
Abstract
Background
Incident disclosure has proved its cultural sensitivity. To meet patient needs, this study aims to investigate Japanese preferences regarding incident disclosure.
Methods
An online panel questionnaire survey was conducted in Japan, and 840 valid responses were collected. A total of 191 (23%) respondents or their family members had incident experience. The respondents were asked to indicate their preferences regarding disclosure practice, specifically for incidents entailing moderate and severe harm. The chi-squared test was applied to examine preference differences.
Results
Mostly similar preferences were identified among Japanese respondents, regardless of their incident experience, age, and sex. For instance, they wished to be disclosed through face-to-face communication (92% in moderate and 92% in severe harm incidents), immediately after detection (63%; 65%), at the bedside, or in a consultation room (50%; 46%). The incident was likely to be disclosed by the healthcare provider most responsible/directly involved in the patient's care at the time of the incident (48%; 45%), accompanied by the team/department leader (50%; 56%) and patient safety manager (50%; 59%). If the incident entailed severe harm, top management members were also expected to be involved (45%); all details about the incident were expected to be informed (57%).
Conclusions
The findings reveal that Japanese patient preferences regarding incident disclosure are partly shared with Western countries and partly with other Asian countries. The unique Japanese preference for disclosure places is also identified. Recommendations for incident disclosure are then suggested and we believe this could be the first step toward supporting disclosure in Japanese healthcare organizations.
Introduction
Substantial efforts have been made to improve patient safety through incident reporting and learning as these provide important information for quality and safety improvements. 1 In addition, once an incident has occurred, disclosure becomes important. Disclosure refers to communication between a healthcare provider and a patient; the patient's family members; or a proxy that acknowledges the occurrence of an incident, describes the incident, and delineates the link between the incident and its outcomes in a manner that is meaningful to the patient. 2 The key elements of disclosure are an explanation of the event, an appropriate acknowledgment of responsibility, sincere regret and apology, appreciation of how the event has affected the patient and family, commitment to preventing a recurrence, and evidence that learning has occurred. 3 Thus, disclosure stems not only from the ethical imperative to tell the truth but also from the need to develop safer healthcare delivery systems. 4 In addition, it is a promising means by which the number of lawsuits against a healthcare institution can be reduced, patient satisfaction can be enhanced, and healthcare providers involved in the incidents can get relief.5,6 The disclosure of harmful incidents is required in many Western countries, for example, the UK, Australia, New Zealand, and Germany.7–9 Disclosure has become a widely accepted practice standard across disciplines, and many countries have established national policies to encourage and guide the disclosure.10–14 Excluding near misses and no-harm incidents, the initial question of “whether to disclose” is no longer relevant.
However, the implementation of disclosures in practice has been challenging. Western countries with well-developed disclosure policies report that, despite theoretical support for disclosure, as few as one-third of patients are informed about harmful incidents during their care.10,15 In addition, a policy–practice gap exists as disclosures are made not in alignment with current policy guidance.7,16,17 Numerous barriers were reported related to this, including incomplete implementation of the disclosure policy on the front line; 18 potentially inadequate legal protection for healthcare professionals or organizations; healthcare professionals lacking education, training, and support from the healthcare organization; and fear of litigation. 19 It was also suggested that the current policy guidance may not sufficiently address the issues arising in disclosure practice. 7 Besides, healthcare professionals experience various other apprehensions regarding the disclosure process, such as when and how to disclose, who should disclose, and whether other team members should be present. 20 Accordingly, research has increasingly shed light on these issues,21–26 and then another gap between patient expectations and the actual practice of incident disclosure was revealed.25,27 To bridge this “disclosure gap” and resolve the “disclosure dilemma,” 28 it is important to understand patient needs and experiences.
The importance of cultural sensitivity has been proved in incident disclosure. 29 Therefore, the findings obtained from the aforementioned studies in Western countries could not be generalizable to non-Western cultures.30–32 Additionally, patient perspectives of incident disclosure are also varied among non-Western countries. 6 In most Asian countries, there is no national policy to encourage and guide the disclosure to patients. However, efforts to disclose after incidents are continuously being made. For instance, the Japanese government enacted the “Medical Accident Investigation System” in 2015 for incidents that caused patient deaths. 33 Disclosure to patient families was designed as one process in this system, but no more detailed information was provided to guide the disclosure. The limited research findings have revealed that similar to patients in Western countries, Asian patients also desire incident disclosure, such as in Japan, 34 China, 6 and Korea. 35 However, like in other Western countries,36,37 incident disclosure is not commonly practiced. In addition, there is a lack of incident disclosure education and training for medical students. Therefore, as a first step, guidance is required about the basic, albeit important, issues pertaining to incident disclosure such as when and where to disclose, how and who should disclose. For this purpose, patient needs regarding incident disclosure should be understood. Related studies have been conducted in China 29 and Korea 35 whereas not yet well investigated in Japan. The Chinese 29 and Korean 35 studies revealed that although some aspects are shared, significant differences exist not only between Western countries but also between the two Asian countries, for example, regarding whether to disclose near misses, the person to make the incident disclosure, and the representatives of hospital side attending disclosure meetings.
Therefore, focusing on Japan in the present study, we aim to investigate Japanese patients’ preferences regarding incident disclosure. Specifically, outcome severity level and prior incident experience are considered as patient needs in relation to incident disclosure may vary.7,38 The cultural sensitivity is then discussed by comparing the Japanese patients’ preferences to other countries. In addition, suggestions are made to support healthcare organizations and professionals in disclosure practice.
Methods
Instrument used in the survey
The present study is a cross-sectional study that applied the questionnaire survey approach. The questionnaire used in this survey was adapted from the previous study. It was developed by reviewing the existing literature, guidelines, and discussions with healthcare professionals and patient safety managers. 29 No mismatch with situations in the Japanese context was ensured by minor revisions, and the questionnaire was pre-tested by several Japanese individuals. The questionnaire included two sections in addition to a demographic section. This article reports the findings derived from responses to the second section. There were 15 items in this section to assess respondents’ preferences regarding how incidents should be disclosed to them if they were the affected patients. The first item (i.e. “How severe should an incident be to inform you of its occurrence?”) assessed the severity at which incident disclosure was desired. Severities defined in the questionnaire were near miss as “an incident detected before it reaches patients”; mild harm, referring to “no intervention or only minimal intervention is required”; moderate harm requiring “additional treatment, for example, possible surgical intervention and a longer duration of hospitalization”; and severe harm, referring to “major permanent or long-term harm.”39,40 The subsequent items focused on moderate and severe harm incidents because healthcare organizations experience extreme difficulty in disclosing these incidents. Respondent preferences regarding the following seven aspects were assessed: disclosure method, the extent of information provided, timing, place, patient and hospital representatives, and the person to disclose the incident. Several response options were provided for each question. The respondents were required to indicate their preferred option for each item, and multiple choices were acceptable for the items regarding patient and hospital representatives. The question items did not differ between public and private healthcare services, because there is no difference in access and national health insurance coverage in the Japanese healthcare system.
Survey sample
This study was approved by the Ethics Committee of the Institute of Science Tokyo (No. 2018139). An online Japanese questionnaire survey was conducted between December 2020 and January 2021. To recruit a large and representative sample from the general population in Japan, we employed a survey company (Cross Marketing Inc., Tokyo, Japan), which has a large panel including millions of registered members. Data were collected from Japanese nationals who were non-healthcare professionals, aged 20 years or older, and living in Japan. Informed consent was obtained using a letter of introduction, which the respondents read before answering the questionnaire. This letter described the purpose of the survey and assured them of the voluntary nature of participation, anonymity, and the confidentiality of the responses. A total of 840 valid responses from 46 out of 47 Japanese prefectures were collected; 203 (24%) respondents or their family members had been hospitalized during the past 3 years, and 459 (55%) respondents had consulted a healthcare provider as an outpatient during the past 6 months. In addition, 191 (23%) respondents had experienced incidents themselves or in their family members. An overview of the study sample is provided in Table 1.
Profile of the Japanese survey sample.
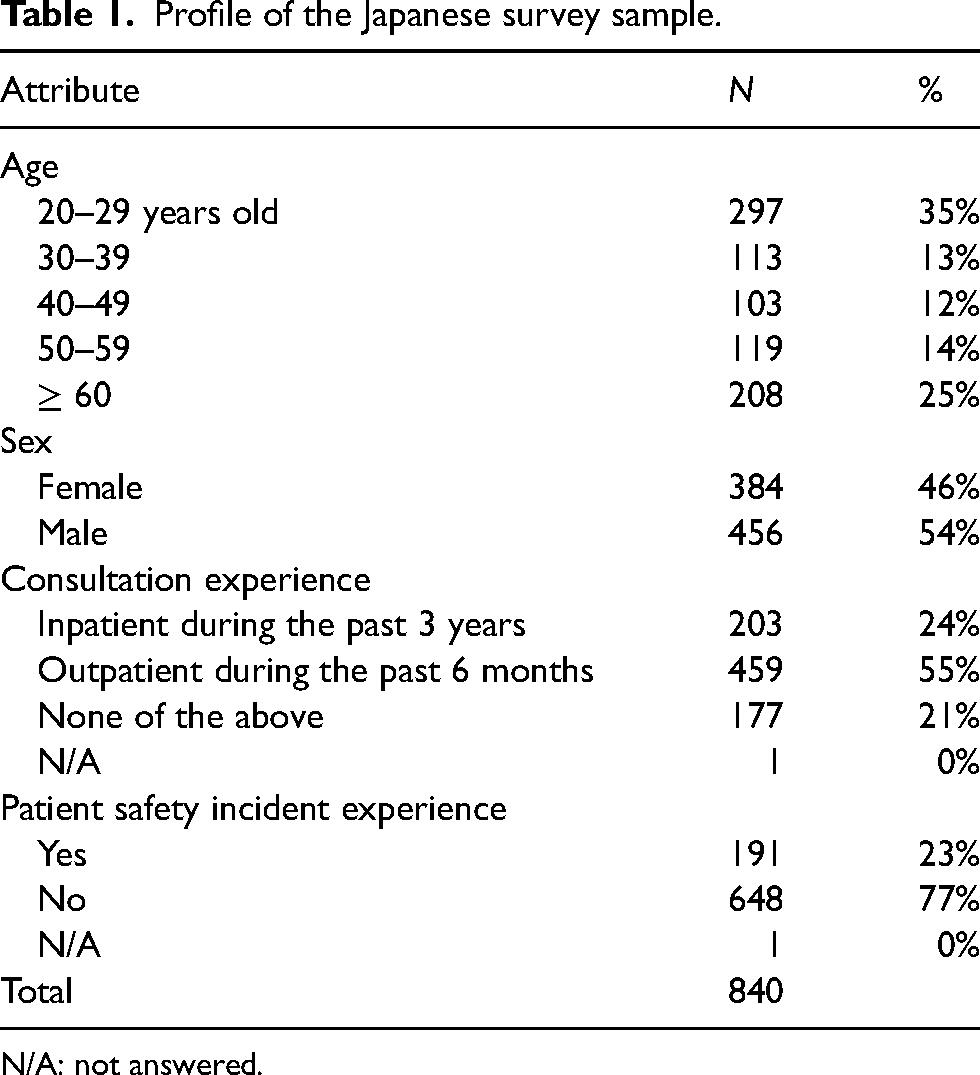
N/A: not answered.
Statistical analysis
Crosstabulation of simple frequencies and the chi-squared test were used to compare Japanese respondents’ preferences regarding the two types of incidents disclosure (i.e. moderate vs. severe). This test was also used to examine their preference differences as a function of respondents’ prior incident experience themselves or in their family members (“yes”: n = 191 vs. “no”: n = 648), age groups (“younger (20–39 years old)”: n = 410 vs. “middle-aged (40–59)”: n = 222 vs. “older (60 or over)”: n = 208), and sex (“female”: n = 384 vs. “male”: n = 456). Due to the small number of responses, the option “others” was excluded from all chi-squared tests. Regarding validation of the instrument, it was verified by the small percentages of “others” responses, as well as the cultural differences such as the underlying different preferences between Japanese and Chinese for the disclosure place and the person to disclose the incident (refer to Supplemental Material 1 for all the detailed comparison results between the Japanese and the Chinese responses collected in the previous study 29 ). All statistical analyses were conducted using the IBM SPSS Statistics 25 software (Chicago, IL, USA).
Results
Severity at which incident disclosure is desired
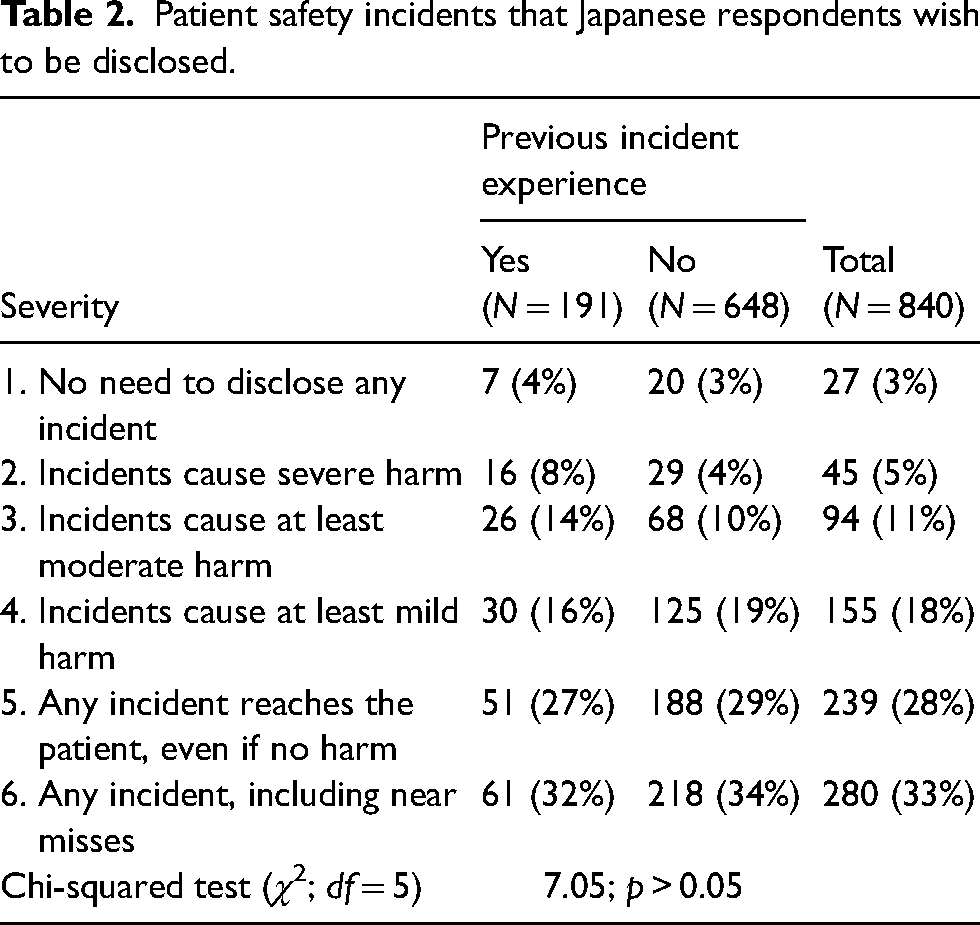
About 30% of the Japanese respondents desired any incident to be disclosed regardless of the harm it entailed. Further, one-third of the respondents expected even near misses to be disclosed. Table 2 presents the percentages of Japanese respondents who wished to be informed about incidents that differ in harm severity as a function of their incident experience (i.e. yes vs. no). The overall trends of the two groups were similar (χ2[5] = 7.05, p > 0.05). In addition, although one significant difference was identified, the underlying trends of the three age groups (χ2[10] = 30.21, p < 0.01) and the two sex groups (χ2[5] = 7.38, p > 0.05) were also shared (refer to Supplemental Material 2).
Patient safety incidents that Japanese respondents wish to be disclosed.
Preferences regarding disclosure of incidents entailed moderate and severe harm
The crosstabulation of simple frequencies for Japanese respondents’ preferences is shown in Table 3. The chi-squared test was conducted to reveal their preferences as a function of harm severity (i.e. moderate vs. severe) and a function of prior incident experience (i.e. yes vs. no). The seven aspects are described one by one. The chi-squared test was also conducted to reveal their preferences as a function of age and a function of sex. The underlying trends of the three age groups and the two sex groups were shared for all seven aspects; the only exception was about information provision in a moderate harm incident between female and male groups (refer to Supplemental Material 2). Therefore, only this exception is described in detail.
Japanese respondents' preferences regarding incident disclosure.
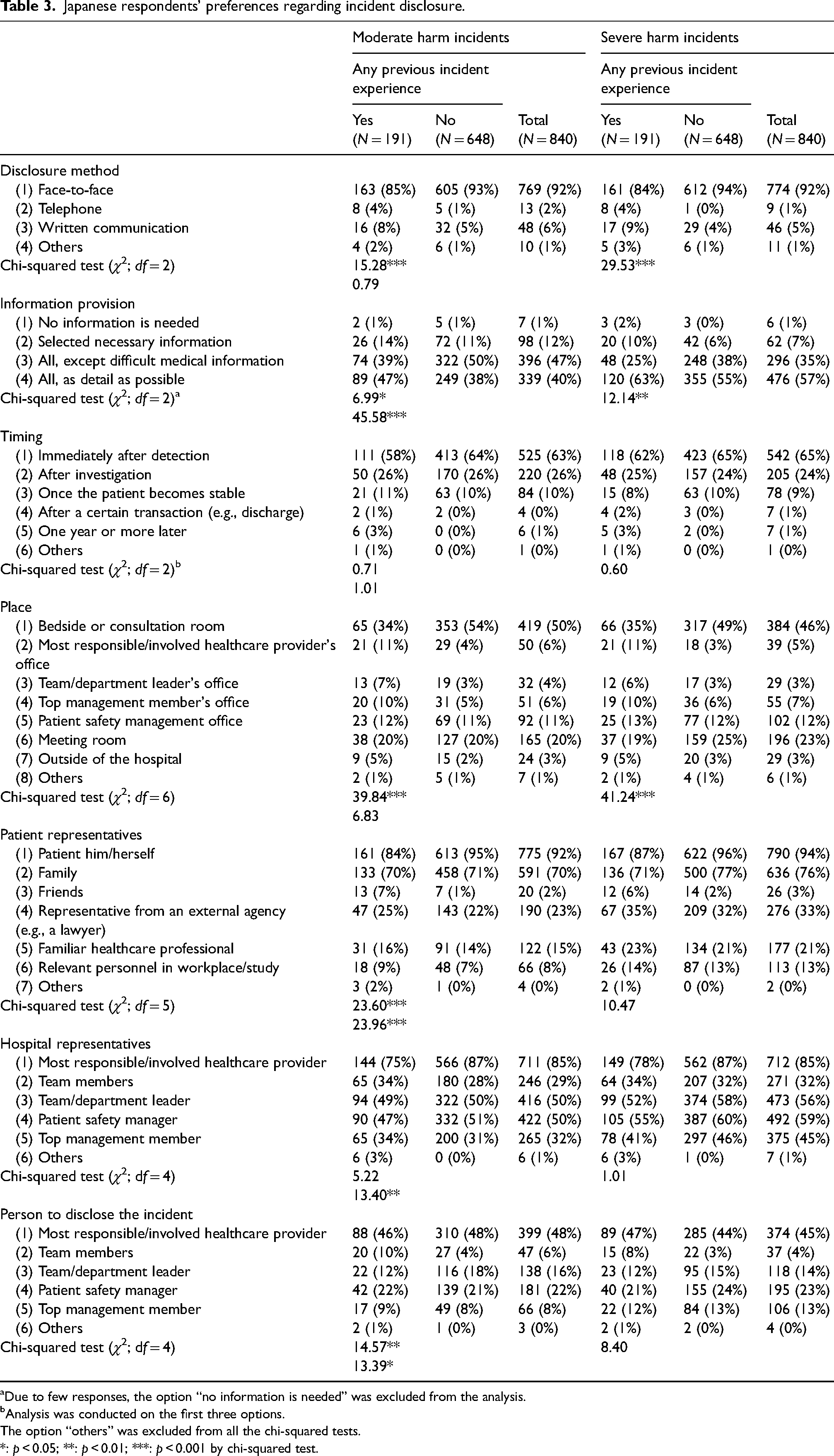
Due to few responses, the option “no information is needed” was excluded from the analysis.
Analysis was conducted on the first three options.
The option “others” was excluded from all the chi-squared tests.
*: p < 0.05; **: p < 0.01; ***: p < 0.001 by chi-squared test.
Disclosure method
No significant difference was revealed in Japanese respondents’ preferred disclosure method as a function of harm severity (χ2[2] = 0.79, p > 0.05), and the most preferred method was face-to-face communication. Significant differences as a function of prior incident experience were identified in both moderate and severe harm events. However, the trends underlying their preferences were similar between the two groups.
Information provision
Regarding the extent of information with which the Japanese respondents wished to be provided, there was a significant difference between the two harm-severity levels (χ2[2] = 45.58, p < 0.001). The Japanese respondents were more likely to want detailed information about an incident that caused severe harm (57%) than one that caused moderate harm (40%). For both situations, it seems that all details about the incident were mostly preferred by respondents who had experienced incidents, which was significantly higher than among those with no incident experience. A significant difference was also observed between sex groups for moderate harm incidents (χ2[2] = 8.40, p < 0.05). Comparing to male respondents (36%), female respondents (46%) were more likely to want all details.
Timing
According to the response numbers shown in Table 3, the chi-squared test was conducted for the three options for disclosure timing: “immediately after detection,” “after investigation,” and “once the patient becomes stable.” There was no significant difference in Japanese respondents’ preferred timing of disclosure between the two harm severity levels (χ2(2) = 1.01, p > 0.05). The most preferred timing was immediately after incident detection, followed by after an investigation. Similarly, no significant difference was identified between groups with and without incident experience.
Place
There was no significant difference in Japanese respondents’ preferred place of disclosure as a function of harm severity (χ2[6] = 6.83, p > 0.05). The most preferred place to receive disclosure was the bedside or a consultation room, followed by a meeting room. Significant differences were identified between respondents who had and had not experienced incidents. However, the trends underlying their preferences were similar between the two groups.
Patient representatives
Regarding the individual to whom the incident should be disclosed, there was a significant difference between the two harm severity levels (χ2[5] = 23.96, p < 0.001). In a severe harm event, Japanese respondents were more likely to ask a representative from an external agency (e.g. a lawyer) to be present for the disclosure. However, the trends underlying their preferences were similar; over 90% of the respondents preferred to be directly informed about any incident, and ∼ 70% wanted their family to be present during the disclosure. Similarly, although, in the moderate harm event, a significant difference was observed as a function of respondents’ prior incident experience, the trends underlying their preferences were similar.
Hospital representatives
Regarding Japanese preferences pertaining to hospital representatives, there was a significant difference between the two levels of harm severity (χ2[4] = 13.40, p < 0.01). More Japanese respondents expected representatives from the top management of the hospital (e.g. the president) to be present for severe events; the percentage increased from 32% to 45%. However, the trends were shared that 85% of the Japanese respondents wanted the healthcare provider who was most responsible/directly involved in the patient's care at the time of the incident to be present. Over half of them expected the presence of the leader of the team/department and a patient safety manager. In addition, no significant difference was observed regarding hospital representatives’ preference as a function of incident experience for either moderate or severe harm events.
Person to disclose the incident
Regarding the person who should disclose the incident preferred by Japanese respondents, there was a significant difference between the two harm severity levels (χ2[4] = 13.39, p < 0.05). However, the two situations shared the trend that the highest preferred person was the healthcare provider most responsible/directly involved in the patient's care at the time of the incident (48% in moderate and 45% in severe harm events), followed by the patient safety manager (22%; 23%) and then the leader of the team/department (16%; 14%). Similarly, although there was a significant difference between the groups with and without incident experience for moderate harm events, the aforementioned trends were shared by the two groups.
Discussion
International comparisons of patient preferences regarding incident disclosure
This study identified mostly similar preferences regarding the disclosure of incidents among Japanese individuals, regardless of their incident experience, age, and sex. Their preferences are partly shared with Western countries and partly with other Asian countries. All the aspects are discussed as follows.
Regarding whether near misses should be disclosed, this study reveals that Japanese patients varied in their attitudes toward near miss disclosure, which was similar to China 29 and some Western countries such as the UK 18 and the USA. 41 In contrast, it differs from the trend observed in Korea of most individuals demanding open disclosures of near misses. 35
Regarding preferences for the disclosure of incidents that entail moderate or severe harm, Japanese patients were likely to be informed about the incident through face-to-face communication and in a timely manner after incident detection. These findings are comparable to those reported for China, 29 Korea, 35 Australia, 25 the USA,23,42 and New Zealand. 24 Disclosure is suggested to include an explanation of the key elements of the incident, an evaluation of the impact of the event on the patient and family, a dedication to preventing a repeat occurrence, and demonstrating that lessons have already been absorbed.3,43 Therefore, disclosure may not be only once. The immediate information could be provided in the first timely disclosure; after investigation, disclosure of other information is made further for several times if necessary. Regarding the highly technical medical information, healthcare providers are suggested to inquire about patient preference and prepare to honestly disclose all required information. 29
Japanese patients preferred disclosure at the bedside or in a consultation room. This expectation is different from Chinese 29 and those in other countries like the USA,21,23 who wished to be informed in a meeting room. Another study in Switzerland also reported that patients did not find agreement on the desired location and the privacy level of disclosure. 26 However, the result obtained in this study does not indicate that Japanese patients prefer informal disclosure, although disclosure is commonly practiced informally at the bedside.16,17 Thus, it is important to prepare before disclosure, including providing a non-interrupted environment.
Expecting the most responsible/directly involved healthcare provider to disclose, the preference of Japanese patients corresponds to those observed in Western countries such as the USA 21 and New Zealand. 24 However, this finding is different from the trend observed in China 29 and Korea, 35 which found that patients preferred to be informed by those who occupy a higher position within the organizational hierarchy. Although Japanese patients in this study did not prefer high-position personnel to disclose the incident, they did show their preference for top management personnel attending the disclosure meeting, particularly in a severe harm event. This may be because, in Asian culture, patient perceptions of hospital sincerity improve when higher-position personnel are involved in disclosure. In addition, patients expect not only disclosure but also reconciliation; therefore, those who occupy high positions and are empowered to make decisions about pertinent issues (e.g. compensation and future treatment) are expected to be involved in this process. 29 It means that, rather than the most responsible/directly involved healthcare professional disclosing alone, a team disclosure is suggested.20,44
Implications for incident disclosure practice
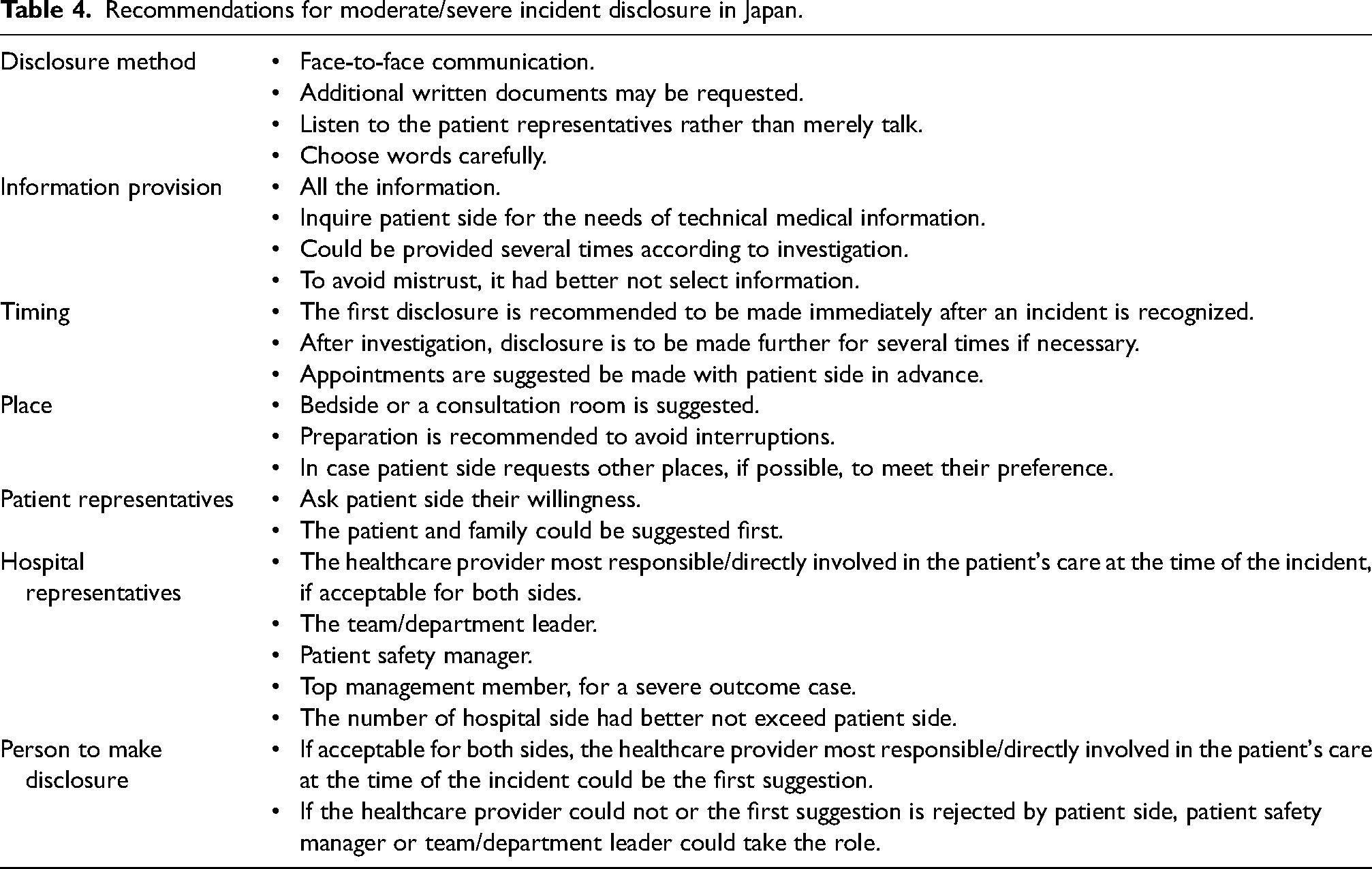
According to the findings of the present study and referring to the existing guidelines, for example, Duty of Candour in the UK, 12 Australia Open Disclosure Framework, 11 Guidance on Open Disclosure Policies in New Zealand, 13 and Canadian Disclosure Guidelines, 14 the recommendations for incident disclosure in Japan are proposed in Table 4. There is no one-size-fits-all approach to competent disclosure.23,24,26 Therefore, the suggestions we would like to make from the patient perspective are flexible, and can be tailored to individual patients’ needs and could help healthcare providers on how to enact disclosure. 9 We suggest face-to-face communication, and written forms are provided after the disclosure if requested. 15 To build trust relationships, assumptions are not made about the kinds of information that patients/families consider to be necessary; instead, all details could be honestly disclosed.24,29,45 Patients and family members find detailed explanations more helpful than confusing. 42 Certainly, highly technical medical terms had best be avoided. 15 In addition, the “being heard” element is proposed as it is insufficient to only listen to the patient's answers to questions posed by providers.24,45 Words are to be selected carefully to promote reconciliation.10,24 The key point for the disclosure place is that a meeting room, as suggested by most countries,21,23 may not be appropriate for Japanese patients. Thus, a familiar and comfortable place for patients could be better for disclosure and reconciliation. Preparations before disclosure are suggested to ensure no interruptions and privacy. In addition, a team disclosure is suggested20,44 and the representatives of both hospital and patient sides are carefully discussed up to needs. Regarding the disclosure aspects that have not been investigated in the present study, generalizing from the aforementioned guidelines in Western countries to Japan should be careful. For instance, adding the word “sorry” as suggested in these guidelines may have a different effect in Japan which has its own apology culture. 46
Recommendations for moderate/severe incident disclosure in Japan.
Limitations
The present study has four main limitations. First, although the responses were collected from 46 out of 47 Japanese prefectures, the response rate could not be known because of the online survey methodology. In addition, the survey sample was small and the percentage of young respondents was higher than that of the Japanese population distribution. However, the results of this study revealed that trends underlying Japanese preferences were mostly similar regardless of their age. Therefore, the findings could be representative of the general population to some extent. A larger and more representative sample is expected in future studies. Second, the respondents had not necessarily suffered from moderate or severe harm incidents in real life. Thus, their responses could be different if they are affected by a real event. However, the findings in this study revealed that trends underlying Japanese preferences were mostly similar regardless of their incident experience. Thus, we believe the results obtained from this study could be reliable. Third, the proposed recommendations pertain solely to incidents that entail moderate and severe harm. Therefore, future studies should examine how to disclose incidents that entail mild or no harm, that is, lower-level disclosure. 17 Fourth, the situation of children or older adults with a responsible family member was not addressed and this study was designed only from the patient perspective. Various patient situations and other stakeholders’ perspectives involved in incident disclosure should be investigated in future studies.
Conclusions
This study investigated preferences regarding the disclosure of incidents among Japanese individuals. The findings revealed mostly similar preferences among Japanese respondents regarding the disclosure of incidents that entail moderate and severe harm. In addition, the trends underlying their preferences were mostly alike, regardless of whether they had incident experience or not, their age and sex.
Japanese patient preferences are shared with Western countries for some aspects and shared with other Asian countries for other aspects. In addition, the unique Japanese preference for disclosure places is also identified. Therefore, to ensure that incidents are disclosed in accordance with patient preferences, the present findings are potentially helpful to support Japanese healthcare organizations and professionals in disclosure practice.
Supplemental Material
sj-docx-1-cri-10.1177_25160435241305232 - Supplemental material for Japanese patients’ preferences regarding disclosure of patient safety incidents: A survey study
Supplemental material, sj-docx-1-cri-10.1177_25160435241305232 for Japanese patients’ preferences regarding disclosure of patient safety incidents: A survey study by Xiuzhu Gu and Mingming Deng in Journal of Patient Safety and Risk Management
Footnotes
Authors’ contributions
Both authors contributed to the conception and design of this study and data collection. Gu X made analysis and interpretation of the data and drafted the first version of the manuscript. Deng M revised it critically for important intellectual content. Both authors have read and approved the final version of the manuscript.
Acknowledgements
We are grateful to the respondents who participated in our survey and the hospital management personnel for insightful discussions.
Ethical approval
This study was performed in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Institute of Science Tokyo (no. 2018139). All methods used in this study were performed in accordance with the relevant guidelines and regulations.
Consent to participate
Informed consent was obtained using a letter of introduction, which the respondents read before answering the questionnaire. This letter described the purpose of the survey and assured them of the voluntary nature of their participation, their anonymity, and the confidentiality of their responses.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was in part supported by the Japan Society for the Promotion of Science [grant number 19K15236] funded to the first author. This funding body had no role in the design of the study, or collection, analysis, and interpretation of data, or in writing the manuscript.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.