
Abstract
Background:
Intermittent exotropia (IXT) is a prevalent strabismus in Asian children. While surgery is the main treatment, its long-term success can be influenced by postoperative exodrift. Therefore, accurately assessing this exodrift is essential to determine the optimal early postoperative alignment.
Objectives:
To investigate postoperative exodrift changes following unilateral lateral rectus recession combined with medial rectus plication (RP) procedure for children with basic type intermittent exotropia (IXT).
Design:
Retrospective, Cohort study.
Methods:
A retrospective review was conducted on the clinical data of patients with basic type IXT who underwent surgical intervention between 2022 and 2023, with a minimum follow-up of 12 months. Based on the postoperative ocular alignment at near within the first week, patients were divided into three groups: Group exo with exodeviation equal or exceeding 5 prism diopter (PD); Group ortho with exodeviation or esodeviation less than 5 PD; and Group eso with esodeviation equal or exceeding 5 PD. The successful motor outcome was defined as exodeviation or esodeviation equal to or less than 10 PD. The recurrent exotropia was defined as exodeviation exceeding 10 PD, and consecutive esotropia was defined as esodeviation exceeding 10 PD. The clinical features associated with motor outcomes and sensory outcomes were analyzed.
Results:
Final exodrift magnitudes were comparable across groups: Group exo (distance: 10.18 ± 10.55 PD, near:7.71 ± 9.82 PD), Group ortho (distance: 8.27 ± 7.23 PD, near: 9.13 ± 8.13 PD), Group eso (distance: 12.50 ± 10.71 PD, near: 12.80 ± 11.69 PD), (p = 0.149 for distance; p = 0.157 for near). Patients exhibiting overcorrection and ortho during the early postoperative period tended to have a better motor outcome compared to those undercorrection. Fusion function improved significantly regardless of the early postoperative ocular alignment (p < 0.001).
Conclusion:
Children with basic type IXT who exhibit varying ocular alignment in the early postoperative period demonstrated a comparable magnitude of 10 PD for long-term exodrift. It is recommended to overcorrect within the range of 0 to 10 PD following RP techniques.
Introduction
Intermittent exotropia (IXT) represents one of the most prevalent forms of exotropia observed in children. The prevalence of IXT among individuals under the age of 19 in the United States is approximately 32.1 per 100,000, 1 whereas the prevalence among Chinese children is reported to be 4.69%, 2 suggesting a higher incidence in the Asian population. Current conservative management strategies for IXT include observation, correction of refractive errors, occlusion therapy, overcorrection with minus lenses, prism therapy, and visual training. In cases where patients exhibit poor control, leading to decompensated fusion and stereopsis dysfunction, surgical intervention is generally considered. Surgical treatments for IXT mainly include bilateral lateral rectus recession (BLR), unilateral lateral rectus recession combined with medial rectus plication (RP), and unilateral lateral rectus recession combined with medial rectus resection (RR).
The selection of surgical techniques for IXT depends on classification. Medial rectus resection and medial rectus plication are both frequently chosen as strengthening procedures for basic type IXT. Alkharashi 3 reported that the success rate of RP is inferior to that of RR, attributed to the recurrence of exotropia due to exodrift. Some studies propose that a slight overcorrection during the early postoperative period may reduce exodrift and enhance the long-term success rate.4,5 However, excessive overcorrection in the early postoperative period probably risk of consecutive esotropia, damage to binocular vision function, and adversely affects the long-term outcomes of the surgery. Very few studies reported the influence of early postoperative ocular alignment on exodrift following RP. Therefore, we aim to investigate postoperative exodrift changes following RP procedure, thereby providing the optimal early target ocular alignment evidence-based data for the future.
Materials and methods
In this study, children with basic-type IXT who underwent RP technique by the same surgeon between January 2022 and December 2023 were included. The inclusion criteria for the study were as follows: participants aged between 3 and 18 years, completed amblyopia treatment before surgery (BCVA ⩾ 1.0), a minimum of three follow-ups postoperatively, long-term follow-up at least 12 months, and with records of binocular visual function at the final visit. The exclusion criteria encompassed: a history of previous ocular surgery, the presence of vertical strabismus, torsional strabismus, A-V type strabismus, nystagmus, dysfunction of the oblique muscles, abnormal eye movements, developmental delays, or any neurological disorders. All surgeries were administered under general anesthesia. Based on the maximal deviation angle, RP was performed using a surgical formula based on the surgeon’s experience (Table 1).
Surgical dose of LR recession and MR plication.

The clinical data collected at each visit included age at the time of surgery, gender, uncorrected visual acuity, best corrected visual acuity (BCVA), refraction (D), binocular visual function, and the angle of deviation (prism diopter [PD]). These measurements were taken during various stages: preoperative, early postoperative (1–7 days), mid-term postoperative (3–6 months), and long-term postoperative (exceeding 12 months). The prism and alternate cover test (PACT) was employed to assess the angle of deviation at distance (6 m) and near (33 cm) after correction. In addition, the fusion was evaluated using synoptophore and Worth’s 4-dot test. Stereopsis was measured with the Titmus stereo test.
We represent residual exodeviations with a negative sign (−) and esodeviations with a positive sign (+). Based on the postoperative ocular alignment at near within the first week, patients were divided into three groups: ① Group exo: angle of deviation ⩽ −5 PD; ② Group ortho: −5 PD < angle of deviation < +5 PD; and ③ Group eso: angle of deviation ⩾ +5 PD. According to the angle of deviation at the final follow-up after surgery, the successful motor outcome was defined as horizontal exodeviation or esodeviation equal to or less than 10 PD at near or distance, recurrent exotropia defined as exodeviation exceeding 10 PD, and consecutive esotropia defined as esodeviation exceeding 10 PD. Without stereopsis or stereoacuity greater than 100 arcseconds, was defined as stereopsis deficiency; and stereoacuity less than or equal to 100 arcseconds, was defined as fine stereopsis.
All analyses were performed with statistical software (IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp). The Kolmogorov–Smirnov test was applied to test the normality of consecutive data. Continuous values with normal distribution were expressed as mean ± SD, and one-way ANOVA was used for comparison between groups. Continuous values with non-normal distribution were compared between groups using the Kruskal–Wallis test, and the Bonferroni post hoc test was employed for further pairwise comparisons. We performed chi-square test or Fisher’s exact test to compare categorical data between groups. Survival curves were plotted using the Kaplan–Meier survival analysis, and the differences in postoperative cumulative survival rates between groups were compared using the log-rank test. Statistical significance was indicated by a p value less than 0.05.
As a retrospective study, no prospective sample size calculation was performed. However, to assess the adequacy of the included cohort, a post hoc power analysis was conducted. Based on detecting a clinically meaningful difference of 10 PD in exodrift,6,7 with an assumed standard deviation of 10–12 PD, an alpha of 0.05, and 80% power, a minimum of approximately 52 subjects was required. Our final sample of 93 consecutive patients exceeds this estimate, confirming sufficient power for the primary analyses.
Results
Demographic and clinical characteristics
The study comprised a total of 93 patients diagnosed with basic type IXT and underwent RP procedure, with the mean postoperative follow-up period of all patients being 16.81 months. Based on their ocular alignment observed in the early postoperative period, with 17 cases in Group exo, 56 cases in Group ortho, and 20 cases in Group eso. The mean age at the time of surgery across the three groups was 8.06 ± 3.05 (range, 3–15) years old. The three groups had no statistically significant difference in demographic and clinical characteristics (p > 0.05 for all; Table 2).
Demographic and clinical characteristics among the three groups.

One-way ANOVA.
Pearson χ2 test or Fisher’s exact test.
Kruskal–Wallis test.
Comparison of postoperative exodrift
Based on the postoperative ocular alignment at near within the first week, the mean early postoperative deviation for the three groups was −7.24 ± 2.80 PD for Group exo, −0.73 ± 1.72 PD for Group ortho, and 8.65 ± 4.45 PD for Group eso, respectively. The longitudinal follow-up data revealed that the exodrift exhibited a stable magnitude throughout all time intervals, and there was approximately an exodrift of around 10 PD, regardless of the early postoperative ocular alignment (p > 0.05) (Table 3, Figure 1).
Postoperative exodrift after RP procedures among the three groups.


Comparison of the postoperative exodrift among the three groups (a) 6 m; (b) 33 cm.
Comparison of long-term ocular alignment
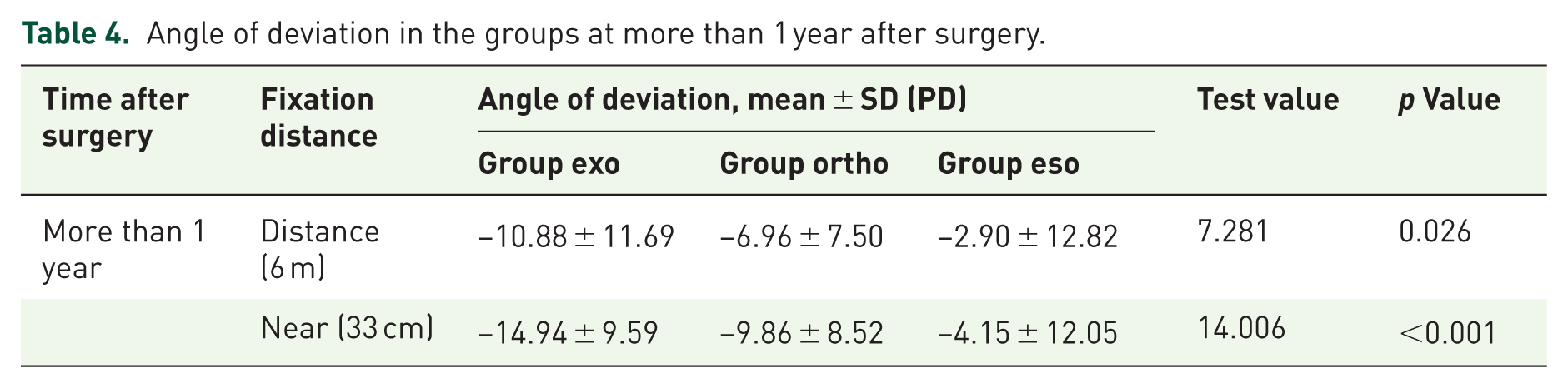
A comparative analysis of long-term postoperative ocular alignment at the final follow-up revealed that patients who initially experienced overcorrection displayed a markedly reduced angle of deviation at both distance and near for the last visit. (H = 7.281, p = 0.026 for distance; H = 14.006, p < 0.001 for near; Table 4).
Angle of deviation in the groups at more than 1 year after surgery.
Comparison of long-term motor outcomes
The overall success rate across the three groups of patients amounted to 66.67%. In detail, Group exo achieved a success rate of 52.94%, Group ortho achieved 71.43%, and Group eso achieved 75.00%, respectively. No significant statistical differences in motor outcomes were observed among the three groups (χ2 = 6.784, p = 0.148). Notably, nearly half of the patients in Group exo (47.06%) experienced undercorrection, while in Group eso, 1 case (5.00%) had overcorrection over the long term. The mean postoperative follow-up for all patients was 16.81 ± 8.23 months, and 15.77 ± 7.21 months for Group exo, 17.15 ± 8.77 months for Group ortho, and 16.73 ± 7.74 months for Group eso, respectively. There was no statistically significant difference in follow-up among the three groups (p > 0.05).
“Survival” was defined as an angle of deviation ranging from −10 PD to +10 PD. With postoperative follow-up as the time variable and postoperative deviation as the survival outcome, the Kaplan–Meier curve was plotted (Figure 2), which estimated the mean time to failure outcomes for Group exo, Group ortho, and Group eso to be 11.01, 21.17, and 21.47 months postoperatively, respectively. Over time, patients who exhibited ortho or overcorrection in the early postoperative period demonstrated a higher tendency of successful outcomes and maintained alignment for a longer duration compared to those who were undercorrected initially postoperatively. However, the results showed no statistically significant difference in cumulative survival rates among the three groups (log-rank test: χ2 = 2.381, p = 0.304). Furthermore, the survival curve indicated that regardless of the early postoperative ocular alignment, the patients’ angle of deviation generally stabilized around the 15th month after surgery.
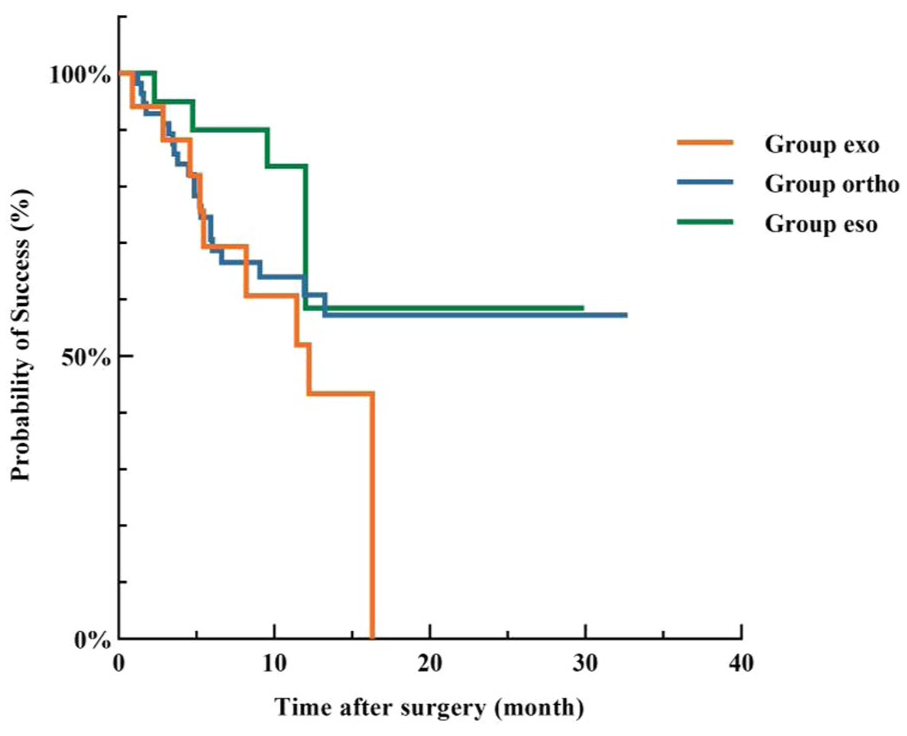
Kaplan–Meier survival analysis for failure motor outcomes among the three groups (p = 0.304, log-rank test).
Comparison of sensory outcomes
88.17% of patients achieved fusion at the last visit. In Group exo, the percentage of patients exhibiting fusion increased from 23.53% preoperatively to 82.35% postoperatively. Similarly, in Group ortho, this percentage increased from 25.00% to 89.29%. In Group eso, the percentage of patients with fusion was 20.00% preoperatively, which improved to 90% postoperatively. Notably, regardless of early postoperative ocular alignment, all three groups exhibited improvements in fusion at the last visit.
Regarding fine stereopsis, Group exo showed an increase from 64.71% preoperatively to 88.24% postoperatively. In Group ortho, the proportion of patients with fine stereopsis improved from 64.29% to 89.29%. Group eso had a preoperative fine stereopsis rate of 65.00%, which increased to 85.00% postoperatively. All three groups demonstrated improvements in fine stereopsis following surgery, culminating in an overall rate of 88.17% of patients achieving fine stereopsis at the last visit. However, it is important to note that a statistically significant difference in fine stereopsis was observed only within the group of patients exhibiting early postoperative ortho when comparing preoperative and postoperative proportions of patients with fine stereopsis.
Discussion
Surgery is recognized as one of the vital treatments for IXT. The previous studies indicate that the success rates associated with IXT surgery are variable. Among the various factors influencing success rates, exodrift emerges as a significant factor. However, differences in surgical techniques, the period of postoperative follow-up, and the definitions of “success” across studies, and the amounts of exodrift are diverse, the success rate for RP reported ranging from 55% to 64%.3,8–11 While our study indicates an overall success rate of 68.82%, it aligns closely with existing literature. By contrast, the success rate for RR is reported to be 76.67%, surpassing that of RP (66.67%). 12 However, this result does not necessarily suggest that the RR procedure possesses an irreplaceable advantage over RP. Anand 13 considered that RP offers certain benefits in the surgical treatment of IXT. RP avoids tendon transection, minimizes intraoperative hemorrhage, and leads to mild postoperative inflammatory responses. In addition, RP can enhance muscle strength while maintaining its structural integrity and allows for the simultaneous intervention of multiple muscles within the same eye.
Some researchers have confirmed that following IXT surgery, ocular alignment tends to gradually drift outward, probably leading to recurrence of exotropia. This phenomenon results in a significant reduction of the long-term success rate. 14 Therefore, some doctors suggest that early postoperative overcorrection is essential, as it may help to neutralize the trend of exodrift and improve the long-term success rate of the surgery. 15 Previous studies have indicated that the recommended amount of overcorrection should be between 0 and 20 PD. 16 However, further studies suggest that the target ocular alignment for overcorrection needs to be based on the surgical techniques. Lee 17 considered early overcorrection, ranging from 11 to 20 PD following BLR and 1 to 10 PD after RR, is optimal for long-term success. To achieve the desired early target ocular alignment, it is necessary to adjust the surgical amount calculated using the Parks’ formula. It is recommended to increase the recession amount of the lateral rectus muscle by 1.5–2.5 mm beyond the traditional surgical table,18,19 and for muscle plication, augmenting the surgical dose by 2 mm beyond the initially planned resection can yield a more favorable correction outcome. However, because excessive overcorrection can increase the risk of suppression scotoma and monocular fixation syndrome, potentially resulting in consecutive esotropia, amblyopia, and stereopsis impairment,20,21 determining the optimal overcorrection in the early postoperative period in the case of children is a challenge.
In our study, the three groups of patients exhibiting varying early postoperative ocular alignment experienced nearly comparable exodrift with time for both distance and near, approximately 10 PD throughout the follow-up period. In addition, the mean time to failure outcome for patients exhibiting early postoperative undercorrection was 11.01 months, shorter than the 21.17 months for the ortho and 21.47 months for the overcorrection during early postoperative. Our study found that patients who presented with ortho or overcorrection early postoperatively were more likely to achieve favorable outcomes compared to those with undercorrection. These patients demonstrated a greater capacity to maintain alignment, with stabilization occurring around 15 months postoperatively, at which point no further exodrift was noted. The results suggest that sustaining early ocular alignment within the range of 0–10 PD following RP is advisable, as it appears to optimize long-term ocular alignment without the risk of consecutive esotropia under a similar exodrift amount. Therefore, augmenting surgical dosage or utilizing adjustable suture techniques to achieve slightly early overcorrection is worth investigating in the future. In our study, the final follow-up results showed that regardless of early postoperative ocular alignment, there was a notable improvement in sensory outcome across all groups. This result demonstrates that even if postoperative exodrift and recurrence of exotropia, the reduction in the angle of deviation still enhances binocular vision function in patients with IXT.
The limitations of our study include, it was a retrospective study, with a small sample size and unbalanced distribution across the three groups, and the period of follow-up is relatively short. In addition, some parameters, such as AC/A ratio, post-patch PACT, and lateral incomitance, were not part of our standard preoperative protocol for IXT. In the future, prospective studies with a larger sample size, inclusion of these key parameters, and a longer follow-up are needed.
In conclusion, children with the basic type IXT who exhibit varying ocular alignment in the early postoperative period demonstrate a comparable magnitude of long-term exodrift. It is recommended to overcorrect within the range of 0 to 10 PD during the early postoperative period following plication techniques, which is more likely to maintain ortho for a longer period and enhance the long-term success rate. Furthermore, even if the long-term motor outcomes are unfavorable, a reduction in the angle of deviation can still improve binocular function postoperatively.