
Abstract
Objective
To explore different models of clinical–insurer engagement around maternity safety and to understand how state insurers could and should engage with clinical staff to improve outcomes and reduce harm.
Design
Semi-structured interviews and focus groups were conducted with senior representatives from state insurers. Transcripts were analysed to identify different models of engagement. Themes were also elicited from the transcripts. A further one-day focus group allowed for clarification and elaboration of these themes.
Participants
Senior representatives from state insurers in England, Scotland, Wales, Republic of Ireland, Sweden and Victoria, Australia.
Results
A variety of clinical engagement activities were undertaken by the insurers. These included training on claims and risk management, hospital site visits, facilitating multi-professional network meetings and working with clinical experts to develop best practice recommendations. Some insurers engaged with frontline clinical staff through collaborative patient safety programmes. The themes (identity and size, data and research, incentivising improvement and system integration) were important for considering the role of state insurers within health systems and how insurers could engage with clinical teams.
Conclusions
This study identified different examples of clinical–insurer engagement. Whilst this was encouraging, the relationships between insurers and clinical teams could be developed further. Insurers and clinical staff could still collaborate more closely and work together in improving patient outcomes. Whilst not specifically their domain, insurers do have a role in patient safety. Closer clinical collaboration may strengthen this contribution.
Introduction
Across the world, birth is not as safe as it could and should be. Preventable harm is not only a tragedy for the families affected, but with rising treatment and litigation costs, it is a significant drain of financial resources from healthcare systems. In 2016–17, the English National Health Service Litigation Authority paid out £1.7 billion in compensation and fees for clinical negligence claims. Alarmingly, the value of the obstetric claims received in 2016/17 is expected to reach £2 billion. 1 These are claims that no one wants to receive or pay. It is money lost to the healthcare service and patient care. However, these payments, and in particular the prevention of the underlying incidents, may help to drive improvement in health systems. Agencies that provide indemnity insurance for clinical negligence are not patient safety organisations but can have a role in preventing harm and avoiding litigation.2,3 Whilst there is evidence of involvement by both private and state insurers in patient safety initiatives,4–7 there has been little empirical research to understand the strategies employed by state insurers to engage with clinical teams. A better understanding of the different ways state insurers interact with clinicians could be useful in informing future practice. In this study, we explored different models of engagement by examining the work of six state insurers in Europe and Australia. We focused on maternity care given its disproportionate litigation burden – in England, obstetric cases represent 10% of the number of claims but constitute 50% of the total value. 1 Our aim was to describe how different state insurers engage with clinical staff to improve outcomes and prevent harm, and explore how such engagement can be more effective.
Methods
We examined different models of insurer engagement with clinical providers (clinical–insurer engagement) at the following six state insurers:
NHS Litigation Authority (NHSLA) – England Welsh Risk Pool Services (WRPS) – Wales Central Legal Office (CLO) – Scotland State Claims Agency (SCA) – Republic of Ireland Landstingens Ömsesidiga Försäkringsbolag (LÖF) – Sweden Victorian Managed Insurance Authority (VMIA) – Victoria, Australia
These insurers were chosen to compare current practice in England, Wales, Scotland and the Republic of Ireland. Sweden was included to enable comparison with an administrative ‘no-fault’ compensation scheme run by a national mutual insurance company (LÖF). The VMIA was included as it has funded quality improvement initiatives for maternity units across Victoria. 6 The key features of each insurer and the context in which they operate are summarised in Figure 1. Many of the participants did not identify with the term insurer as there are no formal insurance contracts between their organisation and their clients. Indemnifier or reimburser are thus more accurate terms to describe some of these organisations. However, for ease of reference, we refer to all agencies that manage clinical negligence claims and provide compensation as insurers. We defined engagement to include any sort of partnership or relationship which is specifically focussed on improving safety and outcomes.
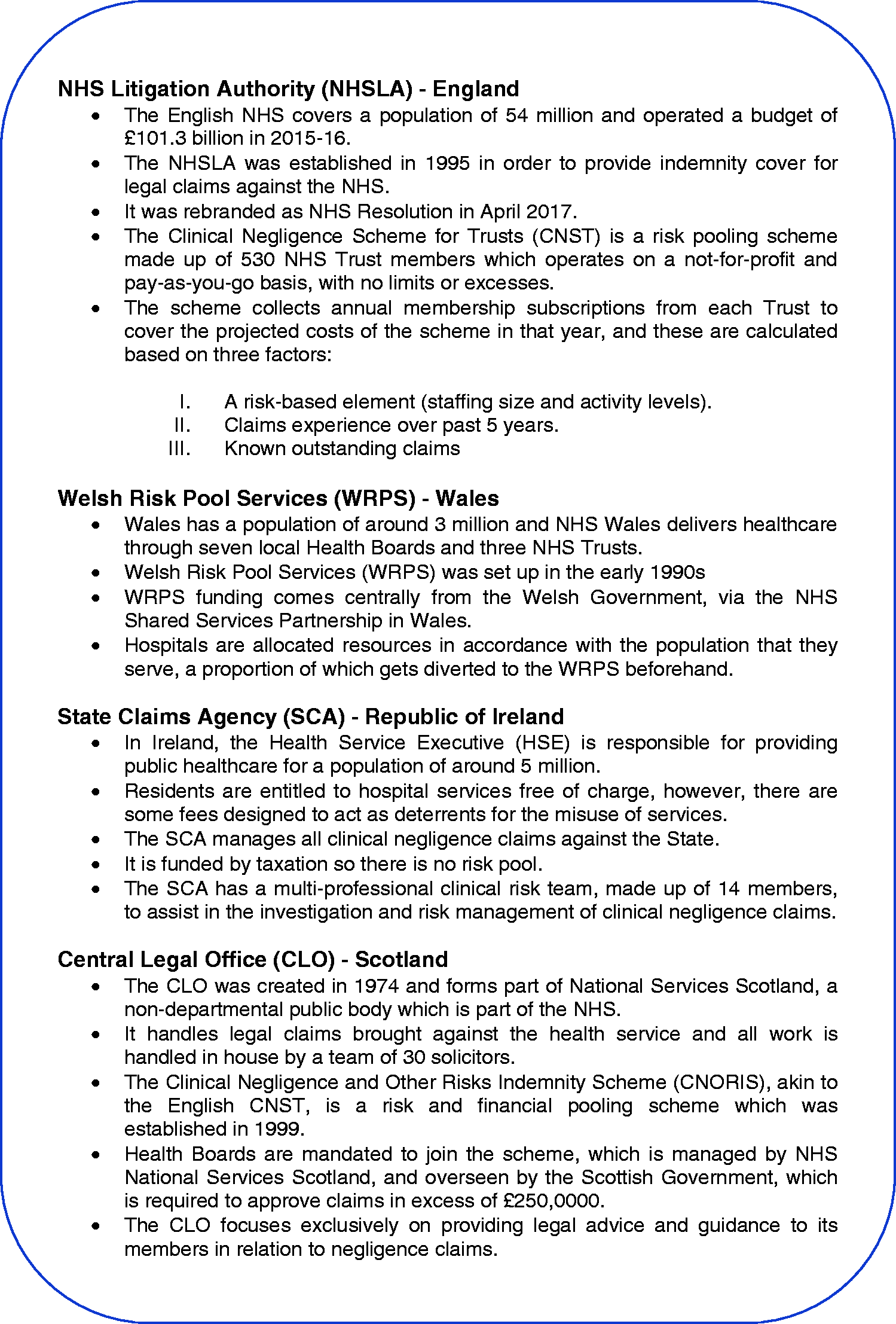
Key features and context of insurers.
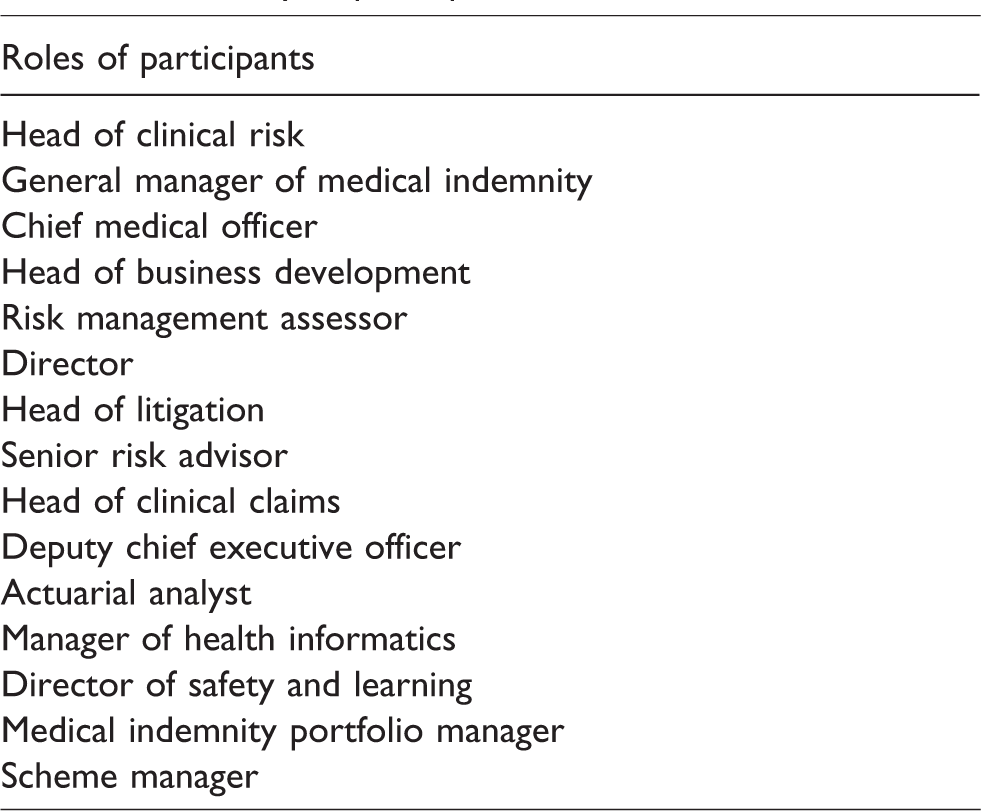
We carried out semi-structured interviews (with one participant) or focus groups (with more than one participant) with senior representatives from each insurer. To maintain confidentiality, the names of the participants and their affiliations have not been provided. However, the roles of the participants from all six state insurers have been listed in Table 1. The interviews/focus groups took place between August 2016 and February 2017 and were conducted by OQ (Reader in Law) and CY (Obstetric Registrar and Research Fellow). The exception was for the VMIA, where CY facilitated focus groups. A basic topic guide (see Appendix 1) was utilised at each interview/focus group. All interviews/focus groups were audio-recorded when permission was given (all except one) and were transcribed. Analysis was supported by a one-day focus group with all participants who provided feedback on our preliminary analysis of the data and an opportunity for collective reflection on the emerging themes.
Summary of participant roles.
We followed a Grounded Theory approach, defined as the ‘discovery of theory from data systematically obtained from social research’. 8 This approach is well suited to investigating areas such as this where there is limited existing research. The transcripts and field notes were analysed independently by both researchers before observations were compared and themes identified. There was a high degree of similarity in terms of our observations and no disagreements within the research team in identifying themes from the data. We employed deviant case analysis (i.e. whenever a theme or categorisation was identified within the data, each interview was re-examined for counter-examples and disconfirming data). This afforded greater confidence that the identification of themes was trustworthy and reduced bias. Ethical approval was obtained from the University of Bristol Faculty of Health Sciences Research Ethics Committee. Participants were provided with information leaflets regarding the study and written consent was obtained prior to the interviews/focus groups.
Results
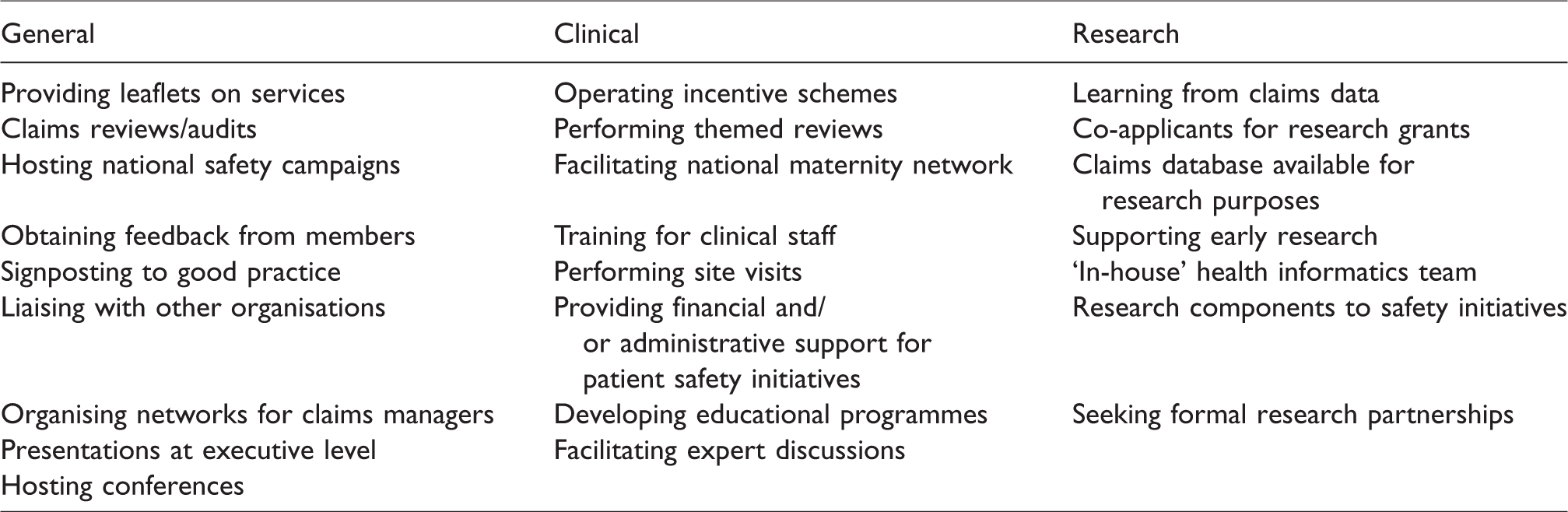
Insurers were involved in a wide variety of engagement activities. We classified these into ‘general’, ‘clinical’ and ‘research’ engagement. All insurers participated in general engagement activities, for example providing claims data to hospitals, conducting claims reviews, and hosting quality and safety conferences. There were also a range of initiatives and projects whereby insurers attempted to engage with clinical staff and also support research activity. All engagement activities discussed by the insurers are summarised in Table 2.
Summary of engagement activities.
There was no consensus amongst respondents on the best way of ensuring effective clinical–insurer engagement. Whilst there was no lack of activity, there was an acknowledgement that engagement with frontline clinicians (as opposed to managers) is challenging and somewhat under developed. This was reflected in the following quotes from respondents at the NHSLA: "What do we need to do to be engaging with the clinicians on the ground? How can we best develop and start to move things forward?" "I think in an ideal world we would have really pulled off much closer clinical engagement, and if I’m being realistic, I’m not sure we’d do it at hospital level but there’s the potential to do it at speciality level." "We work with midwives, infectious specialists, obstetricians, primary GPs. We reach them via their professional organisations, and our role here is to administer and support financially. Then hopefully we get the perfect marriage here."
A strong feature of the approach of LÖF was its emphasis on inspiring appropriate professional norms around learning and improvement as opposed to being overly prescriptive: "We’re quite cautious about telling – it’s not that we say, for instance, 'LÖF does not say that you should do it this way.' We don’t say that. We say that we have helped the professionals to find the best practice to do it and we have supported them…So, what we actually work with there are professional norms. 'We help the professions to develop their professional norms. ‘It’s okay to do it this way. It’s not okay to do it this way.' " "I think it’s also important to stress that we always try, if it’s possible, to find a way to compensate. That’s how we work. We are not here to save money. That’s important to save money. We just want to make sure that if we can pay compensation we should do that and try to find a possibility. So, we don't want to be this ugly insurance company that just wants to fool everyone. We really want to help people."
Even within the fault-based system in the UK, there were important differences in terms of the mechanics of paying for claims. In England, Hospital Trusts pay a premium to be members of an indemnity scheme (the Clinical Negligence Scheme for Trusts) which is administered by the NHSLA. This means that the NHSLA takes responsibility for managing claims and paying out compensation. Whereas in Wales, if a settlement is agreed, the hospital pays the settlement first, before applying to the WRPS for reimbursement. Hospitals are only reimbursed if an adequate learning plan has been implemented and WRPS has the power to delay or even refuse reimbursement at its discretion.
"It is a sanction that is used so they know it is used" (on discussing the possibility that hospitals may not be reimbursed after paying a claim).
In the Republic of Ireland, the reporting of any adverse healthcare incidents to the SCA is a statutory requirement. Whilst there is no formal penalty for non-compliance, if a claim is not preceded by an incident report, the SCA can decline to cover the cost of the claim and the hospital would have to pay out themselves.
Engagement appeared to be easier in smaller health systems. Respondents from Wales made repeated reference to the relatively small size of their health systems and their ability to get to know key clinical personnel. "I think because Wales is smaller we’ve been able to have a better handle on the risk management and the training and the lessons that come out of the claims." "From the point of view of claims management, it’s easier in a smaller place where you have only about 10% number of the claims and just geographically, it seems easier to manage." "Data is only going to start to signpost you to look at which stone you might want to turn over. It’s not going to tell you how to fix those problems necessarily." "So, we can capture more and more data if we want, we can capture more and more granular data but is it going to necessarily take us that further forward in terms of actually supporting and engaging with people on the ground to improve? It might give them more tools but more information about what they already know is an issue isn't helping them solve that issue whereas the provision of potential support [or] intervention…to help them get past that would be, I think, a really positive step towards that improvement."
"We want our patient safety activities to be data-driven. Targeted work, we can’t work with everything, so we have to be selective."
Finally, many of the insurers seemed to take a proactive approach to risk management and the recent rebranding of the NHSLA to NHS Resolution,
12
with its focus on learning and prevention, is evidence of this. "Yeah, we’re insurers and we’re there to make sure that the clients are well looked after when things go wrong but, at the same time, we see our role to prevent that harm happening in the first place." "So, all of the players, whether you’re the national lead for maternity for NHS England or you’re in improvement or you’re here, we’ve all got the same aim…whatever we can possibly do in a combined way to reduce harm." "A dollar’s a dollar at the end of the day but if we’re preventing harm/saving lives it’s a whole different story and I think it generates more enthusiasm for all of us knowing that we’re looking for something that’s going to help."
Discussion
This study demonstrated that state insurers participated in a wide range of general, clinical and research engagement activities. There were many models of clinical–insurer engagement but there was a strong sense that this relationship could be improved further. Our analysis of the responses allowed us to identify the following themes which appear to be centrally important for effective clinical–insurer engagement: insurer identity and size, their use of data and commitment to research and how they attempt to incentivise improvement and integrate the system.
Insurer identity and size
A fundamental question surrounds the identity of each insurer and what they regard as their main priorities. Whilst all the insurers are responsible for protecting the interests of their members, both financial and reputational, they must also compensate patients for negligent or avoidable harm. This raises the significant challenge of how insurers can satisfy all of these different stakeholders whilst maintaining their trust and confidence. Balancing the interests of patients (particularly those who bring claims) whilst defending the financial interests of the health system is particularly challenging. Apart from LÖF, which operates within a system which provides an entitlement to compensation for avoidable harm, the other insurers have operated within systems which have (historically) been focused on denying or defending claims. It is important not to overlook the impact of these different systems on how insurers identify themselves and what they consider to be their main priority. For example, LÖF functions as an insurance company which essentially regards patients as its customers and attempts to resolve claims to their satisfaction. This contrasts with the approach of insurers in fault-based systems which have tended to focus on satisfying its clinical provider members. We would tentatively suggest that no-fault systems, with an emphasis on efficient resolution of claims and a less adversarial approach, are more conducive to effective clinical–insurer engagement.
Effective engagement also appeared to be easier in smaller health systems. It was a foreground assumption of this research that engagement might be easier in smaller health systems, and the responses appear to confirm this. One of the explanations for the positive examples of engagement in Sweden and Victoria is the relatively small size of their health systems. This presents challenges for such engagement in bigger health systems such as the English NHS and raises the possibility of larger insurers operating at regional level in order to help facilitate more effective engagement.
Data and research
Claims data can complement clinical data and improve the potential learning from harmful events. However, data collected for claims purposes are limited in a number of ways. First, it presents a skewed picture in only focusing on failure rather than success. Second, given the time lag between the incident date and the claim date, it may not accurately reflect the safety of current care being delivered. Third, such data are collected for narrower legal rather than much broader clinical purposes. Combining clinical and claims data would be challenging given the need to integrate many different databases. Insurers and clinicians should work in partnership to carefully design an accessible system that will facilitate, rather than impede, the analysis of claims and clinical data together. This would result in more data being converted into meaningful information. Furthermore, a consensus on the taxonomy to be used between insurers and clinicians worldwide would encourage data sharing and the formation of larger datasets. This would increase opportunities for learning and foster a greater sense of collaboration.
In addition to developing a better way of using data, insurers could work more closely with clinical experts and draw on academic expertise in designing patient safety research. In particular, insurers could fund collaborative research projects as part of their risk mitigation initiatives.6,7 The VMIA has supported the implementation of a multi-professional obstetric emergencies training programme (PROMPT) throughout Victoria. Each participating unit received funding from the VMIA to help with training costs. An initial analysis found that the programme was associated with improvements in staff attitudes towards safety, teamwork and perception of management. There were also significant improvements in some clinical outcomes during or after training. 6 The VMIA is currently collaborating with a UK charity (PROMPT Maternity Foundation) to evaluate the state-wide impact of this training package.
Incentivising improvement
Incentives can play an important role in encouraging improvement but there is no agreement on the perfect model for this. Though not formal regulators, insurers can exert some regulatory influence by setting targets (such as adopting evidence-based patient safety programmes) linked with monetary and administrative incentives. 14 Other financial incentives could be in the form of premium discounts or returns subject to certain assessment criteria. The NHSLA previously offered discounts of up to 30% on hospitals’ premiums if their standards were met. These were process measures covering governance, learning, workforce, environment, training and procedures. 15 These discounts and standards were eventually stopped as there was no clear correlation between compliance with standards and better outcomes.16,17 Eligibility for discounts on premiums, therefore, should include assessment of both processes and clinical outcomes.
There is a considerable time lag in maternity claims between the incident and settlement, usually due to the time needed for a diagnosis and long-term prognosis to be made. As a result, premiums charged to maternity units may still be influenced by previous events, even if care has significantly changed since they occurred. There is an argument that premiums are too backward looking and do not reward current, good practice. Future pricing strategies should take this into consideration.
Non-financial incentives can also be very powerful and could include releasing data for regional/national benchmarking or promoting professionalism. Such incentives could be considered universal and not reliant on pricing strategies or premiums. Negatively focused incentives such as imposing penalties on substandard care may also be utilised. These measures, however, may perpetuate poor care by punishing those that need help in improving.
Further exploration of different incentive models, including their evaluation and implications for policy, is clearly required. Insurers have the financial resources and administrative capacity to help develop and run incentive schemes. Crucially, from these interviews and focus groups at least, there appeared to be a growing appetite for new and better incentive plans, as demonstrated by proposals in England to introduce a new discount scheme in 2018/19. 18 Insurers, hospital staff (both clinical and managerial) and other key agencies in the health system should all be involved in the co-design of future incentive models. This would ensure system-wide coherence of objectives, which are realistic and relevant to frontline services.
System integration
Many people and agencies in a health system contribute towards patient safety. However, an overcrowded system may hinder rather than enhance quality improvement efforts. Poor communication and inadequate sharing of information between clinical teams or organisations may lead to time wasted on reinventing solutions that already exist elsewhere. 19 The existence of too many local processes creates more variability within a health system, which may perversely undermine patient safety. 19 The regulatory sector is similarly congested. Many regulators have overlapping roles and often duplicate data requests unnecessarily. This bureaucratic burden wastes time and resources for both the regulators and those being regulated. 20
A more co-ordinated approach would help to align the aims throughout a health system. Patient safety and quality of care are more likely to improve if all the drivers in the system – for example, policy, training, incentivisation and regulation – are pointing to the same objectives. 21 An insurer is only one stakeholder, amongst many others, in the pursuit for safer patient care. Despite this, insurers may be ideally placed to facilitate system integration through their multi-level contacts and financial power. Insurers could work together and liaise with organisations at all levels of the health system.
This research is subject to some limitations. The study design was limited to understanding engagement from the perspective of key personnel at insurers. No account was taken here of the perspectives of clinicians or managers. Another limitation is the small sample size of state insurers we selected to participate in this study. As the insurers were purposefully chosen, there will be an element of selection bias and our findings may not be as representative as they could be. Data saturation was also unlikely to have been achieved through interviewing six state insurers, though our sample size was limited by the time and resources assigned for this work. Despite the limitations, there has been little, if any, research in this area previously so this work offers preliminary insights into how some state insurers currently engage with clinical teams, which other insurers may find helpful.
Conclusion
To conclude, this study identified different models of clinical–insurer engagement, which include training clinical staff on claims and risk management, hospital site visits, facilitating multi-professional network meetings and working with clinical experts to develop best practice recommendations. Some insurers, notably the VMIA and LÖF, have mainly engaged with frontline clinical teams through collaborative patient safety initiatives. These projects were supervised by clinical experts from the start and some appear to have had beneficial effects on outcomes 6 or litigation. 7 Whilst it was encouraging that many examples of clinical–insurer engagement were elicited, there is scope for this dynamic to be developed further.
Analysing the way that different insurers currently work has allowed us to develop recommendations for how state insurers could play a more effective role within the healthcare system and how they may use different levers to affect patient care and safety. These recommendations fall within the categories listed below. Insurers could:
○ By using their system-wide contacts and influence to coordinate and prioritise health-related initiatives ○ By signposting members to possible solutions or directing them to relevant contacts ○ To create ways to combine clinical and claims data ○ Implement safety initiatives with proven clinical effectiveness ○ Undertake translational research together, with the aim of applying this to multiple settings
○ By providing administrative support in collaborative projects ○ By identifying problematic areas to focus on through claims analyses ○ By supporting collaborative research
○ By providing monetary support/incentives for safety initiatives with proven clinical effectiveness ○ By providing premium discounts (where applicable) when certain assessment criteria are met ○ By adjusting their premium models (where applicable) to influence current practice ○ By supporting regional/national benchmarking ○ By reaffirming professional pride and professionalism
Whilst this study primarily focussed on maternity care, these recommendations may also be relevant in other medical specialties. Insurers and clinical teams could and should collaborate more closely to achieve their common goals: improving patient outcomes and reducing costly payouts.
Footnotes
Authors’ contributions
TD conceived the original idea for the study and secured funding. CWHY and OQ conducted the interviews/focus groups. All authors contributed to the one-day focus group. CWHY and OQ performed the analysis and drafted the manuscript. All authors provided critical review and approval of the final manuscript.
Acknowledgements
We would like to thank all of the insurers and their representatives for their interest and participation in this study. We are also grateful to Louise Austin for transcribing the discussions during the one-day focus group with all the participants.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TD is a Trustee of the PROMPT Maternity Foundation, a UK-based charity that undertakes research, distributes the PROMPT ‘Course in a Box’ and runs PROMPT ‘Train the Trainers’. TD and CWHY are partially funded by the PROMPT Maternity Foundation on a secondment basis from North Bristol NHS Trust. OQ has no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Foundation (award number 7663).
Patient consent
Patient consent was not required for this study.