
Abstract
Background:
Cardiac surgery has been associated with adverse ocular events. Off-pump coronary artery bypass graft surgery evades the systemic inflammatory response seen in extracorporeal circulation and is superior to on-pump surgery with regard to end-organ dysfunction and neurological outcomes.
Objectives:
To determine the effects of off-pump (without extracorporeal circulation) coronary artery bypass graft surgery on choroidal thickness, ganglion cell complex, and the retinal nerve fiber layer.
Design:
Prospective, longitudinal study.
Methods:
Patients who underwent off-pump surgery were examined preoperatively and postoperatively at 1 week and 6 weeks after surgery. Choroidal thickness, ganglion cell complex, and the retinal nerve fiber layer measurements were recorded, and the effects of off-pump coronary artery bypass on these parameters were assessed.
Results:
A total of 44 eyes of 44 patients were included in the study. There was a statistically significant increase in subfoveal choroidal thickness from 252.84 ± 56.24 µm preoperatively to 273.82 ± 39.76 µm at 1 week and 301.97 ± 44.83 µm at 6 weeks after off-pump coronary artery bypass graft surgery (p = 0.044; p ⩽ 0.001). Ganglion cell complex and retinal nerve fiber measurements showed no significant difference compared to preoperative values.
Conclusion:
Off-pump coronary artery bypass graft surgery showed no negative effects on ganglion cell complex and retinal nerve fiber measurements. A significant increase in subfoveal choroidal thickness was seen after off-pump surgery, which might be advantageous in patients who are at high risk or have preexisting ocular diseases that are affected by the choroid.
Keywords
Introduction
Visual loss after non-ophthalmic surgery is a rare, disastrous complication that is most frequently encountered after cardiac surgery. 1 Ischemic optic neuropathy and retinal artery occlusion due to emboli and/or low perfusion pressure due to hemodynamic instability can result in hypoperfusion of the optic nerve, retina, and choroid with serious consequences. Coronary artery bypass graft (CABG) surgery is the most widely performed cardiac surgery worldwide, and the place of on-pump, using extracorporeal circulation (ECC), and off-pump coronary artery bypass graft (OPCAB) surgery is still widely debated.2,3 Most authors agree that a patient-based approach should be used to determine which patients would be most likely to benefit from each procedure: high-risk patients, patients with a history of cerebral stroke, vascular disease, kidney failure, and liver disease are some of the patients in which OPCAB has been deemed advantageous.4,5
Hemodynamic changes and the systemic inflammatory response after on-pump surgery have been postulated to cause changes in retinal and choroidal circulation.6,7 Purtscher-like retinopathy is a prominent example of the effect of on-pump CABG-related inflammatory response on the retina. 8 Studies examining the retinal nerve fiber layer and choroidal thickness after on-pump coronary artery bypass graft surgery have shown no deleterious effects on short-term follow-up.6,7,9 OPCAB is believed to decrease end-organ dysfunction by protecting against the adverse effects of ECC seen in on-pump patients. 4 Neurological outcomes in patients treated with OPCAB have also been found to be superior to on-pump coronary bypass 10 ; changes in retinal nerve fiber layer (RNFL) and ganglion cell complex (GCC) have been associated with neurological diseases such as Alzheimer, multiple sclerosis, and Parkinson’s disease11–13; and the assessment of these layers after OPCAB may give us further insight into the effects of surgery on neurological sequelae as well as the optic nerve. 14
Due to the inter-relationship that exists between the blood supply of the choroid, retina, and optic nerve head, any disruption in this blood supply can lead to irreversible damage.15,16
As OPCAB surgery has a more favorable profile of neurological adverse events and evades the systemic inflammatory response seen in ECC, we aimed to determine its effects on choroidal thickness (CT), GCC, and RNFL.
Methods
This prospective longitudinal study included patients who underwent OPCAB at Balikesir University Hospital’s cardiovascular surgical department between June 2015 and June 2016.
Patient selection
Patients from the cardiothoracic surgery department who were to undergo OPCAB with stable ischemic coronary artery disease were examined in the ophthalmology department of Balikesir University Hospital preoperatively and postoperatively at 1 week and 6 weeks after surgery.
Exclusion criteria were a spherical refractive error of ±3 diopters (D), cylindrical refractive error ±2D, glaucomatous optic neuropathy or macular pathology, optic nerve head anomaly, a significant media opacity that precluded good quality fundus imaging, previous intraocular surgery or interventions, ejection fraction below 50%, and uncontrolled diabetes or hypertension. All of the patients included in the study were on aspirin, b-blocker, nitrate, and statin, and these medications were not discontinued preoperatively. Postoperative treatment with the same drugs was continued as standard. Any patient with a change in medication regimen was excluded from the study.
OPCAB procedure
A classic median sternotomy approach was used, and preparation of the left internal thoracic artery harvesting and other conduits was performed using a standard technique. ECC was not used and the heart was not stopped. Mean arterial pressure above 60 mm Hg was maintained throughout the surgery. Major adverse cardiac and cerebrovascular events (MACCE) were evaluated in patients at the postoperative first and sixth-week controls.
Ophthalmological examination
A complete ophthalmological examination, including best-corrected visual acuity (Snellen), axial length, intraocular pressure (Goldmann applanation tonometry), slit-lamp biomicroscopy, and a dilated fundus examination, was performed preoperatively.
All preoperative and postoperative optical coherence tomography (OCT) images were taken by a single experienced technician in enhanced depth imaging mode using spectral domain OCT with a wavelength 840 nm (bandwidth 150 nm) (Cirrus HD spectral domain-OCT Model 4000; Carl Zeiss Meditec, Inc., Dublin, CA, USA). Measurements were taken between 9 am and 11 am to avoid diurnal variation. Patients who were enrolled in the study were instructed to abstain from caffeine and cigarettes 1 week prior to imaging. Using the spectral domain OCT, CT measurements were taken at the fovea from the outer edge of the hyperreflective retina pigment epithelium to the hyperreflective inner scleral border (Figure 1). The average of three separate measurements, taken by a single examiner (KT) who was blinded with regard to the nature of the study, was recorded. RNFL and GCC data were recorded from automated measurements made from the in-built software program. The average, minimum, and six sectoral (superior, inferior, superonasal, inferonasal, superotemporal, and inferotemporal) values were recorded for the GCC. Peripapillary RNFL values from four quadrants (superior, inferior, temporal, and nasal) were recorded.
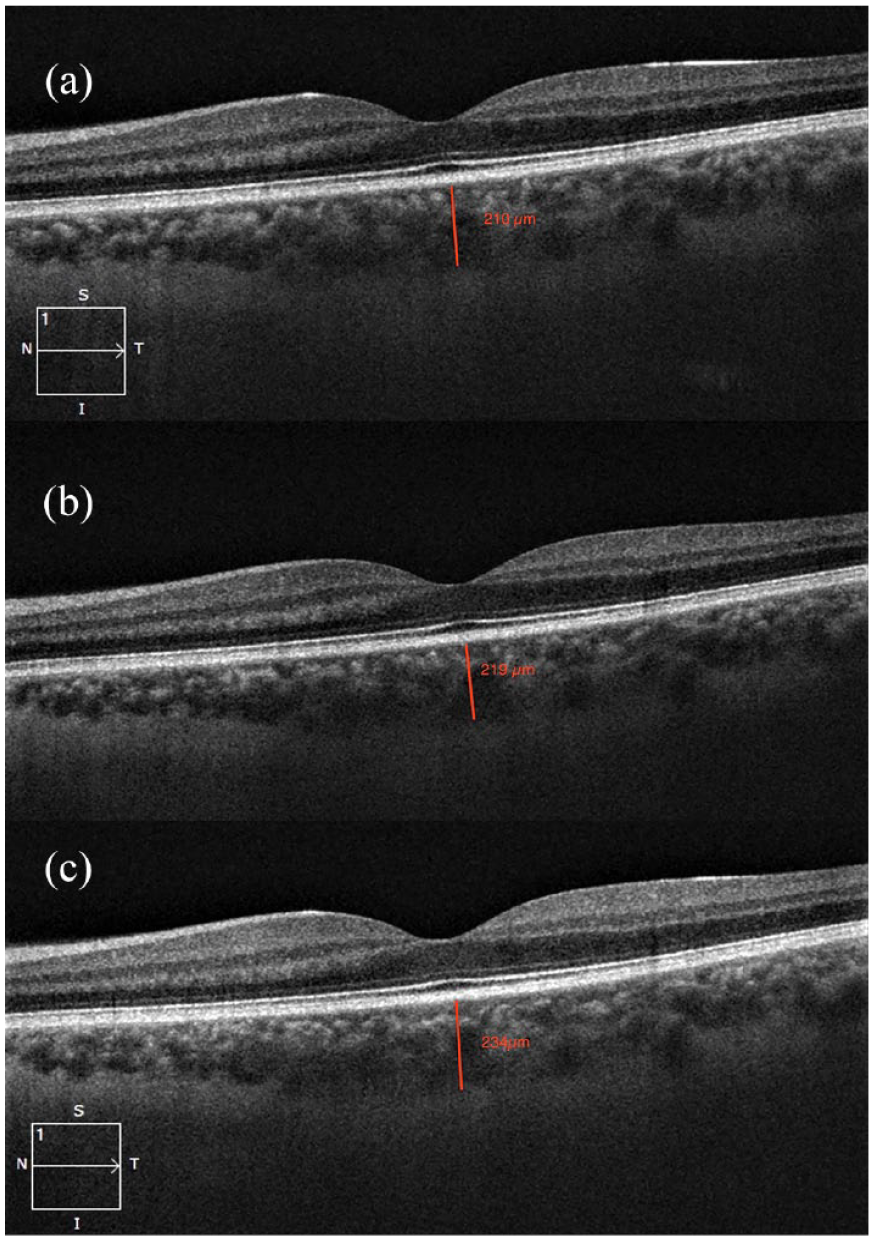
CT was measured at the fovea from the hyperreflective retina pigment epithelium to the hyperreflective inner scleral border. (a) Preoperative CT. (b) Week 1 CT. (c) Week 6 CT.
Statistical analysis
A single eye from each patient was selected for statistical analysis, and the selection was randomized using standard statistical software. 17 Continuous variables were expressed as mean ± standard deviation. The Shapiro–Wilk test was used to determine whether the parameters in the study showed a normal distribution. Paired sample t-test and Wilcoxon signed ranks test were used to compare preoperative and postoperative measurements. p < 0.05 was considered to be statistically significant.
Results
A total of 45 patients were enrolled in the study, with one patient being lost to follow-up. A total of 44 patients were included in the study, the average age of patients who participated in our study was 54.5 ± 13.1. A total of 27 male (61%) and 17 female (49%) patients underwent off-pump coronary artery bypass. Demographic values, as well as clinical characteristics of patients, are summarized in Table 1.
Baseline demographics, ocular measurements, and risk factors of off-pump coronary artery bypass graft patients.

AL, axial length; BCVA, best corrected visual acuity (Snellen); D, diopters; IOP, intraocular pressure; SEQ, spherical equivalent.
There were no visual disturbances reported by any of our patients in the postoperative period. There was a statistically significant increase in subfoveal CT from 252.84 ± 56.24 µm preoperatively to 273.82 ± 39.76 µm at 1 week and 301.97 ± 44.83 µm at 6 weeks after off-pump bypass (p = 0.044; p ⩽ 0.001) (Figure 2).

CT changes after off-pump coronary artery bypass graft surgery. (a) Preoperative CT. (b) Week 1 CT. (c) Week 6 CT.
There was no MACCE in any of the patients at the postoperative first and sixth-week controls.
Nasal retinal nerve fiber layer thickness was measured preoperatively as 67.83 ± 12.24 µm and decreased to 64.70 ± 15.3 µm at 1 week postoperatively and subsequently increased to 65.87 ± 9.20 µm at 6 weeks with an overall decrease in thickness (p = 0.463; p = 0.138), although not statistically significant all other RNFL measurements showed an increase (Table 2).
Retinal nerve fiber layer changes after off-pump coronary bypass graft surgery.

RNFL, retinal nerve fiber layer; P1, preoperative and postoperative Week 1; P2, preoperative and postoperative Week 6.
Postoperatively, there was an increased thickness in all GCC layer measurements; however, these values did not reach significance (Table 3).
Ganglion cell complex changes after off-pump coronary artery bypass graft surgery.

GCC, ganglion cell complex; P1, preoperative and postoperative Week 1; P2, preoperative and postoperative Week 6.
Discussion
The choroid is a rich vascular structure that delivers oxygen and nutrients to the outer retinal layers and provides the main nutrient supply to the fovea, retina pigment epithelium, and outer photoreceptor layer. 18 Disruption of choroidal circulation can lead to rapid and potentially irreversible damage to the highly functioning outer photoreceptor layer and retinal pigment epithelium.19,20 Retinitis pigmentosa, central serous retinopathy, pathological myopia, and age-related macular degeneration (AMD) are some of the few diseases in which choroidal dysfunction plays a role.21–24 Besides ocular diseases systemic diseases have been found to affect the choroid: cardiovascular disease, as well as its treatment, is associated with changes in CT. 25
Choroidal blood flow is regulated by sympathetic, parasympathetic, and neural regulation; this regulation ensures that the retina’s needs are met and also compensates for changes in perfusion pressure.14,26 Our study is the first study to examine the effects of OPCAB on CT, RNFL, and the GCC. Pekel et al. studied CT changes after on-pump surgery, they found a slight postoperative thickening in the subfoveal region, this thickening however was not statistically significant. 4 ECC is not utilized in OPCAB, ECC is associated with oxidative stress and inflammatory response with the release of C-reactive protein, both C-reactive protein and oxidative stress have been associated with thinning of the choroid.27–29
Severe coronary artery disease is the main indication for CABG surgery and subfoveal CT is significantly lower in these patients compared to normal controls (252 versus 303 μm). 30 Our mean CT preoperatively was 252.84 ± 56.24 μm similar to previous age-matched studies. There was a significant increase as early as 1 week after surgery to 273.82 ± 39.76 and an increase to 301.97 ± 44.83 μm at 6 weeks postoperatively. In a study of CT changes in patients with carotid stenosis after carotid endarterectomy, 31 post-surgically patients had a significant increase in CT which was linked to improved ocular perfusion.
In our study as hemodynamic status was kept stable throughout surgery (mean arterial pressure above 60 mmHg), and the lack of adverse outcomes in the early postoperative period leads us to believe that possibly improved ocular perfusion might reverse the effects of coronary artery disease on CT. The preoperative and cardiac output monitoring was not recorded. However, we think that avoiding the heart–lung machine in OPCAB may have prevented the adverse effects of ECC, such as hemodynamic changes and inflammation. This may explain why our CT measurements increased significantly in OPCAB, but not in on-pump surgery. While there are variations between studies CT measurements for the healthy population of our study group ranged from 309.95 ± 60.05 (for patients between 40 and 49 years of age); 278.88 ± 51.29 (50–59 years of age); and 266.50 ± 49.56 (60–73 years of age). 32 Whereas preoperatively our average CT was consistent with those of patients in the sixth to seventh decades; 6 weeks after OPCAB our subfoveal choroidal thickness (SFCT) increased to 301.97 ± 44.83 which correlates with patients in the 4th decade. The increased thinning of the subfoveal choroid with age while physiological is also seen in some diseases such as AMD33,34; according to the World Health Organization, AMD is one of the leading causes of blindness in developed countries and can cause irreversible visual impairment. 35 AMD shares many of the risk factors of cardiac disease and an association with endothelial dysfunction, systemic inflammatory response, and atherosclerosis has been reported.36,37 The progressive thinning seen in these patients is correlated with disease severity, in the elderly population group, choroidal thinning might lead to the progression of AMD or even earlier onset of AMD in high-risk patients. 38
Visual loss after surgery is largely associated with ischemic optic neuropathy as well as emboli thus optic nerve parameter measurements using OCT can help us determine any detrimental effects on the optic nerve due to surgery. 39 In our study, there was no significant change in postoperative retinal nerve fiber layer values at 1 week or 6 weeks postoperatively. Although no studies on the effect of off-pump surgery on RNFL thinning in off-pump surgery, on-pump surgery’s effects on RNFL are conflicting, a study by Buyukates et al., 9 which had a similar design to ours showed significant thinning that returned to normal 1 month after surgery in all but the inferior quadrant. In a study by Pekel et al., 6 in which RNFL thickness 1 month after the coronary bypass was compared to healthy controls, they found no significant difference. Uzun et al. 40 also found no significant change in RNFL thickness 1 month after an on-pump coronary artery bypass. Patients with nonarteritic ischemic optic neuropathy have shown a decrease in GCC prior to RNFL thinning at approximately 1 month after the insult suggesting this could be a more sensitive marker for post-surgical optic nerve damage. 41 GCC showed no significant change in our study at 1 week and 6 weeks after off-pump coronary artery graft surgery.
To our knowledge, this is the first study to measure CT, RNFL, and GCC changes after OPCAB. RNFL and GCC in patients undergoing OPCAB showed no significant differences compared to preoperative values; thus, we can conclude that OPCAB did not have any negative structural effects on the optic nerve head.
Ischemic changes in the RNFL and GCC are not necessarily acute and it may take as long as 1 month for ischemic changes or damage to the optic nerve to translate to ganglion cell and RNFL thickness measurements, in cases such as these CT might be a more direct measurement of hemodynamic changes. 41
Limitations of our study were as follows: A major limitation of our study was the lack of a control group, future studies with a no intervention or on-pump CABG control group could better determine the effect of off-pump surgery on CT, RNFL, and GCC. Sample size/power analysis was not performed but based on previous literature,6,7,9 short follow-up period; lack of retinal perfusion measurements and cardiac output measurements, future studies with a longer follow-up period using OCT angiography to determine perfusion, and studies comparing on-pump and off-pump techniques together with cardiac output could lead to a better understanding of the effects of CABG surgery on the choroid and optic nerve head.
Conclusion
OPCAB showed no negative effects on the RNFL or GCC measurements. A significant increase in subfoveal CT was seen in OPCAB patients postoperatively. Increased CT might indicate improvement after surgery, making OPCAB advantageous in patients who are at high risk or have preexisting ocular diseases that are affected by the choroidal thinning.