
Abstract
Background
Surgical-and-Perioperative Risk Prediction Calculators (SPRPCs) help predict patients’ safety outcomes for proposed surgical procedures. These evidence-based assessments can inform shared decision-making between patients and providers – improving patient safety, satisfaction and care. However, evidence persistently indicates low use of SPRPCs in surgical care. We reviewed qualitative literature to explore surgeons’ and anaesthetists’ attitudes and perceptions of features of SPRPCs, facilitators, barriers and complexity influencing their adoption.
Method
A systematic literature search was performed across three bibliographic databases. A two-stage screening process was performed using pre-determined inclusion and exclusion criteria. The Joanna Biggs Institute (JBI) checklist was used to critically assess quality. Qualitative data from included studies were analysed using thematic synthesis.
Results
Four qualitative and two mixed-methods paper were included, reporting data from 72 clinicians in total. Three studies focused on orthopaedic surgery SPRPCs, two on the Surgical Perioperative Assessment System tool and one on post-anaesthetic care unit hypotension prediction. Six facilitator, and four barrier, themes were identified. SPRPCs were seen as valuable in lowering patients’ risk of harm and supporting: informed consent discussions, declining surgery, and staff communication. These benefits were contingent on SPRPCs being transparent, accurate and integrated with care pathways. Conversely, some argued SPRPCs do not change clinical decisions, pose a threat to autonomy and patient-centred care and open the clinician to legal liability.
Conclusions
SPRPCs are underutilised when developed without consideration of clinicians’ needs and workflow. Findings highlight the importance of clinicians’ involvement in SPRPC design. Further research would support improvements in their clinical adoption.
Introduction
Approximately 310-million major operations are performed each year globally, each being taxing financially and with potential risks to patient safety. 1 A crucial, challenging aspect of surgery decision-making involves prediction of major morbidity and mortality risk. 2 Clinicians must quantify and evaluate the potential risks when assessing patients for surgery and communicate these risks as part of effective risk counselling.2,3 Surgical and peri-operative risk prediction calculators (SPRPCs) help direct decisions about whether and how to proceed amongst surgical and non-surgical options by weighting different aspects of individual patient data that are known outcome predictors.2,4,5 Evidence suggests they reduce mortality rates, inpatient stays, and care requirements post-discharge.4,6 Likewise, benefits may also include reduction in human errors, improvement in standards for patient care, and cost-efficiency.5,7
Understanding the elements predicting surgical outcomes can facilitate discussions improving patient safety, anxiety, satisfaction and care.4,9–12 The adoption of SPRPCs may offer a framework to improve dialogue around patient surgical risk, thus improving shared decision-making, as well as enhancing clinician confidence in presenting risk-benefit analysis, thus reducing patient dissatisfaction.7,9,12–15
Evidence suggests that surgical trainees have adequate SPRPC knowledge, and that patients value their use in consultations, yet clinicians underutilise them, valuing personal knowledge and experiences more.2,4,9–12
Increasing understanding around clinicians’ views and attitudes towards the use of SPRPCs in surgical practice, and barriers to their use, would guide their future development and uptake. We therefore aimed to review qualitative evidence of clinicians’ views and attitudes towards SPRPCs.
Methods
Search strategy
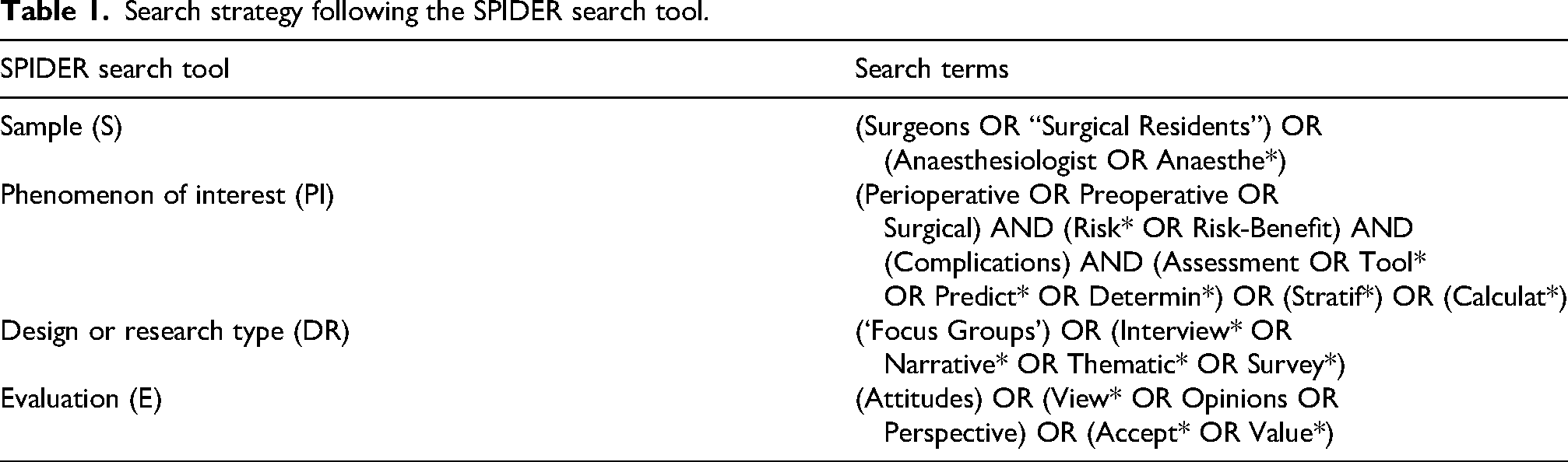
The protocol was registered on 06/11/2023 (PROSPERO-ID: CRD42023480234). Three electronic bibliographic databases were searched (EMBASE (SCOPUS), MEDLINE (Ovid) and CINAHL Library) using a SPIDER-based search strategy 16 (Table 1). Searches were limited to peer-reviewed publications between 01/2000 and 03/2025 in English and citations were also searched. An updated search was conducted on 25/3/25, 118 new articles were screened, but no further eligible studies were identified.
Search strategy following the SPIDER search tool.
Inclusion and exclusion criteria
Primary qualitative or mixed-methods studies exploring clinicians’ views or experiences of SPRPCs were included. Papers must have included verbatim quotes from clinicians but could address current or prospective SPRPC implementation. Studies of clinician and patient views were included where clinician-specific data could be identified and analysed.
Data extraction (selection and coding)
Search results were exported to RAYYAN and duplicates removed.17,18 Records were screened by title/abstract and then by full text. 19 One author (SJ) screened all search results by title/abstract, while a second author (AA) screened a random sample of 10% of the results (N = 51; agreement was 100%). Both authors screened all 31 articles retained for full text screening and chose the same 6 articles with 100% agreement. Data were extracted from all eligible articles by SJ, with AA performing a quality check on 50% with 100% agreement between authors.
Quality assessment
Papers selected for inclusion in the study were critically assessed for quality using the JBI checklist20,21 separately by two authors (SJ and AA). Both authors scored the studies the same (100% agreement) No studies were rejected based on quality (Supplementary Table 1).
Plan of analysis
Qualitative thematic synthesis was performed. Data analysis was performed in NVivo14, using the thematic synthesis protocol.22,23 Familiarisation with results and extraction of participant quotes was followed by inductive code generation (by SJ). Coding structures were evaluated by SJ and EF and codes combined to form refined themes. Studies were then reanalysed for further evidence of themes and themes refined discursively to reflect study aims.
Results
Literature searching results are given in Figure 1. Six papers were included; three from initial searches and three from bibliographies and citation searching in Google Scholar.24–29 Studies were published during 2015–2021.
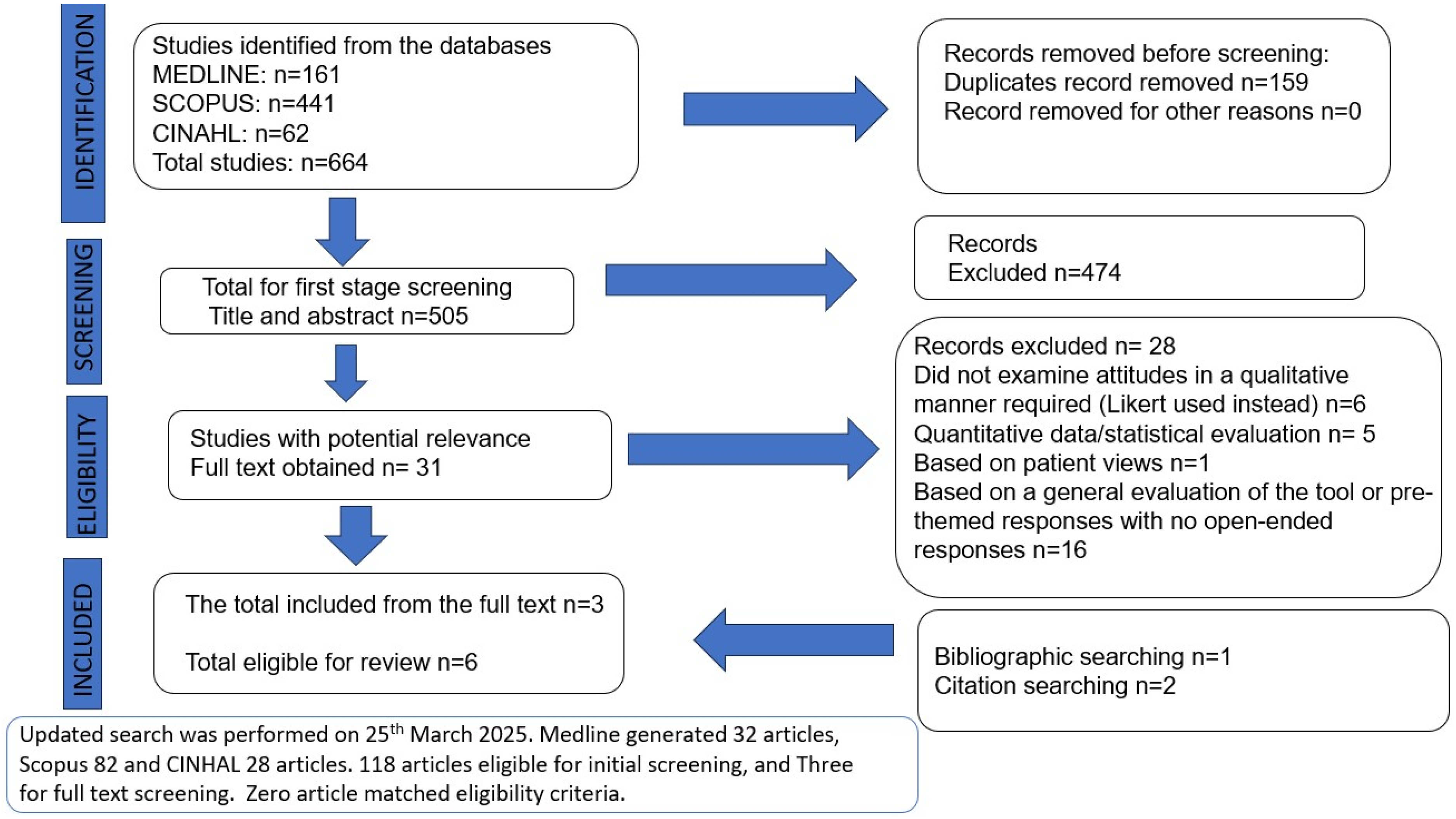
The PRISMA flowchart.
Study characteristics
The studies originated in United Kingdom, United States of America, Canada and Australia (Supplementary Table 2). Four studies were purely qualitative using either interviews (3) or focus groups (1); two combined questionnaire and interviews. Only two papers met all JBI critical appraisal criteria.
Data were reported from 72 clinicians (57 surgeons, 6 anaesthesiologists, 8 orthopaedic registrars and 1 internal-medicine registrar). Four studies reported gender split with 65.6% male, 34.4% female participants; clinician mean age was 47.3 years, with 0.5–30 years of specialist experience. In total, three studies focused on decision aids in orthopaedic surgery including aids used for total knee arthroplasty, total joint arthroplasty as well as tools to evaluate post-operative recovery through evaluation of pain using pain-catastrophising scale (PCS), two studies focused on the Surgical Perioperative Assessment System tool (SURPAS) and one on post-anaesthetic care unit (PACU) hypotension prediction24–29 (Supplementary Table 3).24–31
Themes
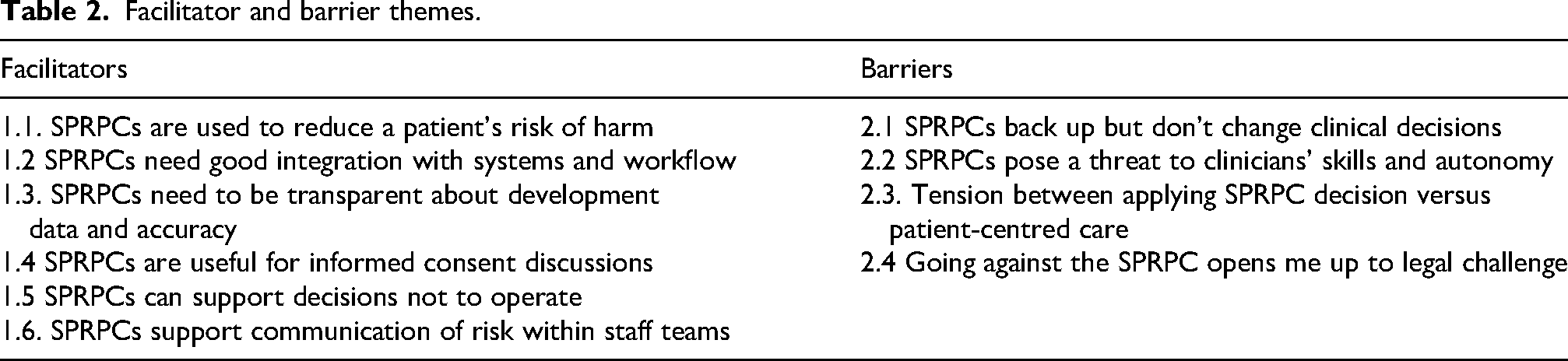
Table 2 summarises facilitator and barrier themes.
Facilitator and barrier themes.
Theme 1: factors which facilitate the use of RPCs
SPRPCs are used to reduce a patient's risk of harm
SPRPCs were viewed as aiding avoidance of potential harm, by identifying probable adverse events otherwise missed. This was viewed as an opportunity to question proposed plans and explore risk-mitigating alternatives. If you’re using this tool and it's making you ask certain questions, then that question itself hopefully might lead to others [and] the answer the patient gives, might lead to some other questions. (ID14)
24
If I knew that if I did this [used SURPAS] and that it showed my patient is much higher risk than I had previously thought, [and] if there's something I can do that's going to lower that, then that's a motivator. (Surgeon)
26
I found it helpful, primarily, with … more complicated patients presenting for more complicated surgery … with the less than healthy patients. (Provider #9)
27
SPRPCs need good integration with systems and workflow
SPRPCs were perceived to take up precious consultation time such that SPRPCs needed to be integrated into clinic workflow and record-keeping, ‘simple and quick’ (Provider #3)
27
or pre-completed by the patient. I just couldn’t use a tool that is going to take up more time. So the tool may only take 5 min but then you add 4, 5, 6 patients and that is half an hour extra … that you didn’t have. (022)
28
It is frantic getting patients through … But if there was something validated and it was done as a routine process, the patient came in with a form filled out with a score that would be really nice. (016)
28
…[I] very much like the documentation tool. You can generate the note of what the predicted risks are for that patient compared to the national database and simply copy that into your clinical note. (Provider #4)
27
SPRPCs need to be transparent about development data and accuracy
Doubts were raised about tool accuracy, the validity of the tool development research methods and access to transparent information about this, together with the transparency in information about these which was accessible to users. Would need to see the data and peer review.
25
The human body is not a scientific machine. Medicine is an art and science and the art isn’t always represented in the research. (028)
28
Unless you can clearly demonstrate a certain cut-off does better, so until there is almost black and white there will be some shades of grey. And even if there is evidence you will still get surgeons that will reject it. That is just my feeling. (021)
28
SPRPCs are useful for informed consent discussions
Participants viewed SPRPCs as helpful in the process of informed consent, supporting shared understanding and decision-making.
32
…one important thing about a decision-aid and the consent process is that they know what to expect and it is still the patient's decision to decide if they want to have surgery or not, but they can be appropriately informed and have the appropriate expectations to weigh up the risk and benefit. (019)
28
I’ve also ended with ‘does this change any of your thinking about this operation? Was this beneficial to you?’ Like I said, many patients say that it was beneficial to them because it makes them more comfortable proceeding with surgery. It reassures them that the choices that they pretty much already made are the correct ones. (Provider #4)
27
I think it increases the depth of understanding. (Provider #7)
27
Some of the results we've gotten have been surprising to me, in terms of the risks of the surgery for certain patients … I think it's been helpful for patients to see the numbers, at least from when I talked to them. It feels to me that they're more educated about their operation (Provider #10).
27
SPRPCs can support decisions not to operate
Surgeons reported difficulty with expressing their refusal to operate in patient discussions. It was hoped SPRPCs might support explanations for refusals clearly and empathetically, showing decisions were based on professional risk analysis, not personal feelings. I think the main benefit of an aid would be making the patient understand if I am saying no to the surgery, it's not because I don’t like them, it is because there is data written black on white that they are not going to do well … It will not just be my gut feeling. I can give them data and say, sorry, it is written here. It's not me, it's the computer. So it backs up what I am saying. (013)
28
These perceived benefits extended to communicating with patients’ families: I actually had one patient that it was helpful because I was able to demonstrate the reason why I felt an operation was not the best thing, because risks were significantly higher than the national average. The patient and the family could see that on the little human pictures, so they understood. (Provider#5)
27
SPRPCs support communication of risk within staff teams
SPRPCs were perceived as enhancing communication within multidisciplinary teams, adding value to management plans and advanced preparedness. However, this was contingent on tool confidence: I would communicate that this patient is at increased risk and ask them to have a heightened awareness of that possibility and communicate with me if they are starting to see some degree of hypotension.
25
It might be most helpful for less experienced post-anaesthesia care unit (PACU) nurses or nurses who did not have time to read the whole chart and think ‘oh yeah, when I see these patients, then I typically have to do this’ or ‘I am expecting a longer PACU stay’.
25
Of course, the resource allocation in the PACU can be challenging … The [risk] score can … help us be more proactive.
25
Theme 2: factors acting as barriers to adoption of SPRPCs
SPRPCs back up but don’t change clinical decisions
Some clinicians perceived that SPRPCs had little role in adjusting management plans, especially when alternative non-surgical options were limited: I have not made any changes in my operative decision-making based upon this tool. (Provider #6)
27
At the end of the day if there is a pathology that can be deleted by surgery and the patient accepts some improvement then that means that the surgery will happen. (025)
28
Instead, results generated by the SPRPCs were used to affirm their pre-determined decisions: I don’t think it would really influence my surgical decision-making, I think it would more affirm my decision. (029)
28
Well, if you make an alternative plan and say we are not going to do surgery we are going to lose weight, do some physiotherapy, take painkillers, you send them off and they come back and say they have done all of that. It means you don’t have another option to offer them and those patients often just want an option. (016)
28
SPRPCs pose a threat to clinicians’ skills and autonomy
Common among clinicians was concern that a decision-making tool challenged their personal clinical judgement and autonomy to guide consultations and come to a holistic decision for their patient. Clinicians considered their acquired skills were superior in enabling in-depth patient assessments, particularly where an SPRPC score deviated from their judgement: If I think they are ok and if they score badly I will relook at it and say why is that? Am I missing something obvious? But at the end of the day, if an aid says one thing and my sniff test says there is something not right, I’m still following my nose. (010)
28
I don’t use any formal tools. I use guess old-fashioned clinical acumen is what I would call it … I have been doing this for a while and you develop a way of assessing people. (028)
28
Not every tool is perfect and it may not capture every patient … the danger is we may end up refusing to do something because of this tool and therefore the patient may not receive the appropriate treatment based on a decision-aid, and nothing is 100% so you have to expect some patients would fall through the cracks. (019)
28
Whilst the risk score is at times helpful, it seems to overpredict minor hypotension in teens and younger women who have normal BP for these age groups, so no treatment would be necessary.
25
No, you can’t make anything compulsory like that … Medicine is not black and white, it is grey, you can never make anything compulsory because a surgeon will operate according to their experience. (024)
28
A lot of surgeons would say in their hands they will get better results, that is just an inherent bias associated with surgical procedures and surgeons themselves so it would be hard to agree on a level. (019)
28
Tension between applying SPRPC decision versus patient-centred care
There was a worry that rather than guiding or informing the clinician's decision, the result of the decision tool would be implemented regardless of the patient's individual circumstances, thus threatening patient-centred care: I don’t think there are things that can become compulsory in terms of a decision aid, as I mentioned, because it takes away patient-centred care. (025)
28
Going against the SPRPC opens me up to legal challenge
Clinicians were concerned about going against the result of an SPRPC, especially if it indicated high risk of a poor outcome and was documented in the patient's notes. Fearing a malpractice suit if the patient's outcome was poor led some to conclude that not using the SPRPC would protect them. You have to think of the medico-legal implications of a patient having a risk value documented in their notes. If they don’t have a good result and then lawyers look through and say you had this validated tool and you still went ahead, where would we lie medicolegally? (024)
28
Discussion
This review explored clinicians’ perspectives of SPRPCs in determining patients’ care, identifying factors which promote or hinder their use. Surgeons agreed that the use of SPRPCs could achieve lower surgical risks for patients, were useful for informed consent discussions, and particularly useful for supporting discussions around a surgeon's decision not to operate. The tools could be used to help explain to patients and family members why surgery would not be a safe option, and visualise risks in ways patients could understand.
SPRPC use was more likely when they were well integrated into patient record systems, clinic time and workflow or could be completed outside of consultation time. Tools were used more when their provenance and accuracy metrics were transparent and available. With experience, surgeons noticed patient groups for whom the tool might make poorer predictions and used their judgement when interpreting results. Clinicians trusted their own clinical acumen when making decisions in the best interests of the patient and did not want their autonomy diminished by compulsory application of tool results. Concern about legal challenge if surgeons operated after SPRPC results indicated poor outcomes, led some to avoid use.
The willingness of clinicians to use SPRPCs depended on what other options were available to offer patients, as they did not feel it was always possible to decline surgery based on risk, if no other treatment options were available. A blanket application of SPRPC outcome on patient decisions was also not considered ethical because it would reduce the patient-centeredness of the care provided.
Similar to our findings, previous studies have demonstrated SPRPC utilisation was greater among trainees, whilst more experienced clinicians rely on their judgement and value their autonomy. 9 Previous barriers identified have included tool integration with patient-specific medical records to match the clinical workflow needs, a lack of time to use the tool, and trust in the accuracy of the tool, all themes which emerged in this review.9,10 Clinicians may consider SPRPCs as over-simplistic, failing to capture the nuance of individual presentations in an all-inclusive manner.7,8 Their integration has been viewed as time-consuming and disruptive towards clinicians’ workflow with minimal output benefit.9,10,33 However, inappropriate subjective judgements, when tools are not used, may present safety implications, including an estimated 20% increase in cost of care adding pressure to the healthcare system. 10
Strength and limitations
Unlike previous qualitative studies on this topic, this review included a large sample of n = 72 participants. Nonetheless, generalisability is still limited; half the papers captured only orthopaedic specialist views. A wider range of specialities may have elicited different views.
The review reported on four high-income countries and cannot therefore inform the uptake of surgical SPRPCs in low- or middle-income countries where use may present different challenges but greater benefits to patient safety.
We chose to focus specifically on qualitative studies of clinicians’ views, rather studies which reported on closed-option responses to pre-specified statements or questions. This approach allowed us to capture the nuance and complexity of why clinicians behave as they do, rather than rely on quantitative data which necessarily simplifies the issues in order to standardise responses. Qualitative studies answer different and more in-depth research questions compared to structured surveys, helping to elucidate phenomena that determine how people behave in real and complex situations. Reliance on this one form of data also meant we could rigorously apply a thematic synthesis methodology.
However, we acknowledge that this specific focus on qualitative data means a loss of information about how common various experiences or barriers are, which would better inform intervention design. During the screening process, we noted several structured surveys of clinicians’ views on SPRPCs. Therefore, a review of these may be warranted to better understand the frequency and distribution of different experiences across specialties and types of respondents. Due to the small number of eligible studies found, an update to this review in a few years’ time would also be justified.
Implications for future RPC development
Our findings point to the following recommendations to improve uptake:
Directly involving clinicians in SPRPC development processes to best align them with clinicians’ workflow. Validating SPRPCs in real world settings. Providing an accessible evidence base for SPRPC provenance. Minimising completion time and/or designing for self-population from patient records. Designing SPRPCs for patient self-completion. Designing SPRPC outputs with clear infographics that are easily communicated to patients.
To support clinician autonomy and patient-centred care, it should also be made easy for clinicians to document the broader context rationales for overriding decisions produced by the tools. The ethical-legal considerations can be addressed through the production of widespread evidence-based guidelines and policies for use, which should be distributed to all tool users.
Conclusion
SPRPC use can aid surgical decision-making by applying evidence-based guidance to individual patients, and these tools have the potential to improve the quality of patients’ care as well as patient satisfaction. As healthcare systems continue to digitalise and streamline, and routine data is harnessed through Artificial Intelligence, we can expect SPRPCs of all types to burgeon. Addressing design features and clinical concerns in order to support rather than challenge clinical activities such as informed consent and patient assessment, can only better their use.
Supplemental Material
sj-pdf-1-cri-10.1177_25160435261421362 - Supplemental material for Clinicians’ views and attitudes towards perioperative or surgical risk prediction calculators: A systematic thematic synthesis
Supplemental material, sj-pdf-1-cri-10.1177_25160435261421362 for Clinicians’ views and attitudes towards perioperative or surgical risk prediction calculators: A systematic thematic synthesis by Sana Akal Jaan, Arooba Ali, Natalie Edelman and Elizabeth Ford in Journal of Patient Safety and Risk Management
Footnotes
Ethical considerations
This was a systematic review using publicly available data and therefore no ethical approvals were needed.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data are taken from referenced, published journal articles.
Supplemental material
Supplemental material for this article is available online.