
Abstract
Background
The Coroners and Justice Act allows coroners in England or Wales to issue reports after inquest, if they believe that action should be taken to prevent a future death. Coroners are under a statutory duty to issue a Prevention of Future Death (PFD) report to persons or organisations that they believe have the power to act. Cumulatively, these reports may contain useful intelligence for patient safety. The aim of this study was to examine the feasibility of extracting data from these reports and to evaluate if learning was possible from any common themes.
Methods
Reports were extracted from 2016 to 2019 for deaths in hospitals, care homes and the community in England and Wales. These were subjected to descriptive statistics and thematic analysis of coroner’s concerns. Application of data mining techniques was not possible due to data quality.
Results
710 reports were examined, with 3469 concerns being raised (mean 4.88, range 1–33). 36 reports expressed concern about having to issue repeat PFDs to the same organisation for the same or similar concerns. Thematic analysis reliability was high (κ 0.89 unweighted) with five emerging primary themes: deficit in skill or knowledge, missed, delayed or uncoordinated care, communication and cultural issues, systems issues and lack of resources. A codebook of 53 subthemes were identified.
Conclusions
PFD reports offer valuable insight. Aggregation and continued analysis of these reports could offer more informed patient safety, workforce development and organisational policy. Improved data quality would allow for possible automation of analysis and faster feedback into practice.
Introduction
The Coroners and Justice Act (2009) Regulation 28, 1 allows a coroner in England and Wales to issue a report to an individual, organisations, local authority or government department and their agencies where the coroner believes that action should be taken to prevent further deaths. If a Coroner believes that action should be taken to prevent a future death, they are then under a statutory duty to issue a Prevention of Future Death (PFD) report to the person or organisation that they believe has the power to take action. A single PFD report can be sent to several people or organisations including the relevant regulatory body and the relevant government department or secretary of state.
The person(s) or organisation(s) on receipt of a PFD notice have 56 days to respond. Some coroner’s will often copy the PFD report to other interested persons/organisations to make them aware of the report without requiring a response. Under the authority of the Chief Coroner, PFD reports are published on www.judiciary.uk/ and are in the public domain. Information relating to a deceased person does not constitute personal data and therefore is not subject to General Data Protection Regulations. 2 Occasionally responses to the Coroner are also published but this is entirely at the discretion of the Chief Coroner.
PFD reported concerns range from brief notes approximately a paragraph long, to lengthy and detailed reports. These are issued by individual coroners but when collated are substantial. It is anticipated that by examining PFDs issued for deaths occurring in health in contexts such as hospitals, community and care homes, there may be opportunities for learning and improving patient safety.
In the last published set of data, 2,20,600 deaths were reported to coroners in 2018, the lowest level since 2000 – down 4% (9,100) compared to 2017. The removal of the requirement to report Deprivation of Liberty Safeguard (DoLs) deaths to coroners, in April 2017, is thought to be a reflection of this reduction in reporting when comparing 2018 to recent previous years. 3
Some other countries have made use of such coroner’s findings. For example, in Australia where such data is more structured, insight can be readily gained.4,5 This has been used to gain insight into areas such as medication related deaths in older people’s care. 4 A search of the literature was conducted using Pubmed and other medical databases using search terms “prevention of future deaths reports”, “section 28” and “coroner’s reports” and revealed that no similar systemic analysis had taken place in England and Wales. In addition, search engines such as Google Scholar were utilised to search reports and grey literature on the subject.
The PFD notices in England and Wales could represent a similar resource in terms of improving safety for people in the health and social care system. The aim of this study was examine the feasibility of extracting data from these reports and to evaluate if any learning was possible by establishing if there are, for example, common themes.
Methods
Prevention of future death reports in England and Wales are publicly available from the judiciary website: www.judiciary.uk/publication-jurisdiction/coroner/.
The original study design was to develop a method for automated extraction of data from PFD reports and explore the automation of thematic analysis using techniques such as machine learning.
On initial examination of the data (2016 hospital data) this proved unfeasible. The data is obtained from the judiciary website in different forms most commonly as scans or photographic images of variable quality or occasionally in portable document format (PDF). These appear to be uploaded in batches irrespective of time of inquest. This presents challenges in using any standard data mining technique and also the application of approaches such as machine learning or automation of analysis.
These reports are categorised into several different settings that deaths occur in. Examples include hospital, care home, prison, railway and military related deaths. For this work PFDs reported for hospitals, care homes and a newer community category were extracted.
The care homes category was extracted for four years (2016–2019) and the community for two (2018–2019). This gave 192 reports which were then subjected to descriptive statistics and thematic analysis after extraction. Hospital deaths were extracted for four years (2016–2019) which resulted in 518 reports, although for reasons described above 2016 was only partially extracted. In total 710 full text PFDs were extracted.
PFDs follow a set format and are completed by individual coroners. The structure of the report contains the following sections: This Report Is Being Sent To – commonly an employer, Coroner details, Coroner’s Legal Powers, Investigation and Inquest, Circumstances of Death, Coroner's Concerns – The Matters of Concern, Action Should be Taken, Your Response – the organisation or individuals responsibility to respond and Copies and Publication – who the report is to be copied to including details of public dissemination.
Reports vary in length from a paragraph or sentence to many pages depending on the issues the coroners wish to raise. The section in each report in which the coroner cites concern, actions or recommendations they wish to raise which they may feel prevent a future death was extracted. These data were then subjected to descriptive statistical methods. The concerns were additionally subjected to thematic analysis. Inclusion criteria for extraction were: Hospital Death (Clinical Procedures and medical management) related deaths Care Home Health related deaths Community health care and emergency services related deaths Mental Health related deaths* Alcohol, drug and medication related deaths* Child Death* Suicide* Emergency Services related deaths (from 2019)*
*These categories appear to be additional categories in the website catagorisation and a single PFD may be listed under several categories.
As the Coroner’s office categorisation varies and has changed over the years, other categories may still be identified and added to the above in the future. Exclusion criteria from this study due to relevance were: Road (Highways Safety) related deaths Railway related deaths State Custody related deaths Military related deaths Terrorist incidents Major Incidents
Due to the issues of variability in presentation and format of the reports, the report contents were extracted from the website manually from September 2019 to January 2020 and placed onto an excel spreadsheet.
Data analysis
The primary intended method was to have been the application of data mining techniques. 6 However, on closer inspection of the raw data in the various formats this proved technically challenging and questions around reliability due to data structure and quality emerged. Dates did not always align and extraction of text from images caused significant issues in terms of fidelity. Text extracted from a sample of images did not match text examined manually to any great degree. This would mean that using standard data mining techniques would introduce a high degree of uncertainty in interpretation. The reports were therefore extracted manually to overcome the issues with data quality and structure.
After examining the structure and quality of the data, the application of descriptive statistics and thematic analysis was undertaken. Prevention of future death reports are opinions of the coroner based on inquest findings and so thematic analysis seemed the most pragmatic approach.
Thematic analysis is a straightforward way of conducting hermeneutic content analysis which is from a group of analyses that are designed for non-numerical data. It is a form of pattern recognition used in content analysis whereby themes (or codes) that emerge from the data become the categories for analysis. 7
The PFDs were analysed by three researchers to establish concordance using Cohen’s Kappa for interrater reliability. An inductive approach was used to develop a codebook. Reports were initially read by one clinical researcher to determine themes and then re-read to identify subthemes. In order to establish reliability, a proportion of the PFDs (40% n = 284) were read by two other non-clinical researchers who also identified themes. The emergent codebook had five over-arching themes and 53 thematic code categories.
Results
Data extraction
Seven hundred and ten PFDs met the inclusion criteria. This resulted in 3469 concerns being raised within these reports with a mean of 4.88 concerns per report; however, the range was wide (1–33 concerns).
Care home health related deaths
One hundred and two reports were analysed using thematic analysis. In total the coroners made 569 concerns with a mean of 5.5 concerns per report. There was considerable variance in the scope and depth of issues raised.
Coroners sent 144 notices to 120 to individuals and organisations. The most common notices were to the Care Quality Commission (CQC) (15) and the Department of Health (DoH) (6).
Community healthcare related deaths
Ninety reports were analysed using thematic analysis. In total the coroners made 456 concerns with a mean of 5.1 concerns per report. As with care homes, there was considerable variance in the scope and depth of issues raised.
Coroners sent 169 reports to 137 individuals or organisations. The most common notices were sent to DoH (8) NHS England (5) Welsh Ambulance Service NHS Trust (5) and the CQC (4).
Hospital death related deaths
Two thousand four hundred and forty-four concerns were raised from five hundred and eighteen reports with a mean 4.7 concerns per report. The most common notices were to individual Trusts. The largest single organisations to receive notices in respect of hospital deaths were NHS England (57), DoH (33) the Secretary of State (28) and the CQC (22).
Concerns over repeat reports
36 reports expressed coroners concerns about having to issue repeat PFDs to the same organisation for the same or similar concerns (Table 1). An example of this is given in case 2017–160 in which a coroner expresses concerns regarding the repeated need to issue PFDs (also known as Section 28 notices) to the same Ambulance Service and NHS Trust. The same coroner issued PFDs to one organisation in January 2014, September 2014, November 2015, December 2015, August 2016, January and March 2017 all regarding the delay of handover at an acute hospital due to resource issues.
Coroner’s PFDs mentioning raising repeated concerns to the same organisation.
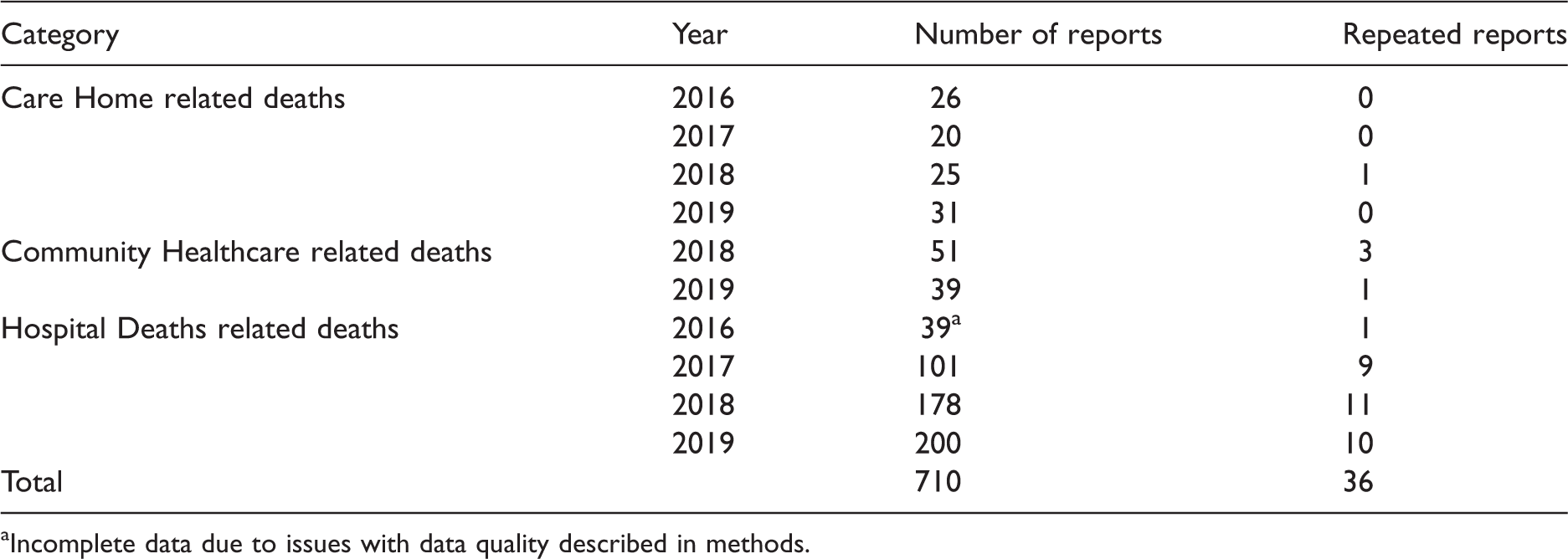
aIncomplete data due to issues with data quality described in methods.
Thematic analysis
This was undertaken by three researchers (Author 1, 100%, Author 2, 40% and Author 5, 40%).
In terms of thematic analysis reliability was high (κ 0.89 unweighted) with five emerging primary themes:
A deficit in skill or knowledge Missed, delayed or uncoordinated care Communication and cultural issues Systems issues Lack of resources
The distribution by setting and years is shown in Figure 1.
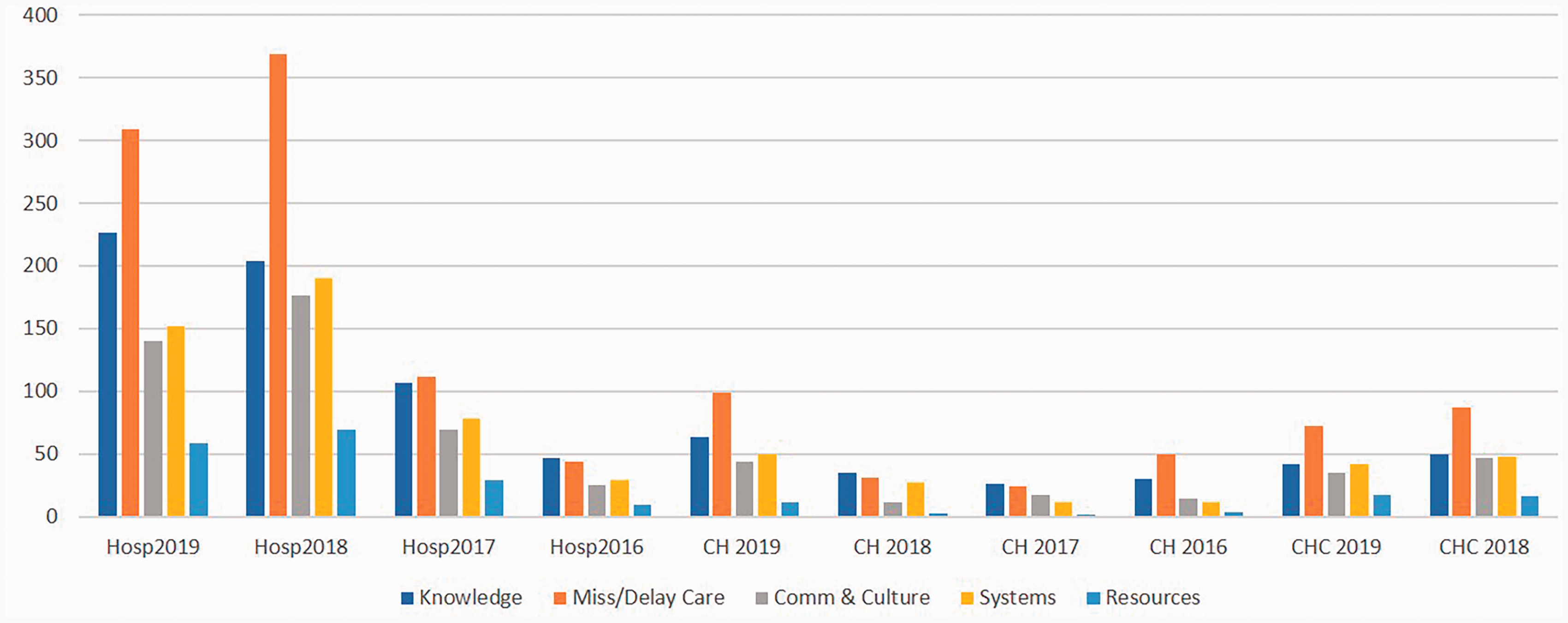
Coroner’s concerns by category and year from 710 PFD reports.
A codebook of 53 subthemes of the five primary themes was identified:
A deficit in skill or knowledge
Deficit in skill or expertise
Failure/ability/education to deviate from algorithmic care or policy when harmful or inappropriate
Failure to be aware of, follow or implement evidence-based guidance
Mis-prescribing
Misdiagnosis
Unnecessary or inappropriate investigations or care
Inappropriate equipment usage
Human error during procedures
Missed, delayed, or uncoordinated care
Care (including investigations and assessments) not done
Care (including investigations and assessments) significantly delayed
Uncoordinated/unmanaged care.
No/poor assessment of care needs.
No or insufficient care plan.
No or insufficient advice on self-care
Inappropriate care setting (no or inadequate assessment)
No or inappropriate medicines management (Polypharmacy/over prescribing/oversupply of medication)
Communication and cultural issues
Failure/refusal to communicate with other team members or agencies
Failure/refusal to communicate with carers/families
Failure to document care
Retrospective documentation both after the fact (question of reliability) or with alleged intent to deceive.
Language or cultural misunderstanding
Inconsistent terminology
Missing notes/documents
Staff stress
Refusal to treat
Dishonesty
Failure or absent leadership
Failure to report concerns to the organisational leaders or regulator
Reactive culture
Systems issues
Ergonomics and design of equipment
Equipment failure
IT unsuitability/failure
Failure to share records in IT platforms across organisations
Unable to access records (paper or IT)
Poor/unsuitable environment
Contracting or financial disputes
Failure to provide care/treatment due to demand management policy/strategy.
Re-organisation of services
No or insufficient learning form internal investigations
Concerns about post-mortem procedures
Medicines unavailability
Out of date applications (“apps”)
Misuse of equipment
Inappropriate use of resources (i.e. police)
Lack of policy/guidance
Regulatory issues
Untraceable staff
No response to coroner
Lack of resources
Equipment missing
No or insufficient staffing
High workloads
Unable to recruit
Lack of staffed beds
Almost all reports (98%, 696) had more than one concern. An example can be seen in case 2018–0044, a patient at an acute trust who died in in 2017. This example cites concerns from four of the five themes multiple times.
There was a failure to escalate and act on [Redacted] deteriorating condition from at least 14.00 on 22 April 2017, when her NEWS was 6, and her GCS is also likely to have dropped. There was a failure to record a single GCS after 14.00, when her level of consciousness dropped. I found no evidence of any clinical or nursing review after this time. There was a failure to discuss [Redacted] condition with neurosurgeons in Nottingham again before she was transferred to Nottingham, when it was clear that her condition had deteriorated significantly. There was a failure to reduce the risks during transfer – a patient with a GCS of 4 and a history of vomiting was handed over to ambulance staff with an unprotected airway and without clinical review, or escort. The trust appears not to have appreciated the significance of these issues. It has not carried out any internal investigation, nor contacted [Redacted] family in line with its duty of candour. I am concerned that there has been no opportunity for learning within the trust, following these serious failures. The trust’s procedure for carrying out High Level Investigations and Serious Untoward Incident Investigations should be reviewed. The trust legal services team did not send the witness (doctor) responsible for reviewing [Redacted] shortly before transfer, as requested. It sent no representative or supporter with, despite the trust being an Interested Person. There was no representative in attendance to hear the conclusions which raised serious concerns.
A major theme was poor or no coordination of care. Good co-ordination of care is associated with better outcomes and increased survival.8,9 A second example is case 2019–0035, a child who died in 2017 in a community setting (general practice) which illustrates the most common themes – a lack of coordinated or continuity of care alongside a deficit in knowledge or action against best practice. An extract from the PFD is shown here:
The medical management of this child's asthma attacks on the innumerable occasions she presented to her general practice and hospital was centred solely on treating the immediate presentation as an isolated acute event seeking its stabilisation and returning her to the care of her family There was:
a. No coordinated record of these occasions b. No analysis of the frequency or circumstances of these events c. No analysis of the underlying chronic asthma condition d. No appreciation of the risk factors for future attacks and death due to asthma in this child e. No long-term management plan for the care of this child despite innumerable attendances for attacks and failure of the parents to bring the child on occasions for routine hospital and practice appointments f. No evidence of provision of a written personal acute asthma self-management plan recommended in the UK BTS/SIGN asthma guidelines g. No evidence that the family were informed of the risks of poor outcome evidence in this child's history h. No evidence that anyone considered referring this child as recommended in the NRAD, to a respiratory specialist or severe asthma service for investigation, characterisation of the nature and phenotype of this child's asthma so that a long-term management and treatment plan could be formulated and implemented i. No clear understanding or awareness by the health professionals caring for [Redacted] of the current UK asthma guidelines, the recommendations of the NRAD or of the prescribing advice in the British National Formulary for the management of asthma
Discussion
Recurring themes emerged from these data which if optimised could offer opportunities to improve safety. The five emergent themes could be a focus for learning and quality improvement.
There are also policy implications from the findings. A deficit in workforce (in either numbers or skill) was evident in these reports. Uncoordinated, delayed or unplanned care, deficits in knowledge and lack of resources where some of the prominent recurring themes.
One of the recurring themes is poorly co-ordinated care alongside lack of resources. Often vigilance, 10 rescue 11 and the management of care would be done by registered nurses however division of labour models of working (i.e. task-based care) have become more common in recent years with the rise of workplace rituals such as “intentional rounding”12,13 which is a different model from other safety critical work which rely more on professional judgment and deference to expertise. 14 This appears to overlap in areas such as the detection or non-detection of deterioration in the themes of skills and missed or delayed care. For example, 24 reports mention NEWS (National Early Warning Score) which is used nationally in England to detect deterioration 15 where coroners remarked on either inappropriate use, non-use, an inability to interpret meaning or act on findings as being of concern.
In 36 reports, coroners expressed concerns or even frustration that learning or action from PFDs was not utilised and that organisations repeatedly appeared before them. The absence of action can be seen in eventual action. For example, one NHS trust had nine PFDs over the period examined, dating back to deaths in 2015. It was not until 2020 that a review of these deaths was finally reported on in terms of an intervention. 16 If PFDs were used as a source of data for patient safety in a systematic way it might be possible to avoid deaths – the original intention of the reporting. Coroners also remark on similar circumstances of death. An example of this can be seen in Case number 2019–0334 who died following a seizure in a bath (a known risk) whilst unsupervised by care staff in 2018. These circumstances were similar to those of Case number 2015–0445 some five years before. There is an obvious policy opportunity here to improve care. Systemic data collection and analysis on similar issues or organisations could form part of an early warning system.
It is interesting to note that the themes arising from PFD reports mirror somewhat the themes that emerge from non-fatal incident reporting. A study by Aaronson et al. 17 used thematic analysis to examine 750 hospital emergency department incident reports. The most common themes were related to delays (138/750, 18.4%), medication safety (136/750, 18.1%), and failures in communication (110/750, 14.7%). A total of 48.8% (366/750) of reports were submitted by nurses. There might be an opportunity to further interrogate incident reporting as a way of improving safety or establishing if such reporting could serve as a forecasting for preventable deaths. The cross-cutting topics for example medicines which appear in the form of mis prescribing and lack of medicine management could be a focus for change. There are estimated to be 237 million medication errors occur at some point in the medication process in England annually and definitely avoidable adverse drug events are estimated to cost the NHS £9,84,62,582 per year, 1,81,626 bed-days, and causing/contributing to 1708 deaths. 18
Coroners often recommended policy or technical training is put in place whilst also stating that there are flaws in this approach for example, when concerns cite lack of skill, willingness or resource to implement an existing policy. Healthcare has made extensive use of policies to try to mitigate risk and coroners frequently mentioned policy or specific technical training to address much wider underpinning safety issues-often but this appears to result in information overload for health care professionals 19 and so a different approach to safety might be more useful. Policy makers could consider approaches used in other safety critical sectors such as the use of this kind of “real world” operational data to better inform structural changes to safety and addressing workforce policy issues such as the reliance on dilution of frontline expertise as the primary method of meeting increasing demand.
Data quality
This study has examined 710 PFD reports in detail as published on www.judiciary.uk/. The reports are not published in chronological order. PFD reports appear to be published some years after the incident which led to the report had taken place. The reports appear to be published in batches from a single Coroner area, so it is common to see a spike in reports published from a single area. It is also not possible to know if all reports are published or there are gaps in these data as there is no centralised database.
PFD reports are all published as Adobe PDF documents, however, it was rare that these were original digital documents, in many cases they are scans of signed pieces of paper. The quality of these scans varies substantially and occasionally the documents are poor quality photographs. This presents a challenge to extract data and does not allow for significant automation, most reports therefore require manual examination. Further issues arise if a Coroner attaches a report, usually a document from the inquest, to the PFD report – these are not included in the published documents and can leave an incomplete picture.
Conclusion
The emergence of common themes indicates there is a substantial opportunity for learning from PFD reports. There is also an opportunity to better inform policy in areas such as workforce (number and skill levels) the safer use of technology, patient safety, communication and the organisation/structure of healthcare services. Policy makers, providers of health and social care, employers and professional bodies could use learning from PFD reports to improve care by addressing the recurrent issues which are also reflected in other datasets such as incident reporting. This learning could be timelier if data quality issues were further addressed in the coronal system allowing for more automated extraction or systematic use of findings.
Footnotes
Acknowledgements
The authors wish to thank Dr M. Alexander, Dr F Healy and Dr S Ryan for their advice and Dr G Julian for review of the manuscript.
Data sharing
Ethical approval
These data were extracted from publicly available data. All data is identifiable and in the public domain including the names of the deceased and coroners. Case numbers that are in the public domain have been used in this report. This is secondary analysis/documentary anlaysis of publicly available data. It was subjected to the Health Research Authority algorithm. It was not deemed as NHS research.
Guarantor
The corresponding author takes responsibility for the integrity of the work and confirms that he controlled the decision to publish.
Contributorship
AL and GP contributed to study design, data collection, data analysis and manuscript preparation. CO and JL contributed to study design and manuscript preparation. DB contributed to data collection, data analysis and manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the Queen’s Nursing Institute who funded the extraction and analysis of care home, community and general practice reports. The extraction and analysis of hospital and other reports was unfunded.
ORCID iD
Geoffrey Punshon ![]() ">https://orcid.org/0000-0001-9247-9546
">https://orcid.org/0000-0001-9247-9546