
Abstract
Charles Bonnet syndrome (CBS) is characterised by visual hallucinations in individuals with significant visual impairment. This literature review and case report focus on the unique presentation of CBS in an 82-year-old woman with age-related macular degeneration, who experienced visual hallucinations for over 10 years. The aim is to raise awareness of CBS among healthcare professionals and the public, addressing the diagnostic challenges that contribute to its underdiagnosis and mismanagement. A literature review was conducted to assess the prevalence and diagnosis of CBS. Databases including Google Scholar and PubMed were searched using the terms ‘Charles Bonnet Syndrome’, ‘Case report’ and ‘Diagnosis’. The patient reported a range of visual hallucinations, from simple geometric shapes to highly detailed figures. A diagnosis of CBS was made based on her visual impairment and the nature of the hallucinations. No treatment was required, and the patient was reassured that the hallucinations were benign and unrelated to any psychiatric or neurological disorder. This case highlights the diagnostic challenges associated with CBS, which is often misdiagnosed or overlooked due to its rarity and the hesitancy of patients to disclose their symptoms. The long period of unreported hallucinations in this case emphasises the need for greater awareness among healthcare providers, enabling earlier recognition of CBS and differentiation from other conditions. The wide range of hallucination types seen in CBS adds to the complexity of the syndrome. The key takeaway is that increased awareness and recognition of CBS are essential for proper diagnosis, reducing patient anxiety and avoiding unnecessary treatments. This case contributes to the existing literature by illustrating the broad spectrum of CBS presentations and advocating for enhanced education on the condition.
Plain language summary
Charles Bonnet Syndrome (CBS) causes visual hallucinations in people with vision loss. This summary discusses an 82-year-old woman with age-related macular degeneration who experienced CBS for over 10 years. The aim is to raise awareness among healthcare providers and the public, as CBS is often misdiagnosed or missed. A review of the literature was conducted. The patient’s hallucinations ranged from simple patterns to detailed images. She was diagnosed with CBS based on her vision problems and hallucinations. No treatment was needed, and she was reassured that the hallucinations were not related to any psychiatric or neurological conditions. This case shows how CBS can be overlooked because patients may not report their symptoms, and the condition is not well-known. It highlights the need for better awareness to help healthcare professionals recognize CBS and avoid unnecessary treatments. Increased understanding of the varied nature of CBS hallucinations is important for reducing patient distress and improving diagnosis.
Introduction
Charles Bonnet syndrome (CBS) is a condition that is characterised by simple or complex hallucinations in those with visual impairments 1 particularly those suffering from conditions like macular degeneration or glaucoma. 2 The primary theory suggests that these hallucinations may be manifestations of release phenomena resulting from the deafferentation of the visual association areas of the cerebral cortex, leading to a phenomenon akin to phantom vision.3,4
This disease was first recognised in 1760 by Charles Bonnet through his visually impaired grandfather Charles Lulin and later named by George de Morsier. 5 However, despite its historical recognition, CBS remains relatively underdiagnosed due to various factors. 6 One key reason for this is patients’ reluctance to report hallucinations for fear of being stigmatised or misdiagnosed with a psychiatric disorder. 7 Recent research has suggested that the prevalence of CBS is higher in women,8,9 as well as other factors such as isolation of individuals. 9 Over the past 13 years, there has been a significant surge in the number of publications about this condition, attributed to the forthcoming inclusion of CBS in the World Health Organization’s International Classification of Diseases. 10
At present, there is no standardised treatment for this disorder. 11 Furthermore, most funded research is only being conducted in the United Kingdom through charities such as ‘Esmes Umbrella’ and ‘fight for sight’. 8 Despite this, several approaches have been explored to help manage symptoms. Some of these include reassurance, education about the condition, cognitive-behavioural therapy and in some cases medications such as antipsychotics. 12
Individuals with CBS can experience a broad spectrum of visual hallucinations, ranging from simple to complex. 1 Simple hallucinations often manifest as basic geometric patterns or coloured shapes, while complex hallucinations involve more detailed and recognisable forms such as faces, figures or common objects. The common characteristics that have been identified include tessellopsia (the perception of regular overlapping patterns), prosopometamorphopsia (facial distortion), dendropsia (branching forms), hyperchromatopsia (enhanced perception of vivid colours), polyopia (multiple images of a single form) and size distortions such as micropsia and macropsia, where objects appear smaller or larger than their actual size. 12 Despite the diversity of hallucinations within the individuals who experience CBS, these common features help clinicians to recognise and diagnose the syndrome.
The objective of this review is to define and characterise the main symptoms and prevalence of CBS. Furthermore, an individual case report was addressed from one of The Retina Clinic London’s patients to highlight the symptoms and management of CBS. This highlights a key clinical implication: timely and accurate identification of CBS symptoms is essential, not only to prevent unnecessary diagnostic procedures but also to provide reassurance and improve patient outcomes. This case report has been formatted using the CARE checklist.
Case report
An 82-year-old Caucasian woman, a patient at the Retina Clinic London for over five years presented with visual hallucinations to us on the 19 March 2024. The patient reported a history of visual hallucinations dating back at least a decade but had not previously discussed them during consultations. A few years prior to this visit, she had mentioned these hallucinations to her local optician. At this stage, she was reassured by the optician, who explained that such hallucinations can occur in individuals with visual impairments like herself as shown in Figures 1 and 2. It has been suggested that pre-warning about symptoms of CBS is a useful tool in the management of this diagnosis. 10
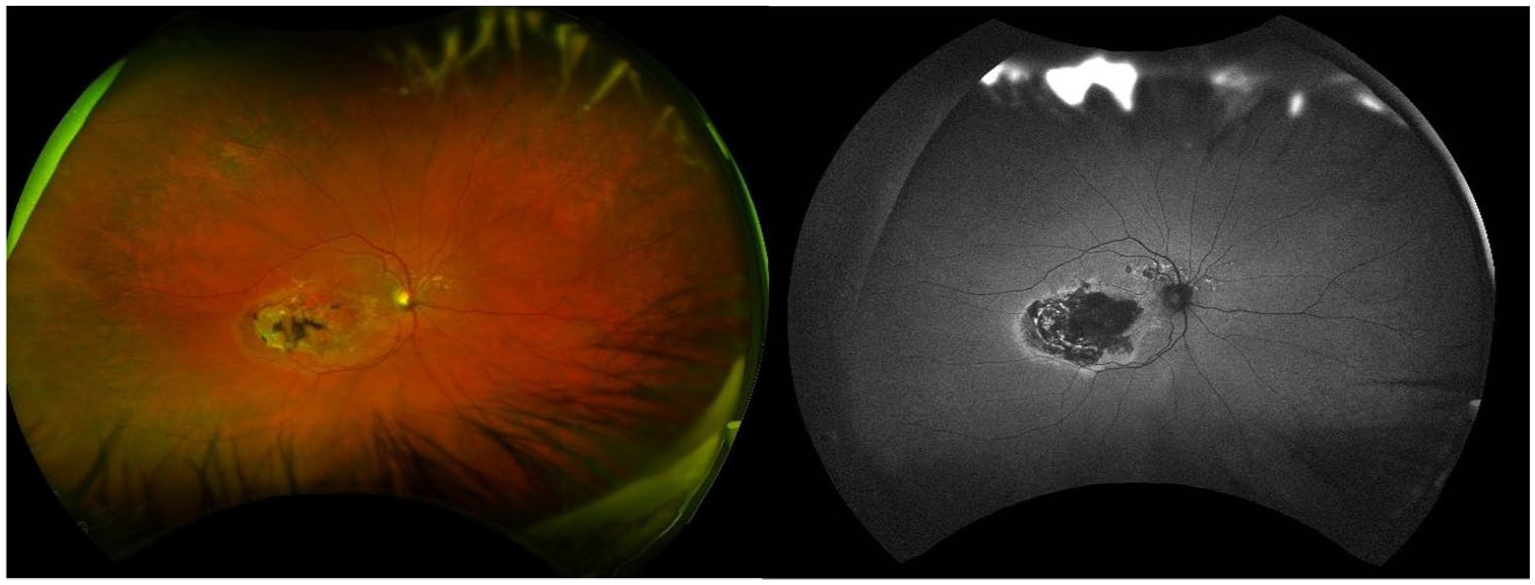
Optos Silverstone (Optos PLCDunfermline, Scotland, UK) Ultra-widefield Colour fundus and Autofluorescence images of patient’s Right eye indicating Late-stage Age-related Macular Degeneration (AMD) in the form of Geographic Atrophy.

Optos Silverstone (Optos PLC, Dunfermline, Scotland, UK) Ultra-widefield Colour fundus and Autofluorescence images of patient’s Left eye indicating late-stage AMD in the form of Geographic Atrophy.
The patient has been enrolled in a phase III clinical trial investigating the effects of an intravitreal injection known as Pegcetacoplan on geographic atrophy secondary to age-related macular degeneration. Throughout this trial, her left eye was designated as the study eye. Her visual acuity remained stable in both eyes throughout this ongoing study period (See Table 1), and symptoms of CBS remained consistent.
Best Corrected Visual Acuity (BCVA) of patient over last 2 years, expressed as standardised Early Treatment Diabetic Retinopathy Study letter score.

CBS diagnosis was done following the World Health Organization 2018 revision of the International Classification of Diseases. 13 Given the patient’s stable vision and lack of any known psychological or mental illnesses, her visual hallucinations were consistent with the characteristics of CBS.
The patient’s medical history includes primary total knee replacement, Geographic Atrophy in her left eye and wet AMD in her right eye (Figures 1 and 2), diverticular disease, laparoscopic cholecystectomy, hypertension, post-operative chest infection and migraines- although not correlated to her hallucinations. She has no known drug allergies. Vitals and laboratories were within normal limits. Her consumption of alcohol and tobacco was minimal throughout experiencing these hallucinations.
The patient first experienced these hallucinations over a decade ago, and they perfectly illustrate the diverse and complex nature of visual hallucinations in CBS. Five distinct hallucinations have been reported by the patient and have been persistent over the last couple of years. The first hallucination that our patient experienced was that of a woman facing her, with a cigarette in the corner of her mouth. The next common hallucination that she experienced came about after she started receiving intravitreal anti-VEGF injections. She saw an eye surrounded by a blue ring, typically in the opposite eye to which she had injected. Another frequent hallucination reported involved seeing the backs of three elderly ladies, whom the patient’s daughter connected to three ladies who attended their church. The figures are described as wearing brown jackets and skirts, with their clothing appearing muffled and in an assortment of colours. The fourth hallucination our patient perceives occurs while watching television, where the patient sees an old barn door adjacent to the screen. The most recent hallucination experienced by our patient involves seeing butterfly wings flapping up and down, with reddish-black colours. The patient reported that this hallucination occurs at least once daily.
Discussion
CBS is a clinical condition with a reported estimated prevalence of 20% in the low-vision population. 13 Niaz et al., conducted a review of over 4303 AMD patients identifying CBS symptoms in 15.8% of individuals. Despite the often vivid and varied nature of these hallucinations, the patient in this case reported that none were distressing or perceived as threatening. Over time she has become accustomed to them, which may be attributed to early reassurance provided by her optometrist when her concerns were initially raised. This finding is consistent with a broader survey, wherein over 70% of participants with AMD reported a neutral emotional response to their hallucinations.10,14 In Contrast, a separate case report involving a 69-year-old male patient described hallucinations of people attacking him, which elicited significant paranoia and distress. 12 These findings underscore the diverse psychological impacts of CBS across different individuals.
The link between CBS and AMD is well-established, with AMD frequently cited as the most common underlying cause of CBS-related visual impairment. 15 Our patient exemplifies this connection, presenting with a history of AMD and hallucinations limited to the visual domain, with no other sensory modalities affected. This intact insight into the unreal nature of hallucinations aligns with diagnostic criteria for CBS and underscores the importance of differentiating CBS from neuropsychiatric conditions.
A notable feature of this case is the patient’s prolonged but neutral response to hallucinations. However, the impact of hallucinations experienced by people suffering from CBS can vary entirely. Cox et al., 16 analysed this using a large-scale questionnaire. This involved a total of 1254 responses from individuals who indicated a diagnosis of macular disease. Among them, 39% reported experiencing hallucinations, including patterns (63%), faces (39%), figures (39%) and animals (22%) and either had been informed or self-diagnosed with CBS. At the onset of CBS, 38% reported fear-inducing reactions, which decreased to 8% by the time of this survey. In addition, 46% stated that CBS affected their daily activities. Merely 7% had refrained from disclosing CBS symptoms to anyone, while 47% had discussed their experiences exclusively with a medical professional. 16
In a separate investigation, a cohort of 2565 individuals aged 40 and above was analysed to assess the prevalence and characteristics of hallucinations in individuals with visual impairment. Findings revealed that 18.8% of the participants had encountered hallucinations. Notably, the likelihood of hallucinations increased with greater levels of vision loss, suggesting a direct correlation between the severity of visual impairment and the occurrence of hallucinations. 7 However, the frequency of hallucinations remained consistent across patients with various visual conditions such as glaucoma, diabetic retinopathy or age-related macular degeneration. 7 This suggests that while the extent of vision loss plays a role in the occurrence of hallucinations, the specific type of visual impairment may not be a determining factor in their frequency. However, a study by Christoph et al. demonstrated that among patients with CBS, AMD was the most common underlying cause of visual impairment. 15
A similar case to that of ours featured an 80-year-old woman who presented to an emergency room with hallucinations of organisms in her food and stool. This patient akin to our patient, fits all the criteria of CBS, including visual impairment, persistent visual hallucinations and intact insight into the unreal nature of the hallucinations. Notably, her hallucinations were limited to the visual sense, with no other sensory modalities affected. 17
Furthermore, an extensive survey was administered to individuals with late macular degeneration, mirroring our patient’s condition, to investigate potential links with visual hallucinations. 14 The findings revealed that 27% of participants were encountering such visual manifestations, with the sole correlation being poor visual acuity. The predominant hallucination reported was that of seeing people, aligning with the primary hallucination experienced by our patient.
Despite the absence of standardised treatment for CBS, 18 olanzapine and mirtazapine, have been documented in the literature.3,12,19 In a specific study, the patient’s treatment protocol began with an initial dose of 2.5 mg, which was subsequently increased to 5 mg administered once daily. The patient reported a gradual reduction in hallucinations, eventually experiencing minimal to no hallucinations. 12 Similarly, another case involved a female patient with CBS who received 5 mg of olanzapine. 19 After two weeks of treatment, while hallucinations persisted, the patient demonstrated an awareness of their unreality and no longer responded to them.
Other medications have been used to try and treat CBS, including valpromide, risperidone, carbamazepine, melperone, valproate, cisapride and ondansetron 3 ; however, they were not required in this case. Treatment options should be considered only if patients are unable to cope with visual hallucinations. In our case, early diagnosis contributed to the patient remaining neutral toward the hallucinations, negating the need for further intervention.
Early diagnosis of CBS is essential to mitigate the negative effects of visual hallucinations. In 2018, the World Health Organization (WHO) established a distinct diagnostic code for CBS, emphasising the need to rule out other potential causes. According to the WHO criteria, CBS is characterised by the occurrence of intricate visual hallucinations, partial or complex vision impairment and the absence of mental or behavioural disorders. 13 Therefore, increasing awareness of CBS remains critical. A specific study revealed that 55% of Canadian family physicians lacked awareness of CBS, with approximately 85% never broaching the topic with patients experiencing poor vision. 10 Moreover, among patients exhibiting CBS symptoms and seeking medical guidance, more than a third perceived that the healthcare provider was uncertain or lacked full awareness of CBS.
In our case, early reassurance by the optometrist likely contributed to the patient’s positive adaptation to her symptoms. However, this level of reassurance is not consistently observed among other individuals with CBS. Patients who are unfamiliar with the condition frequently attribute their symptoms to other factors, such as a perceived decline in cognitive abilities or a psychiatric disorder. For instance, a third of patients express fear of impending insanity due to their hallucinations, while 63% are apprehensive about being perceived as ‘insane’ if they were to disclose their hallucinations. 6
Although a broader association between the severity of visual impairment and CBS hallucinations has been reported in large-scale studies, 7 this relationship is not directly applicable to our case, as the focus here is on the emotional and clinical response to CBS rather than the underlying visual impairment. Similarly, while physician awareness of CBS remains a critical issue,6,10 our patient’s case highlights the positive impact of informed care provided early in the diagnostic process.
Conclusion
In conclusion, CBS presents a fascinating interplay between visual impairment and the brain’s response, resulting in hallucinations that can be both simple and complex. Despite its historical recognition, CBS remains underdiagnosed, primarily due to patient reluctance to report symptoms and healthcare provider awareness gaps. However, recent efforts, including increased research and forthcoming inclusion in international disease classifications, signal a growing understanding of the syndrome.
The impact of CBS hallucinations spans from neutral to distressing experiences, emphasising the urgency of timely recognition and appropriate management. While standardised treatment protocols are lacking, various strategies, such as reassurance, education, cognitive-behavioural therapy and pharmacotherapy, offer hope in alleviating symptoms and enhancing patients’ quality of life.
Diagnostic challenges persist, with many healthcare providers and patients unaware of CBS or mistaking its symptoms for other conditions. Increased awareness among healthcare professionals and the public is essential to facilitate early diagnosis and alleviate patient concerns about stigma or misinterpretation of their experiences.
The case study presented here underscores the complex nature of CBS and highlights the need for comprehensive assessment and tailored management strategies to address the diverse needs of affected individuals. Without adequate awareness of CBS, patients like ours may have distressing hallucinations, significantly impacting their mental well-being.
As research continues to unravel the intricacies of CBS, efforts to enhance awareness, promote accurate diagnosis and develop effective interventions are paramount to improving outcomes and supporting individuals living with this unique syndrome.