
Abstract
Purpose:
To compare the preoperative clinical features in patients with basic unilateral exotropia who underwent single versus two and three or more strabismus surgeries.
Design:
retrospective
Method:
Two thousand four hundred fifty-seven patients with unilateral basic exotropia were recruited over 10 years. Of these, 1886 (76.8%) had one surgery, 411 (16.7%) had two, and 160 (6.5%) had three or more surgical interventions. Preoperative data included the best corrected distance visual acuity (BCVA), refractive error, magnitude of exotropia, and amblyopia type and severity.
Results:
The mean age at first surgery was 26.3 ± 13.35 years (age range: 2–77) with no significant difference between groups with one, two, and three or more surgeries (p = 0.770). Mean BCVA in the strabismic eye was significantly worse in patients who underwent three or more surgeries (0.82 ± 0.076 logMAR) than those who had one (0.55 ± 0.018 logMAR; p < 0.001) or two surgeries (0.52 ± 0.038 logMAR; p < 0.001). Spherical equivalent refraction in the strabismic eye was significantly more hyperopic in patients who underwent three or more surgeries (0.79 ± 0.37 D), compared with those with one (−0.95 ± 0.094 D; p < 0.001) or two surgeries (−0.36 ± 0.16 D; p < 0.001). Relative to one surgery, undergoing two surgeries was independently associated with larger distance horizontal deviation (adjusted odds ratio (aOR) per prism diopter = 1.012; 95% CI, 1.003–1.022; p = 0.009). Undergoing three or more surgeries was independently associated with amblyopia severity (aOR = 2.368; 95% CI, 1.279–4.384; p = 0.006); in the strabismic eye, and higher spherical power markedly increased the odds (aOR = 13.553; 95% CI, 12.801–14.348; p < .001).
Conclusion:
Worse preoperative BCVA, greater hyperopia, and higher angle of deviation were associated with a greater likelihood of requiring more than one surgery. Surgeons should optimize preoperative refractive and amblyopia management and counsel high-risk patients about the increased likelihood of additional procedures.
Introduction
Childhood unilateral exotropia might be constant when it manifests in one eye all the time or intermittent when it manifests when the child is tired, ill, not focusing, or at the end of the day. 1 Intermittent exotropia (IXT) has been recognized as the most common form of childhood-onset exotropia, and it affects approximately 1% of the population.2–4 Burian classified IXT into four forms based on the difference in magnitude between the distance and the near: basic, convergence insufficiency, true divergence excess, and pseudo divergence excess. 5 Previous studies have reported varying results regarding the natural course of IXT during childhood, with no change over 3 years 6 or a higher percentage of improvement than deterioration over 3 years 7 to equal chance of deterioration or improvement over 5 years. 8 Therefore, management of intermittent exotropia requires careful investigation. Several methods have been suggested in the treatment of IXT; however, there is no evidence-based consensus regarding the best treatment time and the most effective method. 9 The common methods include refractive error correction, minus overcorrection, occlusion therapy, base-in prism prescription, vision therapy, and surgery. Surgical intervention is considered when IXT could not be controlled with the nonsurgical methods of treatment, or there is a large angle of deviation, and control of deviation has gotten worse over time, such that it manifests > 50% of awake time at home, or it is observed instantly or by fusion disruption without recovery.10–12 However, strabismus surgery is not always successful in fully eliminating the ocular misalignment, with reported reoperation rates ranging from 4.2% to 60%.13,14 One possible factor in needing multiple surgeries for ocular alignment was defined as deviations ⩾35 prism diopters (PD). 15,16 However, there also might be other possible risk factors to contribute to the need for reoperation, such as younger age at surgery and lack of binocular fusion. 17 Choice of surgical technique may also play a role. The techniques, such as bilateral lateral rectus muscle recession versus unilateral lateral rectus muscle recession combined with medial rectus muscle resection (R& R), might be used.18,19 A smaller amount of preoperative deviation and the presence of refractive errors, especially a shift toward myopia, and the amount of surgery were significant factors in a favorable outcome in patients who underwent surgery for exotropia. 20 On the other hand, a larger angle of deviation and more hyperopia were in association with a low success rate in patients with IXT.21,22 Consistently, initial overcorrection of less than 10 PD toward esotropia was a possible success rate in less recurrence of exotropia within 2 weeks and after 2 years of surgery in IXT.23,24 Although amblyopia rarely occurs in patients with IXT, in cases with constant unilateral exotropia is a definite concern and it might influence the surgery outcome; however, the presence of amblyopia as a contributing factor has not been investigated in the literature. The present study, with a decent sample size, compares the preoperative refractive status, visual acuity, angle of deviation, and amblyopia type and severity in patients with basic unilateral exotropia, either intermittent or constant, who underwent single versus two and three or more strabismus surgeries. Identifying clinical features associated with surgical success may help reduce the need for reoperation.
Methods
Study design
This retrospective cross-sectional study was conducted at the Farabi Eye Hospital, Tehran University of Medical Sciences, Tehran, Iran. The study protocol was approved by the Institutional Review Board (IR.TUMS.FNM.REC.1402.031) and adhered to the tenets of the Declaration of Helsinki.
Participants
The medical records of all patients with unilateral exotropia who underwent strabismus surgery between January 2010 and January 2020 were reviewed.
Patients were included in the study if they exhibited either intermittent or constant exotropia, with one eye being dominant for fixation, as evaluated through the unilateral cover test. The patients selected for inclusion had undergone multiple follow-ups, and due to a decline in the control of exotropia, they were referred for surgical intervention. The criteria for surgery were based on documented serial deterioration in exotropia control, which was assessed using both home and office control scales. 20 For example, if exotropia was present at least 50% of the time, or if there was any observed increase in the magnitude of deviation after several follow-ups, or if a progressive inability to control the exotropia was noted during the manifest phase of deviation, these were considered indicators of poor control. 20 In the constant exotropia, cohorts older than 3 years old, surgical intervention was conducted only if there was no improvement after nonsurgical treatments and the deviation remained unchanged in two consecutive follow-ups; whereas in cases younger than 3 years of age, surgery was performed if they exhibited a deviation magnitude of ⩾40 PD in two consecutive follow-ups. Patients were divided into three groups based on the number of strabismus surgeries performed: single surgery, double surgeries, and triple or more surgeries. Patients with restrictive or paralytic strabismus, vertical or torsional strabismus, prior strabismus or refractive surgery, coexisting ocular pathology, or systemic disorders affecting ocular motility were excluded.
Measurements
Preoperative data extracted from patient records included age, gender, best corrected distance visual acuity (BCVA) in each eye, refractive error, and angle of strabismus deviation at near and far. Visual acuity was tested at distance using the Snellen E chart, and the results were converted to logMAR using this formula: VA logMAR = −log (VAE-Snellen decimal). The conversion was conducted to provide a standardized measurement of visual acuity and make the comparison to the studies possible. Visual acuity was not assessed for children under 4 years old, given the challenges of measuring acuity accurately and interpreting norms in that age group. Refractive error was measured using an autorefractor (Topcon KR-8900 and KR-800, Topcon Corporation, Tokyo, Japan), and the results were confirmed by the Heine beta 200 retinoscope (Heine Optotechnik, Herrsching, Germany). Cycloplegic refraction was conducted using the Tropicamide 1% eye drop instilled two times in 5-min intervals, and patients were tested after 15–20 min. The best corrected subjective refraction results were recorded as sphere, cylinder, and spherical equivalent (SE) power in diopter (D).
The angle of deviation was measured using the alternate prism-cover test at distance and near, and the results were recorded in PD. At a distance, patients fixated on the letters on the visual acuity chart one line bigger than their BCVA. At 33 cm, patients fixated on a small, detailed accommodative target while performing the cover test. 25 If the patient, particularly young children or those with limited cooperation, was unable to undergo the alternate prism-cover test, the Krimsky method was used. The Krimsky method involves placing prisms in front of the non-strabismic eye and adjusting the prism power until the cornel light reflex is centered on both eyes. Basic exotropia was defined as the difference between near and far deviation being ⩽ 10 PD. 5 In cases with divergence excess, the patch test was conducted for 30 min to differentiate the true divergence excess from simulated divergence excess.
Unilateral amblyopia was defined as an interocular difference of ⩾2 Snellen (decimal) lines in BCVA and BCVA ⩾ 0.1 logMAR in the amblyopic eye (8/10 decimal) with the presence of at least one of the following amblyogenic factors: (1) anisometropia (difference in myopia, hyperopia, and astigmatism equal or more than 3.00 D, 1.00 D and 1.50 D, respectively), (2) strabismus, and (3) combined anisometropia and strabismus. 26 Amblyopic patients were divided into three severities: mild (BCVA in the amblyopic eye 0.1 logMAR), moderate (BCVA in the amblyopic eye 0.2–0.7 logMAR), and severe (0.8 logMAR or worse).27,28
The most common surgery techniques performed included unilateral recession–resection (R & R), unilateral lateral rectus recession (LR rec), and bilateral lateral rectus recessions (BLR rec). Patients were followed for a minimum of three years post-surgery.
Statistical analysis
Data were analyzed using SPSS Statistics for Windows, version 24.0 (IBM Corp., Armonk, NY, USA). The Shapiro–Wilk test was used to assess the normality of data distribution. Descriptive statistics, including mean and standard deviation, were calculated. One-way analysis of variance was used to compare the single, double, and triple surgery groups. A p-value less than .05 was considered statistically significant. Independent predictors of reoperation were evaluated using multinomial logistic regression (reference = one surgery) with prespecified predictors: age at first surgery, distance horizontal deviation (far primary position), BCVA in the strabismic eye, refractive components (sphere, cylinder, SE), and amblyopia severity status. Model fit was assessed by likelihood ratio tests and pseudo R². Results are reported as adjusted odds ratios (aORs) with 95% CIs.
Results
The study population consisted of 2457 patients with unilateral basic exotropia, including 1125 (45.8%) females and 1332 (54.2%) males (p < 0.001). The mean age at first surgery was 26.3 ± 13.35 years (range: 2–77 years). Of those, 1886 (76.8%) underwent single surgery, 411 (16.7%) underwent two surgeries, and 160 (6.5%) had three or more surgeries.
In the one-surgery group (n = 1886), the most common procedures were recession–resection (R&R; 50.8%), unilateral LR rec (25.9%), and BLR rec (8.9%). In the two-surgery group (n = 411), R&R (40.6%), LR rec (22.9%), and BLR rec (10.0%) were most frequent. In the three-or-more-surgeries group (n = 160), R&R (41.3%), LR rec (30.0%), and BLR rec (7.5%) predominated.
Tables 1 and 2 show the age, visual, refractive, and deviation characteristics of the different groups of patients with unilateral exotropia based on the number of surgeries. Because our wide age range (2–77 years) may have masked any influence of age, we classified patients into six age groups (Figure 1). As the bar chart illustrates, most patients underwent their first surgery between 19 and 40 years of age.
Age, BCVA, and refraction (sphere, cylinder, and SE) in the strabismic and non-strabismic eyes in patients with unilateral basic exotropia.

BCVA less than 20/400 was considered as follows: finger count: 2.0 logMAR; hand motion: 2.3 logMAR; light perception: 2.6 logMAR; and no light perception (NLP) = 2.9 logMAR.
BCVA, best corrected distance visual acuity; SE, spherical equivalent.
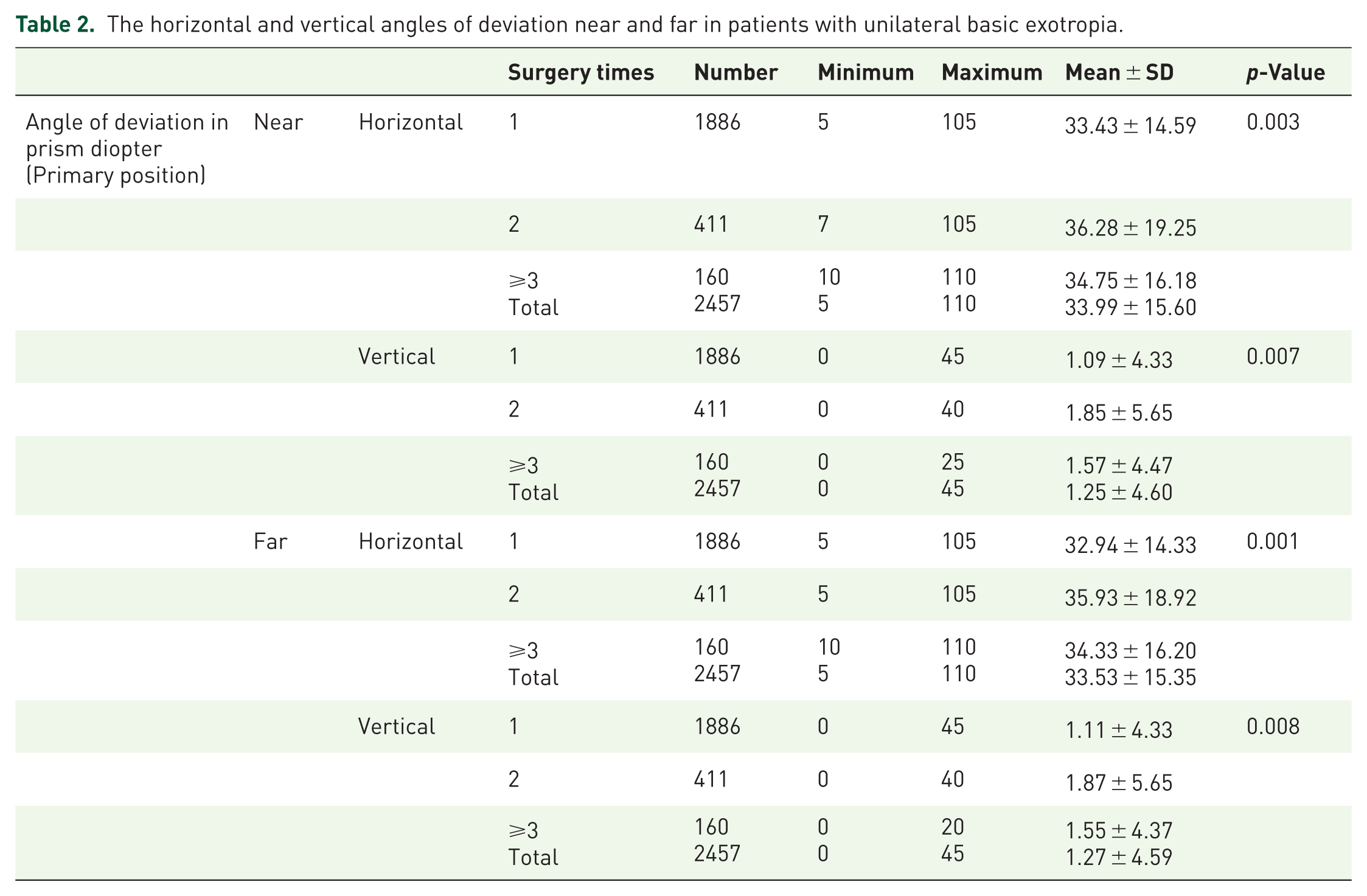
The horizontal and vertical angles of deviation near and far in patients with unilateral basic exotropia.

Distribution of times of surgeries in each age group.
Mean BCVA in the strabismic eye was significantly worse in patients who underwent three or more surgeries (0.82 ± 0.076 logMAR), compared with those who underwent one (0.55 ± 0.018 logMAR) or two surgeries (0.52 ± 0.038 logMAR) (p < 0.001). Post hoc analysis using the least significant difference test showed a significant difference between the one-surgery and three-or-more-surgery groups and between the two-surgery and three-or-more-surgery groups (p < 0.001 for both). There was a significant association between amblyopia severity and number of surgeries (χ2 [4] = 15.683, p = 0.003; Figure 2) and between amblyopia type and number of surgeries (χ2 [4] = 30.758, p < 0.001; Figure 3).

Distribution of times of surgeries in different amblyopia severities.
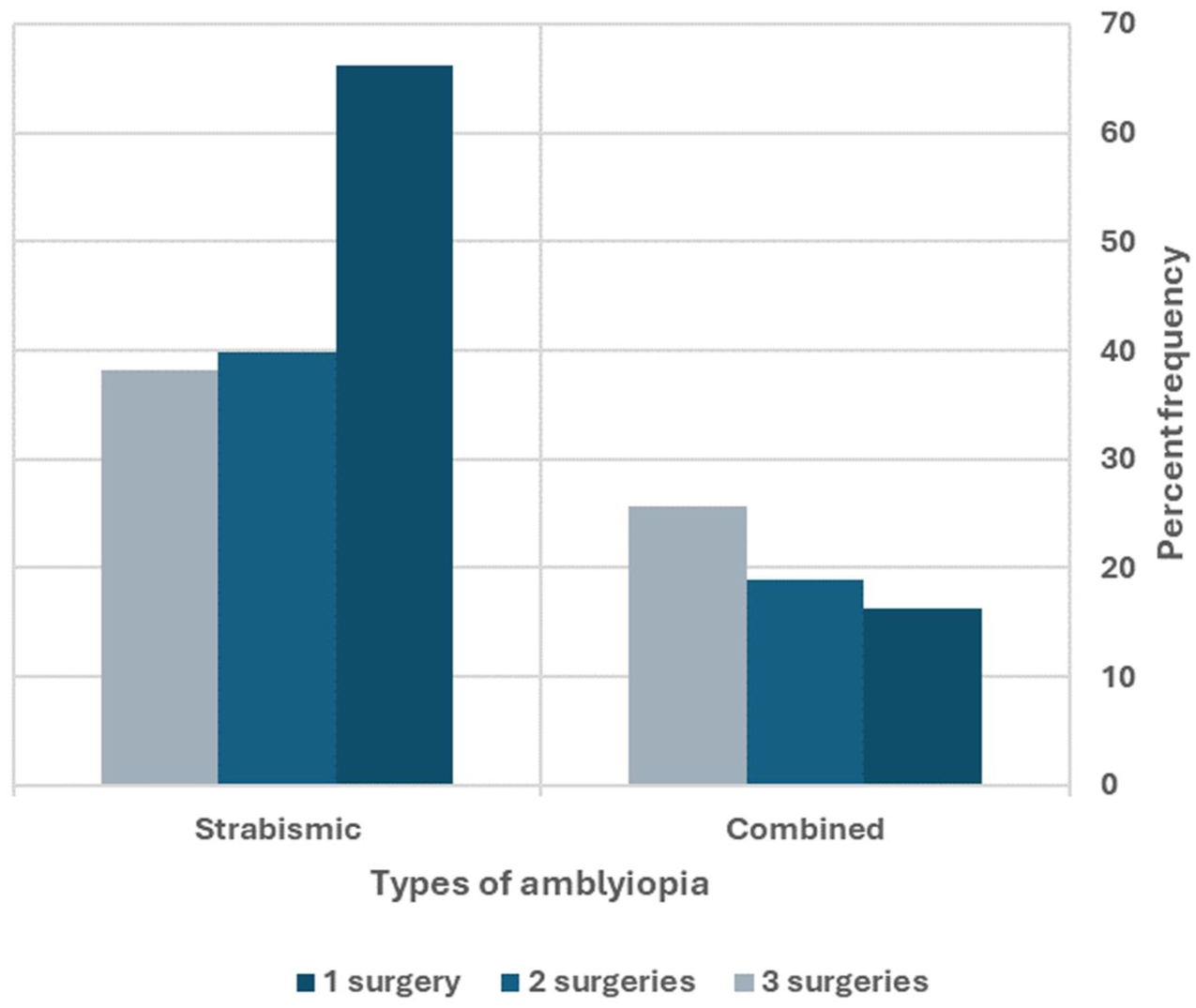
Distribution of times of surgeries in each amblyopia type.
Analysis of refractive errors in the strabismic eye showed a significant difference in spherical component and SE between groups (p < .001 for both). Post hoc analysis revealed a significant difference between all three groups for both spherical component and SE (p < 0.05 for all), with a mean SE of −0.95 ± 0.094 D, −0.36 ± 0.16 D, and 0.79 ± 0.37 D in the one-surgery, two-surgery, and three or more surgeries, respectively (Table 1).
Analysis of the magnitude of horizontal deviation at distance showed a significant difference between groups (p = .001). However, post hoc analysis showed a significant difference only between the one-surgery and two-surgery groups (p < .001; Table 2).
In the multinomial logistic regression, the model significantly improved fit over the intercept-only model (likelihood ratio χ2 = 89.0, df = 22, p < 0.001; Nagelkerke R 2 = 0.077). Relative to one surgery, greater horizontal distance deviation was independently associated with undergoing two surgeries (aOR per prism diopter = 1.012; 95% CI, 1.003–1.022; p = 0.009). In the strabismic eye, higher spherical power was positively associated (aOR = 13.553; 95% CI, 12.801–14.348; p < 0.001) with ⩾3 surgeries. For the ⩾3-surgeries category, amblyopia severity was independently associated with higher odds of multiple reoperations (aOR = 2.368; 95% CI, 1.279–4.384; p = 0.006). Age and distance horizontal deviation were not significant predictors for the ⩾3-surgeries category after adjustment.
Discussion
This study compared the clinical characteristics of patients with unilateral basic exotropia who underwent one strabismus surgery with those who required two or three or more surgeries. Patients with worse BCVA, severe amblyopia, and more hyperopia in the strabismic eye were more likely to require more than one surgery; whereas, the magnitude of deviation was only effective in requiring two surgeries, and it was not different between groups with two and three, or more surgeries. Lastly, age at first surgery did not differ between groups.
The overall reoperation rate in our study was 23.2%, with 16.7% of patients requiring two surgeries and 6.5% requiring three or more surgeries. Studies have reported reoperation rates of 14%–42% after the primary surgical correction of IXT.29–31 These variable rates may be due to differences in patient selection, length of follow-up, and other factors. In a large retrospective study, Repka et al. investigated strabismus surgery and reoperation rate in 846,477 American children with strabismus. 32 They found that 0.13% of patients underwent strabismus surgery and that the reoperation rate, 1 year after the first surgery, was 6.72%. This rate was 3.95% for patients 6–9 years of age and increased significantly to approximately 11.5% for patients older than 65 years (p < 0.001). Repka et al. included both types of horizontal strabismus in their study without specifying the subtypes; whereas we focused only on patients with basic exotropia, of whom 23.2% required more than one surgery during a 10-year follow-up period. In another retrospective population-based study, Leffler et al. reviewed the reoperation rate and predictors of reoperation in 11,115 patients with strabismus (under 18 years old). 33 They found that 7.7% of participants (n = 851) underwent reoperation. Moreover, the reoperation rate was higher in patients under the age of 2 years old, using the adjustable sutures or botulinum toxin injection. Similar to Repka et al., Leffler et al. reported the reoperation rate and contributing factors in various types of strabismus. Our study focused on exotropia and specifically basic exotropia and included a large sample size, providing valuable clinical data in this group of patients who underwent surgery.
Our study found that greater hyperopia was associated with a higher reoperation rate. Zhou et al evaluated the success rate in 82 patients with IXT (age range 3.7–81.6 years) and reported that greater hyperopic refractive error (mean SE) and larger angle of deviation were associated with a lower success rate of unilateral intermittent exotropia surgery. 21 This is in line with our findings, with a higher probability of reoperation in hyperopic patients and a larger angle of deviation in patients who required more than one surgery. Worse BCVA in the strabismic eye was associated with a higher reoperation rate, which was expected because the presence of more severe amblyopia likely affects postoperative ocular alignment.
The surgery techniques used in all three groups were the same. The most common technique was R&R, followed by LR rec and BLR rec. Therefore, the choice of surgery was not a contributing factor for requiring more than one surgery. However, preoperative angle of deviation and amount of surgery, including less immediate postoperative overcorrection, are determining factors for recurrence.20,21,34
Age at surgery was not a contributing factor in the reoperation rate in our study. Consistently, Zhou et al. did not report the influence of age at surgery on the reoperation rate. Similar to our study, a wide age range was included (3.7–81.6 years old) in Zhou et al.’s study. 21 This might have masked any influence of age at surgery. In contrast, Lim and colleagues showed a less reoperation rate when patients underwent surgery at an older age; where they recruited 511 children between 3 and 10 years with intermittent exotropia. 35
In our study, most patients underwent their first surgery between 19 and 40 years of age, and this group also had a higher reoperation rate than the other age groups. Heo et al. reported that younger children (0–3 years old) had a higher reoperation rate than older children (4–6 and 7–12 years old) over a period of 5 years. 36 In another study that systemically evaluated the risk of reoperation in the pediatric population under 9 years old with strabismus, 843 per 10,000 patients with exotropia underwent reoperation. Logistic regression analysis showed that the risk of reoperation was higher when strabismus surgery was conducted at a younger age (<3 years old) and when only one eye was operated than two. 37 Interestingly, Repka et al. evaluated surgery outcomes in children between 3 and <11 years with basic type IXT and reported that younger age at surgery (3 to younger than 5 years vs 5 to younger than 11 years) was associated with better surgical results in these patients. 38 Generally, evidence suggests that an age younger than 3 years is a risk factor for reoperation. However, we did not include children younger than 2 years, and our study population had a wider age range (2–77 years), which may not be directly comparable to the current literature.
The main limitations of this study were its retrospective design and inclusion of patients from a single center. In addition, postoperative data were not collected, which would have allowed us to identify factors associated with surgical success in patients with exotropia. The other limitation was that we did not differentiate between intermittent and constant exotropia. Future prospective multicenter studies are needed to confirm our findings, identify visual and refractive patterns in different types of strabismus, and evaluate postoperative outcomes.
Conclusion
This study supports practical adjustments to surgical planning and counseling. First, worse preoperative BCVA, greater hyperopia, and a larger preoperative deviation are associated with a higher risk of recurrence. Second, prioritize meticulous preoperative refractive management and aggressive amblyopia therapy when feasible to optimize sensory status. Third, counsel patients and families that hyperopia and poorer BCVA increase the likelihood of additional surgery, with clear discussion of alignment targets and early postoperative expectations. Integrating these risk-informed strategies may reduce reoperation rates and improve long-term alignment stability.