) mental health-related event (e.g., psychotic symptoms, admission for mental-related purposes), (3) family-related event (e.g., death of child’s primary caregiver, abandonment, severe negative influences), (4) sexualized behavior perpetuated by the CYP under the age of 16 years or sexually aggressive behavior perpetuated by a CYP of any age, (5) physical harm to others or destroying of property as an act of aggression/anger, (6) self-harm (e.g., attempted suicide, wrist cutting, refusing to eat), (7) delinquency (e.g., theft, vandalism, rioting, loansharking, and drug use), (8) emotional bullying (e.g., constant insulting and spreading rumors), and (9) unacceptable behavior such as disobeying home rules, tantrums, or lying that warranted punishment by an authority figure in various settings (i.e., school, residential care, and home).
Placement breakdown
Placement breakdown referred to the breakdowns of care placement that were premature and unintentional. This included placement breakdowns that occurred before or after a critical incident. Specifically, history of placement breakdown was defined as breakdowns of care placement prior to the occurrence of critical incidents. This was a binary variable consisting of “Yes, experienced breakdowns” or “No breakdowns.”
Demographic information
Information on children’s demographic characteristics was obtained using a standardized questionnaire administered by trained caseworkers. Age was defined as the age at the time of assessment. Duration of follow-up was calculated from the date of discharge or date of study closure (December 31, 2015) minus the date of entry into VCH.
Covariates
Number of service(s) was defined as the number of services/interventions used before the occurrence of a critical incident. These services and/or interventions were aimed at addressing a particular behavioral/psychological/emotional/traumatic issue faced by the child that was undertaken by a professional in regular and structured sessions. The services used were not limited to the VCH but also extended to external settings, such as at schools, hospitals, or family service centers in the community. Number of trauma(s) experienced by a child was defined as the number of items (i.e., neglect, physical abuse, emotional abuse, sexual abuse, domestic violence, medical trauma, or other trauma) with a rating of 1, 2, or 3. Number of strength(s) was defined as the number of strength items on the CANS tool with a rating of 0 or 1.
Procedure
The CANS assessments of the CYPs were completed between October 2011 and March 2013. Ratings were completed by caseworkers and researchers trained and certified in the CANS tool, who obtained the necessary information through the review of case files and interviews with relevant professionals. An examination of a randomly drawn sample of 130 cases revealed good to excellent levels of inter-rater reliability for the CANS ratings among all raters (i.e., intraclass correlations [ICCs] between .79 and .89). Additional demographic information was also obtained from the CYPs’ case files and interviews with their caseworkers.
Information on critical incidents and placement breakdowns was coded from incident reports obtained from VCHs across Singapore, as well as CYPs’ individual case files and electronic case management records (cut-off date in December 2015). These incidents and breakdowns occurred within the 4 years following each CYP’s CANS assessment (cutoff at December 31, 2015). An examination of a random sample of 55 cases yielded moderate levels of inter-rater reliability (i.e., ICCs between .58 and .60; κ values between .59 and .68).
Plan of analysis
All statistical analyses were performed using STATA statistical software (Version 10; StataCorp, College Station, Texas, USA). We compared the baseline characteristics of those with critical incident and those without by employing the χ2 test or by t-test where appropriate. We compared the baseline characteristics of CYPs by CANS LoC score by employing one-way analysis of variance or Kruskal–Wallis where appropriate.
Cox regression was performed to examine the association between CANS items and CANS LoC score with critical incident. We examined the associations in two models: (i) age, gender, race, and (ii) additionally adjusted for duration of follow-up, number of strength(s), number of trauma(s) experienced, history of placement breakdown, and number of service(s) used before the occurrence of critical incidents.
Results
With a median follow-up time of 2.8 years (i.e., the baseline CANS assessment was conducted between 2011 and 2013, with a follow-up of the CYP’s residential stay until December 31, 2015), 226 (46.3%) CYPs experienced a critical incident. The baseline characteristics of the CYPs are summarized in Table 1. The average age of the CYPs was 11.89 years, and slightly over half of the CYPs (51.0%, N = 249) in this sample were of Chinese ethnicity. Majority of the CYPs had a CANS LoC score of 1 (LoC 1: 335 [68.7%], LoC 2: 90 [18.4%], LoC 3: 63 [12.9%]). In addition, 43 (8.9%) of CYPs experienced a placement breakdown during this period of time. The distribution of the CANS LoC score for CYPs who experienced placement breakdown is 15 (34.88%) CYPs had LoC 1; 12 (27.91%) CYPs had LoC 2; and 16 (37.21%) had LoC 3. Of these, seven had a placement breakdown prior to a critical incident.
Baseline characteristics of CYPs of the study population.
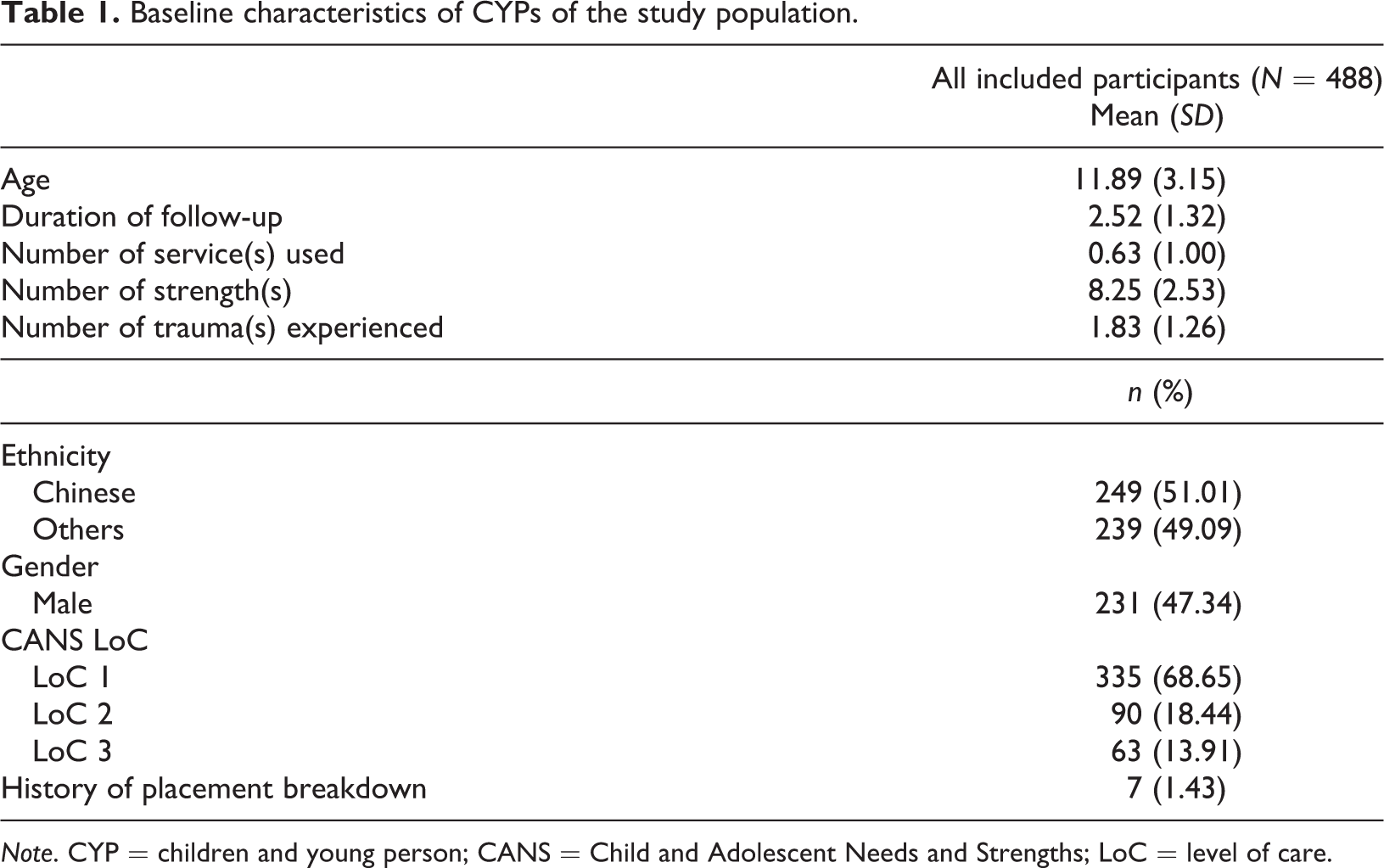
Note. CYP = children and young person; CANS = Child and Adolescent Needs and Strengths; LoC = level of care.
Table 2 compares the baseline characteristics of the CYPs who experienced a critical incident and those who did not. Compared to those who did not experience a critical incident, those who experienced a critical incident were more likely to be male, have a CANS LoC score of 3, have a longer follow-up duration at the VCH, and have experienced a placement breakdown prior to the occurrence of the critical incident. Further comparison of the baseline characteristics by gender is presented in Table 3. Results found that male CYPs were more likely to have a higher CANS LoC score compared to female CYPs.
Baseline characteristics of CYPs who did not experience a critical incident and those who had a critical incident.
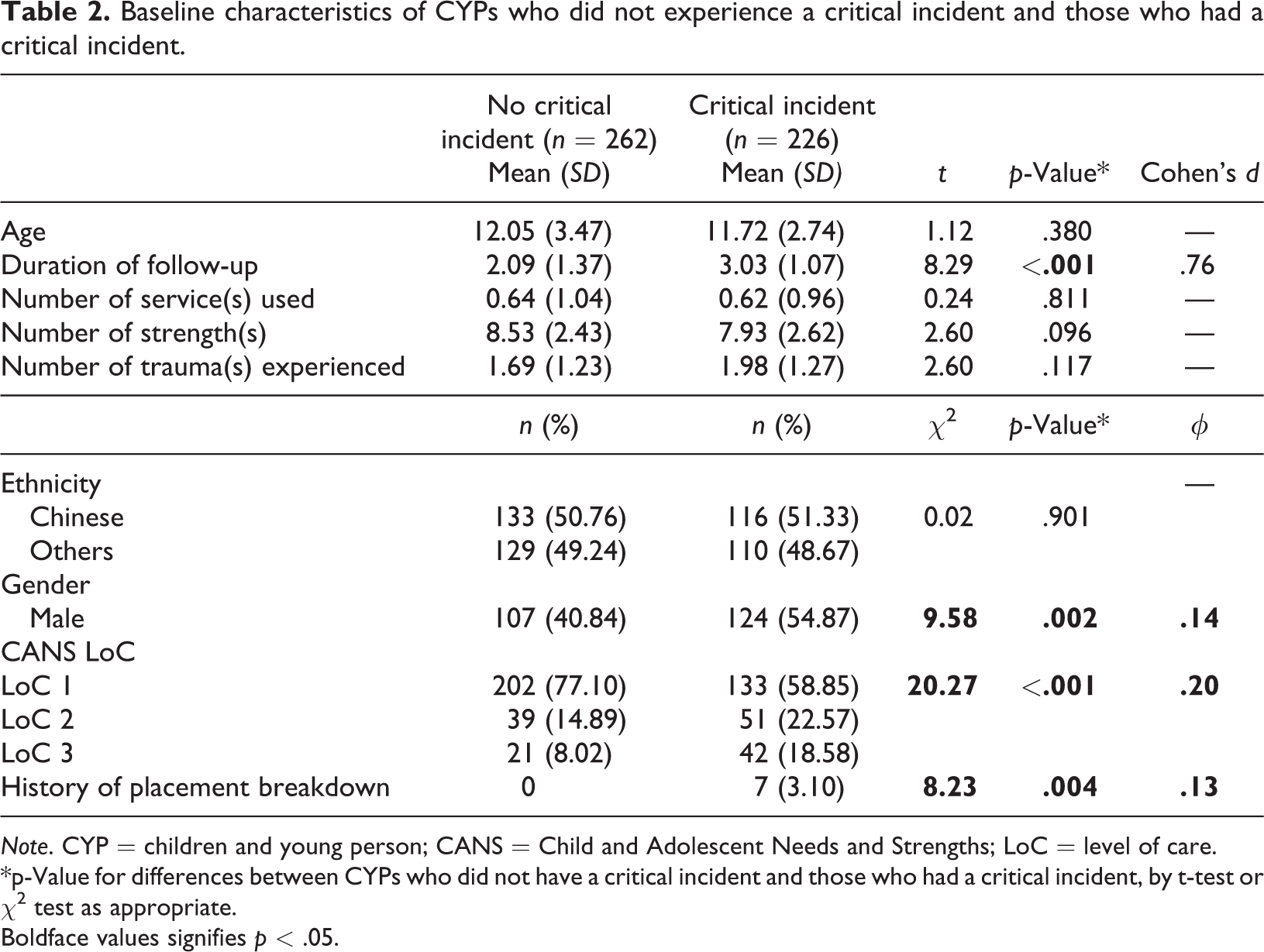
Note. CYP = children and young person; CANS = Child and Adolescent Needs and Strengths; LoC = level of care.
*p-Value for differences between CYPs who did not have a critical incident and those who had a critical incident, by t-test or χ2 test as appropriate.
Boldface values signifies p < .05.
Baseline characteristics of CYPs by gender.
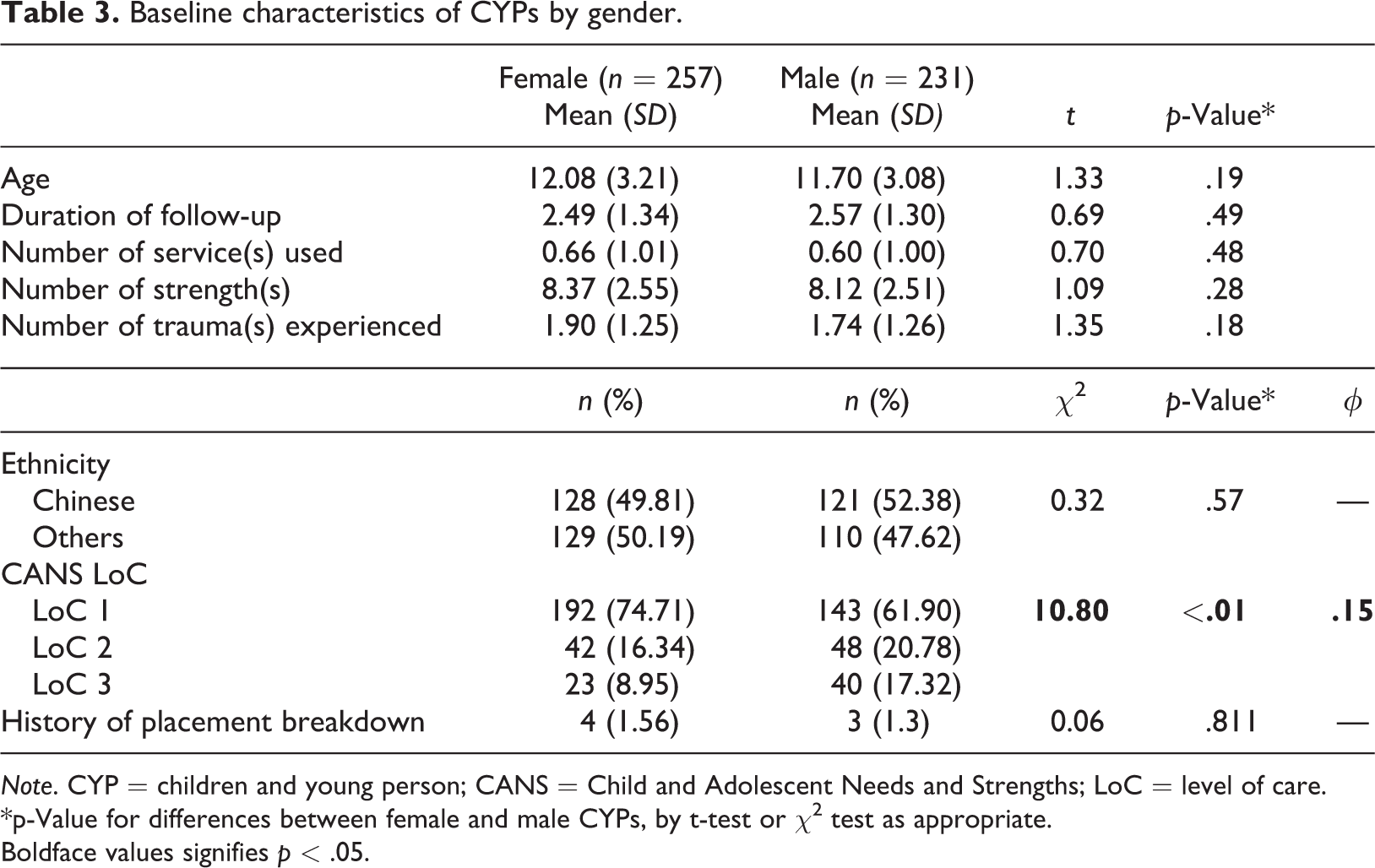
Note. CYP = children and young person; CANS = Child and Adolescent Needs and Strengths; LoC = level of care.
*p-Value for differences between female and male CYPs, by t-test or χ2 test as appropriate.
Boldface values signifies p < .05.
The breakdown of critical incidents by the different types of critical incidents and the CANS LoC score are shown in Table 4. CYPs with CANS LoC score 3 were more likely to have experienced a health-/mental-health-related event, sexualized behavior-related event, or physical harm as compared to CYPs with CANS LoC 1 or 2.
Breakdown of critical incident types by LoC.
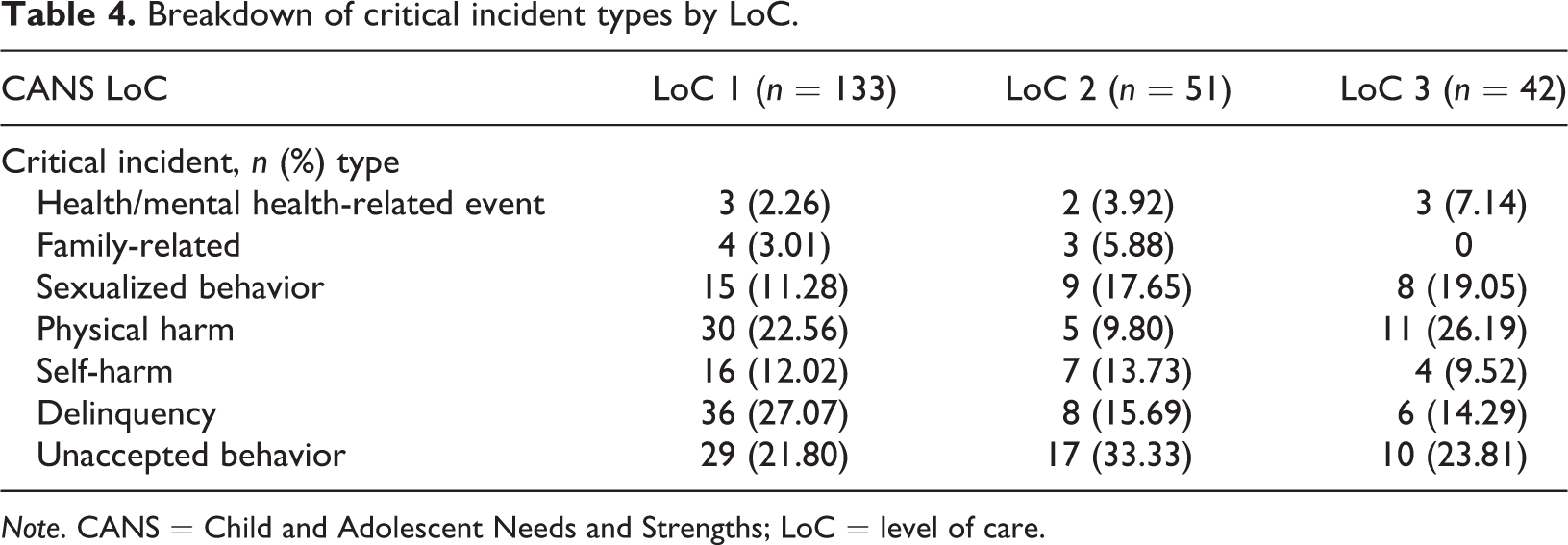
Note. CANS = Child and Adolescent Needs and Strengths; LoC = level of care.
Association of CANS LoC score with critical incidents
Table 5 shows the association of CANS LoC score with the occurrence of critical incidents in the population of CYPs staying in the VCH. After adjusting for age, gender, and race, CANS LoC score 3 was observed to be significantly associated with the occurrence of critical incidents. After further adjusting for duration of follow-up, number of strength(s), number of trauma(s) experienced, history of placement breakdown, and number of service(s) used before the occurrence of a critical incident, CANS LoC score 3 (hazard ratio [HR] = 1.72) was still observed to be significantly associated with the occurrence of a critical incident. When compared to CANS LoC 1, CYPs with CANS LoC score 2 was 1.22 times as likely to experience a critical incident (HR = 1.22, 95% CI = 0.86, 1.72). The lack of significant association between CANS LoC 2 with the occurrence of critical incidents could be limited by the small sample size.
Relation between LoC with critical incidents.
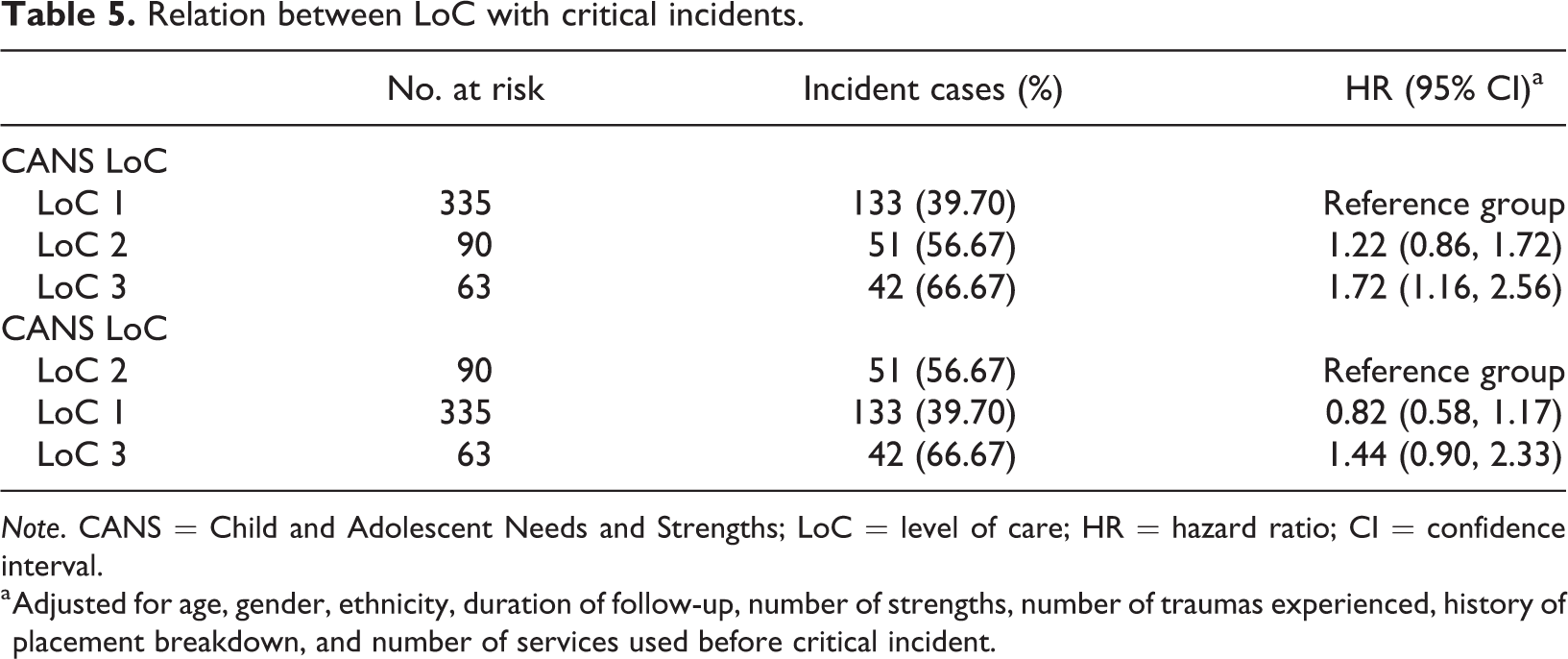
Note. CANS = Child and Adolescent Needs and Strengths; LoC = level of care; HR = hazard ratio; CI = confidence interval.
a Adjusted for age, gender, ethnicity, duration of follow-up, number of strengths, number of traumas experienced, history of placement breakdown, and number of services used before critical incident.
Associations of child-related issues with critical incidents
Table 6 shows the separate associations of child related issues, as measured by individual CANS items, with critical incidents in the population of CYPs staying in the VCH. After adjusting for age, gender, ethnicity, duration of follow-up, number of strength(s), number of trauma(s) experienced, history of placement breakdown, and number of service(s) used before the occurrence of a critical incident, self-harm and suicide risk (HR = 2.50), behavioral problem (HR = 1.96), emotional problem (HR = 1.49), sexual behavior (HR = 1.60), delinquency (HR = 1.56), and poor caregiver bond (HR = 1.41) were still observed to be significantly associated with the occurrence of critical incidents.
Relation between child-related issues and risks with incident cases.
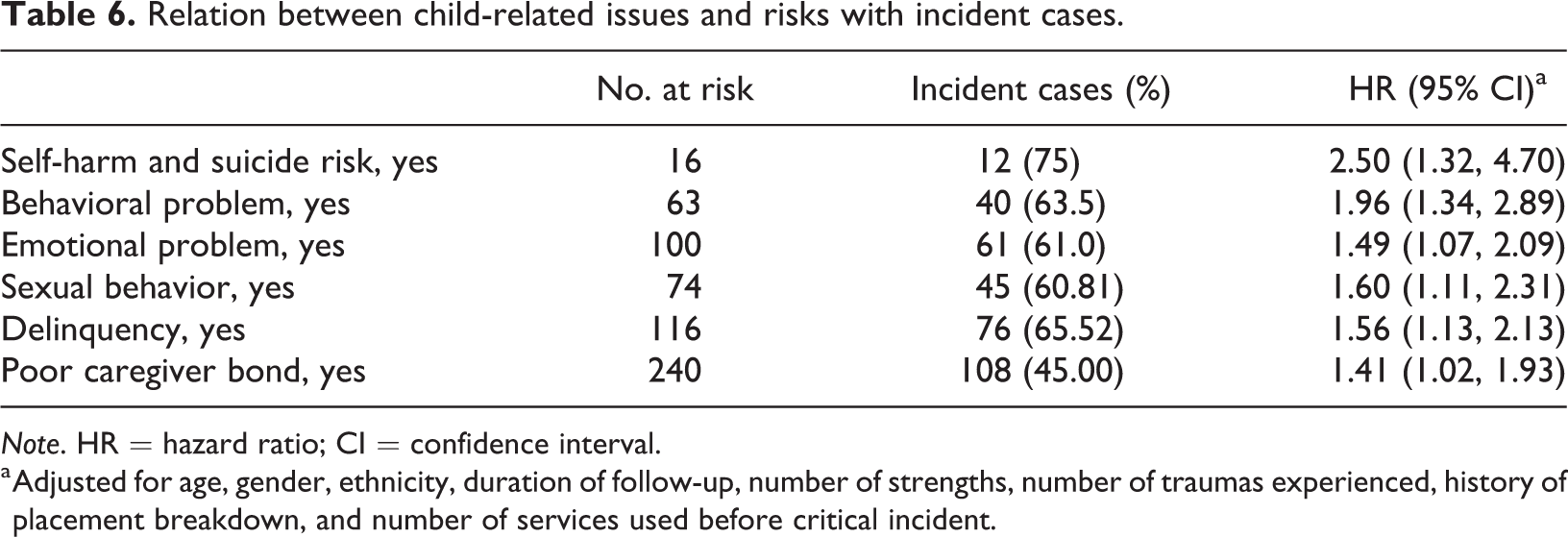
Note. HR = hazard ratio; CI = confidence interval.
a Adjusted for age, gender, ethnicity, duration of follow-up, number of strengths, number of traumas experienced, history of placement breakdown, and number of services used before critical incident.
Discussion
The current study is the first in examining the association between CANS LoC and individual needs with the occurrence of critical incidents during CYPs’ residential stay. The first aim was to investigate whether CYPs with higher CANS LoC were more likely to experience a critical incident. The results demonstrated the expected descriptive pattern that with each increase in LoC, a higher proportion of CYPs was found to undergo critical incidents. A statistically significant difference was only found between CYPs with CANS LoC 3 and LoC 1, in that those with LoC 3 were almost twice as likely as compared to LoC 1 to have critical incidents. Although no significant differences were found in the comparisons between the other LoC, the directionality was as expected, in that CYPs with higher LoC had hazard ratio of greater than 1 (i.e., a higher likelihood of critical incidents) as compared to those with lower LoC. These results imply the utility of the CANS tool in Singapore to assess the problems and needs of each child entering into out-of-home care to support care planning and decision-making and to allow for the monitoring of outcomes of services. CYPs with higher LoC are more in need of intensive remedial actions as there is a higher likelihood of a poor outcome.
The second aim of this study was to examine the associations of individual child issues, which were assessed at point of entry to VCH, with the occurrence of critical incidents during their residential stay. The results demonstrated that CYPs who entered care with trauma, relational, and functional impairments, such as the presence of (1) self-harm and suicide risk, (2) behavioral problems such as impulsivity, oppositional, conduct, and/or substance use, (3) emotional problems such as psychotic, depression, anxiety, and/or anger control, (4) sexual behavior, (5) delinquency, and (6) poor caregiver bond, were more likely (i.e., between 1.4 and 2.5 times) to encounter critical incidents during their residential stay as compared to children who did not present with such problems.
These findings highlight the importance of early identification and adequate treatment programs at residential care to address the above issues so as to minimize the possibility of a critical incident in the residential stay. Evans and Scourfield (2017) demonstrated in a systematic review on self-harm and suicidal risk that suicide attempts were more prevalent with CYPs in care, with those in care being more than three times as likely to make an attempt on their life. Although it is not known in the included studies whether suicidal and self-harm risk were present before the children entered care, this study demonstrated that there are CYPs who enter care with self-harm and suicidal risk in Singapore. Hence, there is a need to consider the adequacy of help for such CYPs. Improved access to information on suicide prevention and counselling channels could be provided to residents in care, with the provision of adequate training for professionals to identify risk and to be knowledgeable of the various avenues for timely support and help. However, suicide prevention interventions that are specific to the needs of CYPs in care still require development.
Considering that youth in residential care have demonstrated significantly higher rates of functional impairment across domains of behavior problems, delinquency, substance use, suicide, and attachment issues (Briggs et al., 2012; Stewart et al., 2010), this study further showed that critical incidents were more likely for CYPs in out-of-home care who had behavioral, emotional, sexual, and delinquency issues as compared to those who entered care without such issues. This result remained even after controlling for the services or interventions which the child had or was undergoing. This finding may indicate a need for a deeper examination of the services or interventions provided: is the referral or administration of intervention conducted in a timely manner, and is the dosage of treatment adequate in relation to the severity of need? Additionally, Boyer, Hallion, Hammell, and Button (2009) demonstrated that the number and types of trauma that the youth were exposed to prior to residential placement was negatively associated with positive residential treatment outcomes.
For CYPs who enter out-of-home care with high behavioral, psychological, and emotional problems, intensive and time-limited care in the form of therapeutic residential care may be needed. This is a type of specialist care which builds on a foundation of shared principles (Whittaker et al., 2016) that involves the planful use of a purposefully constructed, multi-dimensional living environment designed to enhance or provide treatment, education, socialization, support, and protection to children and youth with identified mental health or behavioural needs in partnership with their families and in collaboration with a full spectrum of community-based formal and informal helping resources. (Whittaker, Del Valle, & Holmes, 2014, p. 24)
Limitations and future research
The current study is not without limitations. The first limitation lies in the limited sample size, and hence the limited statistical power. A larger sample size would have allowed for better precision in analyses. For example, the outcome variable of critical incidents could be unpacked into the various types and tested individually in analyses to achieve more fine-grained findings and implications. However, this was not possible in the current study due to the small sample size for each type of critical incidents. A second limitation lies in that not all participants in the current study had completed their residential stay. Thus, the prevalence of critical incidents and placement breakdowns may increase with a sample of closed residential cases. A larger sample would have allowed for an investigation of only the completed cases for more robust findings. Future studies can include other outcomes pertinent to residential care, such as reentry into out-of-home care. This will shed insights on the sensitivity of CANS to other outcomes in addition to those tested in this study. Lastly, future studies should also seek to understand the mediating pathways in which functional impairments, behaviorally and emotionally, lead to a critical incident. For example, the risk for delinquency appears to be mediated by the level of deviance a peer has upon entry into a group facility, the number of deviant peers present, and the length and amount of deviant peer exposure one has. A moderately deviant child is most susceptible to become entrenched in delinquent friendship (Dodge & Sherrill, 2006).
Conclusion
This study provided preliminary insight into the utility of the CANS tool in Singapore as a useful measure of the needs of CYPs in residential care when linked to the outcome of critical incidents during their stay. The study also expounded on individual problems in a range of behavioral and emotional domains, present prior or at entry into care, that are more likely to lead to a critical incident during their residential stay. There is therefore a need for more intensive, timely, and targeted treatments for CYPs with higher LoC or those who have been identified with certain problems. Transition into residential care is often difficult for the child or youth due to separation from caregivers and the change in environment. Thus, services that provide sufficient support in critical transition periods and which involve the family may alter the trajectories of these children and youth, in hope that their problems prior to and at entry into care would not escalate to compromise their functioning and well-being in their residential stays.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.