
Abstract
Background
Workflow interruptions, especially in acute care, are a ubiquitous challenge. Concerning coordination and fast responses in complex work, interruptions foster inter-professional communication. Conversely, interruptions cause attention and task breaks, promoting potential errors or jeopardizing safe care. To mitigate the effects of workflow interruptions on care performance and patient safety, we need to understand the influence of provider tasks on the occurrence of workflow interruptions. Our aim was to investigate the likelihood of work interruptions related to provider activities.
Methods
Expert observations were conducted in an Academic Emergency Department with a standardized assessment of provider activities and workflow interruptions. A total of 160 observation sessions with nurses and physicians were analyzed. We ran multivariate logistic regression models to determine associations between provider tasks and workflow interruptions while controlling for confounders.
Results
On average, providers were interrupted 7.68 times per hour. Most interruptions stemmed from communication within the same profession (28.8%) and with other professionals (27.0%). During documentation and charting, interruptions were 2.5 times more likely than during patient communication. Likewise, diagnostic and therapeutic activities as well as coordination tasks were associated with higher odds of interruptions. Concerning individual interruptions sources, members of the same professional group were more likely to interrupt in a variety of activities. Yet, staff of other professions merely interrupted during charting and documentation.
Conclusions
Our findings reveal that providers engaged in charting and documentation face a higher likelihood of being interrupted. Interventions to mitigate interruptions in acute care should consider the dynamic interplay of tasks and the purpose of interruptions.
Introduction
In the quest to establish safe and effective patient care routines, workflow interruptions have been repeatedly in focus. An increasing literature base sheds light on the role of workflow interruptions for patient care and safety.1–4 Originally, interruptions were conceived as a hazard to safe care, associated with errors, failures, or slips in attention.5–7 Yet, it has been emphasized that interruptions have benefits and purpose, and thus a more nuanced understanding is necessary, based upon real-world observations.5,8,9
Particularly in acute care environments such as Emergency Departments (EDs), providers constantly act in disrupted workflows: interruptions are ubiquitous due to multiple events.10–13 Workflow interruptions can be defined as an intrusion of unforeseen events, causing the discontinuation of ongoing tasks, followed by a break as well as task switch behaviors (i.e. answering a call during a patient's examination).14,15 In ED settings, investigations showed a substantial load of interruption rates between 5 and 11 interruptions per hour.6,13,16–18
In acute care, interruptions are often an unavoidable part of work routines, triggered by inherent needs for coordination and collaboration across different professions, allocation of resources according to clinical demands, as well as urgent communication to master patient load. 19 To this end, interruptions may serve various purposes and may have inherent benefits for clinical care and patient safety.3,13,20,21 Yet, research has proposed that interruptions may have benefits such as allowing providers to gain help or information as well as directing attention to patients needing immediate actions. 22
Drawing upon a systems perspective, interruptions unfold in a dynamic and complex system of various organizational, work, process, and provider factors. 23 Hence, understanding interactions between system factors provides essential insights into how to improve safety and design modern clinical workplaces. 24 Given the current state of interruption research in acute care, the following shortcomings remain:
First, interruptions evolve through coinciding influences of external interruption sources and the provider's tasks. 19 However, previous research mostly ignored potential interrelationships of provider tasks and interruption events limiting inferences concerning potential adverse effects for performance or safety.9,25,26 Yet, the majority of interruptions in acute care work can be attributed to information exchange in intra- and inter-professional communication and coordination activities.17,18 Moreover, interruptions occur across a broad spectrum of different tasks. It has been proposed that interruptions may take place in opportune moments such that providers dynamically assess situations and inherent potential for risks and safety.19,27 A deeper understanding is necessary of how task conditions influence the likelihood of interruptions.
Second, acute care providers deal with a spectrum of workflow interruptions. Previous research in EDs demonstrated that different sources of interruptions stem from a variety of sources, for example, from patients, physicians, nurses, telephone calls, and malfunctioned equipment. 28 It is of interest, to elicit different sources of interruptions and their potentially differential association with provider tasks.13,19
Third, there is a paucity of naturalistic studies on provider activity interruptions in acute care environments. In-situ assessments with direct observations of the provider's workflow and interruptions allow a thorough understanding of how professionals juggle with competing demands to maintain fast and efficient care under time- and resource-constrained conditions.8,13
Objectives
In the light of these shortcomings, a study was set to answer the following research questions:
Are specific provider activities more likely to be affected by workflow interruptions? Are there relationships between specific provider activities and sources of interruptions?
Materials and methods
Design, observational setting, sample, and procedure
Data was collected as part of a larger quality improvement project in emergency care that is documented in detail somewhere else. 29 We used observational data collected during 160 standardized, participant observations of ED provider workflow and activities while patient care. Standardized observations followed an event-sampling method (see below).
The Ethics Committee of Medical Faculty, Munich University, approved the study (Nr. 327-15). All ED providers received written and verbal information prior to data collection. Participation was voluntary and consent was obtained.
The study setting was an ED of an academic center in Germany. This interdisciplinary, 24 h ED has about 84.000 yearly visits. The ED consists of three units: (1) internal medicine, (2) trauma patients, and (3) one short-term observation unit. Permanent staffing includes nurses and physicians from trauma surgery, internal medicine, neurology, as well as medical specialists on call.
Our sample included ED nurses and physicians in active ED patient care. We excluded professionals who had been working in the ED for fewer than 6 months and did not complete yet their professional training.
Our procedure of observations followed a previously established approach. 28 After consent, ED providers were shadowed by a trained observer of our study team. Observers followed this ED provider permanently for around 90 min during their routine work. Observers coded on a clipboard for each workflow interruption and activity, respectively (see below). We deployed a random selection scheme for assigning observations across ED units and the time of the day. In total, we have observed 13,767 min (229.45 h) of work tasks.
Measurements of ED provider's interruptions and activities
We coded provider activities as well as workflow interruptions. Additionally, we noted the times of the start of the respective activity, the end, as well as the time of the onset of the interruption. Post-hoc, time stamps allowed matching of activities and concurrent interruption events.
Activities were classified into five different task categories based upon a previously established and validated tool on ED provider tasks and interruptions.15,28 Supplemental Table 1 lists each task category and provides a short definition, respectively. Interruption events were categorized into five different sources (see Supplemental Table 1).
Additional information for each observation session included profession (physicians and nurses), ED unit (internal, trauma, and observation unit), and time of the day (morning and afternoon).
Statistical analyses
Observational data were transferred into an electronic database, checked for quality, and prepared for the following statistical analyses: we performed logistic regressions to evaluate the relationships between activities and the likelihood of the occurrence of an interruption within particular work tasks.30,31 For the interpretation of the effect, we used odds ratio (OR) with 95% confidence intervals (CIs). For interval-scaled predictors (e.g. task length in minutes), OR was defined as the variation in odds of the outcomes occurring regarding an increase of one unit in the predictor. For categorical predictors, one category was set as a reference. OR was reported for all other categories and defined as the odds of the outcomes occurrence for the respective category compared to the odds of the reference category. 31 To account for bias due to multiple testing, we conducted a Šidák correction resulting in a corrected significance level of p < .01. 31 We performed all analyses using R and RStudio.32,33
Results
A total of 160 observations were analyzed (99 ED physicians, 61 ED nurses; 56 observations in internal, 51 in trauma, 53 in observation unit). Observations lasted 86 min on average (SD = 7.69, median = 88.1, Min: 56.6, Max: 104.1).
ED providers were observed on 60.9 activities on average (SD = 19.7, median = 58) resulting in a total of 9746 activities. We documented interruptions during 1763 activities. Table 1 shows the total counts of observed tasks and interruptions as well as the adjusted durations and interruption rates.
Observed work tasks and workflow interruptions.
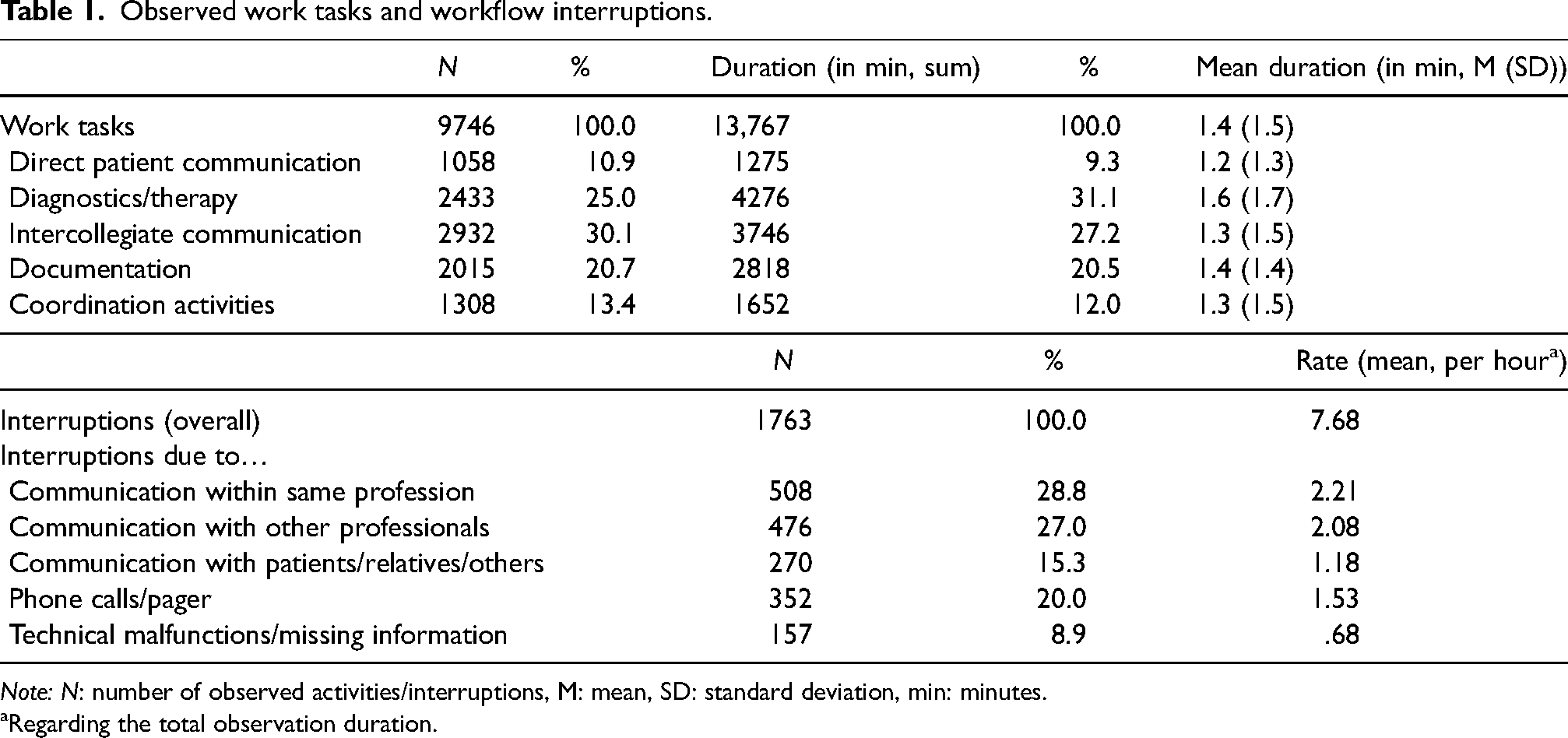
Note: N: number of observed activities/interruptions, M: mean, SD: standard deviation, min: minutes.
Regarding the total observation duration.
Preliminary analyses
We first tested for potential confounding effects. Analyses for contingencies indicated no systematic variation in the occurrence of task interruptions regarding the clinic or profession (Supplemental Table 2).
Nevertheless, inferential verification was examined by conducting a three-predictor logistic regression (with ED unit, profession, and task duration) and with the dichotomous outcome variable (0 = no interruption observed; 1 = interruption observed). Results indicated that task duration was significantly related to a higher likelihood of interruptions, that is, the longer an ED provider is engaged in a task, the higher the likelihood of being interrupted (cf. Supplemental Table 3). Specifically, for every additional minute an activity lasts, the likelihood of an interruption increased by 17% on average. This issue has been described previously as (task) length bias in interruption research. 34 Since there was no relationship with the profession or ED unit, these were not included in the main analyses.
Associations of ED provider activities and interruptions
With regard to our first research question, we investigated if the overall likelihood of workflow interruptions was significantly related to provider activities. Table 2 shows the results of this regression analysis.
ED providers’ tasks as predictors for the likelihood of interruptions.
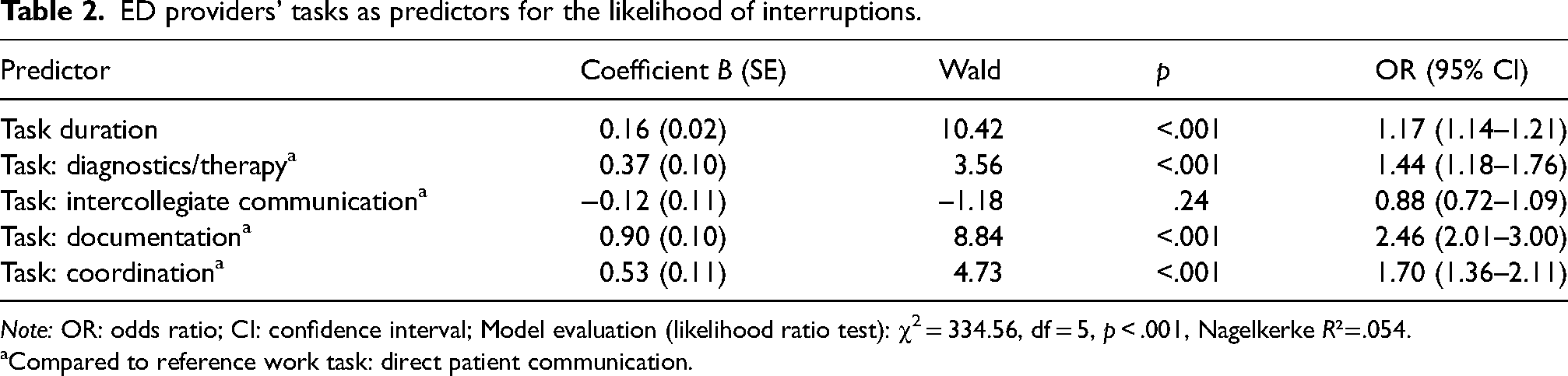
Note: OR: odds ratio; CI: confidence interval; Model evaluation (likelihood ratio test): χ2 = 334.56, df = 5, p < .001, Nagelkerke R²=.054.
Compared to reference work task: direct patient communication.
Consistent with our previous analyses, task duration was significantly related to the likelihood of an interruption event (OR 1.17, 95% CI: 1.14–1.21). Our analyses furthermore revealed that certain ED provider work tasks were more likely to increase the odds of interruptions: during working on documentation, professionals were more likely to be interrupted than during patient communication by the factor 2.46 (95% CI: 2.01–3.00). Likewise, work tasks of diagnostics and therapy (OR 1.44, 95% CI: 1.18–1.76), as well as coordination (OR 1.70, 95% CI: 1.36–2.11) were significantly more likely to be interrupted than patient communication. The likelihood of inter-collegiate communication was not significant.
For our second research question, we ran five logistic regression analyses. Results are shown in Supplemental Table 4.
Multivariate analyses revealed that occurrences of particular work interruptions were more likely within specific work tasks. Interruptions due to communication within the same profession were significantly more likely when professionals worked in diagnostics/therapy (OR 1.75, 95% CI: 1.12–2.56), documentation (OR 2.56, 95% CI: 1.76–3.72) or coordination tasks (OR 1.90, 95% CI: 1.26–2.85) compared to the reference task (i.e. direct patient communication). Moreover, interruptions as a consequence of communication with other professionals had a higher probability while working on documentation tasks in comparison with the reference task of direct patient communication (OR 2.88, 95% CI: 2.00–4.14).
Discussion
Interruptions to providers’ workflow are a common challenge in acute care settings. Particularly in emergency care, timely response and immediate adaptation to changing demands and patient conditions often means for providers to interrupt coworker's activities with potential risks for care performance, quality, and safety. 11 We investigated provider work tasks and interruption events to gain a deeper understanding how in acute work systems task and process factors are interrelated. 13 We deem our findings contributing to the existent knowledge evidence in the following:
First, we observed that the likelihood of workflow interruptions was different across different provider tasks. Specifically, we observed that during three provider activities—documentation, diagnostics & therapy, and coordination—observed odds for interruptions were significantly increased. Our analyses were controlled for task length bias such that the observed probabilities cannot be attributed to varying task durations. 34 ED professionals were about 2 to 3 times more likely to be interrupted during documentation and charting compared to engaging in direct patient communication: it has been previously suggested that ED physicians who are engaged in “solo non-communicative activities” may be perceived as more “interruptible.” 26 These results empirically confirm these assumptions. Yet, this likelihood may impair performance and safety, that is, while writing an order for medication for patient A, a nurse’s request to complete another order for patient B may result in flawed medication order(s). 11 Nonetheless, since the majority of the interruption research reports deleterious effects on provider performance, we assume that associated risks for the accuracy of order entries as well as the comprehensiveness of clinical information in the electronic health record (EHR) need to be carefully considered. 35
Secondly, we investigated respective relationships for five different sources of interruptions. Our granular approach allows a more nuanced understanding of how specific workflow interruptions may occur during particular clinical work tasks. Our analyses revealed significant associations for two sources of interruptions: both were related to inter-professional communication—either within the same professional group (i.e. nurse-nurse communication) or with another professional group (i.e. nurse-physician communication). For interruptions caused by communication within the same profession, we observed that such interruptions occurred with a 1.8–3.7 (OR 2.56) higher likelihood, particularly during documentation as well as coordination (1.3–2.9 times [OR 1.90]) and diagnostic/therapeutic activities (1.2–2.6 times [OR 1.75]). Interestingly, this was not consistently the case for interruptions caused by communications with other ED staff of other professions. Altogether, our observations suggest that professionals of the same profession tend to interrupt their colleagues unless they are engaged in patient or intercollegiate communication, in almost any activity (here subsumed as documentation, diagnostic/therapeutic, or coordination activities). Whereas providers of other professions tend to interrupt with a higher likelihood during documentation activities but not during other working tasks. To the best of our knowledge, this bias has not been empirically confirmed yet, although being suggested based on qualitative inquiries.19,36
Post-hoc, several explanations may be considered: first, ED staff of the same profession may have a deeper understanding of opportune moments when to interrupt their colleagues (i.e. such that interruptions also were observed during diagnostic/therapeutic as well as coordination activities take place). Potentially, colleagues with identical professional backgrounds may have a sense of when is the “right time” and colleagues are not deeply engrossed in their tasks. Eventually, providers may assume potential effects for cognitive load, capacity to resume with the interrupted task at hand, to recover performance as well as inherent risks for errors or procedural failures. 22 Moreover, a high number of interruptions in intra-professional interactions might indicate, that ED professionals conceive mutual interruptions as a tool to quickly adjust to changing work demands and act immediately upon emerging problems.13,22 Contrary, ED staff of other professions might assume charting and documentation activities as the most appropriate moment to disrupt, that is, the activity with the subjectively lowest risk for procedural failures or errors. Our results confirm that ED providers spent a significant amount of their work time (in our study about 21%, cf. Table 1) in clinical information systems with data-viewing and data-entering. 37 This may allow for multiple opportunities to interrupt. Moreover, charting and administration activities are often carried out in semi-public areas, at open workstations or desks without the protection of closed rooms or designated workspaces.26,38 Therefore, the layout and factors of EDs physical environment may undermine smooth workflow during charting or documentation activities. 39
Finally, our observations corroborate that providers spent a significant amount of time in documentation and charting activities as well as in communication with co-workers. Direct patient activities such as patient communication, diagnostic, and therapeutic activities added up to 40% of the overall working time. 18 Our findings resonate well with similar studies showing that ED professionals operate in interruptive work environments with a significant amount of interruptions.13,18,40
Limitations
Our data was obtained in a large academic ED in Germany. This may limit the external validity of our findings for other national healthcare systems or cultural contexts. 41 Observations allow for a realistic assessment of workflows, however, observer bias cannot be excluded. 8 We just recorded observable interruption events, for example, EHR-embedded messaging applications were not tracked. 42 We cannot infer about proximal or distal outcomes of the interrupted tasks. Although our study provides a comprehensive assessment across provider activities, our task and interruption classification schemes are rather broadly defined. Although this approach facilitates observations in dynamic ED settings, it yet dampens inferences concerning the variety of provider tasks and social interactions. Thus, future studies should investigate specific tasks or clinical scenarios with respective safety outcomes. 43 Our data stems from a convenience sampling approach, where selection bias may have occurred.
Implications for future patient safety research and practice in EDs
We demonstrated that the likelihood of interruptions is associated with specific providers’ activities. We showed that a large extent of interruptions is caused by inter-professional communication such that interruptions can be conceived as a common mode of mutual information exchange. Interruptions often arise from patients’ or providers’ needs with different urgency such as sometimes immediate reassessments or interventions are needed instantly in an evolving clinical situation. 13 Nonetheless, studies suggest that many interruptions originating in interpersonal communication are of low or medium priority and can be postponed.18,40 Future studies should, therefore, explore how providers perceive priority or acuity as well as when providers experience opportune interruption moments in busy ED care.19,20 Moreover, studies shall investigate how the timeliness of interruptions across various provider activities might result in patient safety events. 44 Future investigations should strive to apply fine-grained interruption and activity assessments that allow for more granular insights into the interdependencies of individual tasks and associated disruptions; as well as consideration of teamwork interactions. 20
Concerning ED practice, our findings may inform measures or interventions to mitigate interruptions in everyday clinical work. The results suggest that interruptions particularly during charting and documentation activities should be addressed. Moreover, the implementation of strategies and practices that minimize the number of interruptions, modify their intrusiveness, as well mitigating their impact on providers’ need to be undertaken. 11 Nonetheless, opportunities to mitigate workflow interruptions may come from various organizational, structural, and behavioral angles: that is, scheduling timed conversations for relatives, aligning patient flow with referring hospital units, ensuring appropriate staffing levels, and provision of closed spaces for key clinical administration tasks.45,46
Conclusion
To the best of our knowledge, this is the first investigation that comprehensively surveyed ED providers work tasks as well as concurrent interruption events. ED providers are often pulled in different directions due to multiple demands and events. Our findings show that the likelihood of interruptions is associated with the nature of their tasks. Particularly during charting and documentation activities, increased likelihoods were observed. Our insights may inform future interventions that seek to balance real-time information and collaboration demands as well as alleviate the hazardous impact of interruptions for provider efficiency and safety in emergency care.
Supplemental Material
sj-doc-1-cri-10.1177_25160435251346900 - Supplemental material for Associations of professional activities and workflow interruptions in acute care: An observational study in emergency department work
Supplemental material, sj-doc-1-cri-10.1177_25160435251346900 for Associations of professional activities and workflow interruptions in acute care: An observational study in emergency department work by Matthias Marsall, Anna Schneider, Markus Wehler and Matthias Weigl in Journal of Patient Safety and Risk Management
Supplemental Material
sj-doc-2-cri-10.1177_25160435251346900 - Supplemental material for Associations of professional activities and workflow interruptions in acute care: An observational study in emergency department work
Supplemental material, sj-doc-2-cri-10.1177_25160435251346900 for Associations of professional activities and workflow interruptions in acute care: An observational study in emergency department work by Matthias Marsall, Anna Schneider, Markus Wehler and Matthias Weigl in Journal of Patient Safety and Risk Management
Supplemental Material
sj-doc-3-cri-10.1177_25160435251346900 - Supplemental material for Associations of professional activities and workflow interruptions in acute care: An observational study in emergency department work
Supplemental material, sj-doc-3-cri-10.1177_25160435251346900 for Associations of professional activities and workflow interruptions in acute care: An observational study in emergency department work by Matthias Marsall, Anna Schneider, Markus Wehler and Matthias Weigl in Journal of Patient Safety and Risk Management
Supplemental Material
sj-doc-4-cri-10.1177_25160435251346900 - Supplemental material for Associations of professional activities and workflow interruptions in acute care: An observational study in emergency department work
Supplemental material, sj-doc-4-cri-10.1177_25160435251346900 for Associations of professional activities and workflow interruptions in acute care: An observational study in emergency department work by Matthias Marsall, Anna Schneider, Markus Wehler and Matthias Weigl in Journal of Patient Safety and Risk Management
Footnotes
Acknowledgements
The authors thank Theresa Steeb, Tobias Filmer, Joana Beck, and Tobias Augenstein for their support in data collection. The study was conducted at the Institute and Clinic for Occupational, Social and Environmental Medicine, University Hospital, LMU Munich, Munich, Germany.
Authors’ contributions
Marsall, Schneider, Wehler, and Weigl: conceptualization; Schneider, Wehler, and Weigl: methodology; Marsall and Weigl: validation; Marsall and Weigl: formal analysis; Schneider, Wehler, and Weigl: investigation; Wehler and Weigl: resources; Marsall, Schneider, and Weigl: data curation; Marsall, Schneider, Wehler, and Weigl: writing–original draft; Marsall, Schneider, Wehler, and Weigl: writing–review and editing; Wehler and Weigl: supervision; Schneider, Wehler, and Weigl: project administration; Weigl: funding acquisition.
Consent to participate
Study participants received written and verbal information prior to data collection. Participation was voluntary and informed consent for study participation was obtained from all participants.
Consent for publication
Not applicable.
Data availability
Anonymized and de-identified data will be made available to other investigators upon request. Please contact the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Ethics Committee of Medical Faculty, Munich University, approved the study (Nr. 327-15). The study was performed according to the Declaration of Helsinki.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded by the Munich Centre for Health Sciences (MC-Health).
Guarantor
Matthias Weigl as guarantor accepts full responsibility for the work and the conduct of the study, had full access to the data, and controlled the decision to publish.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.