
Abstract
Background:
Anthropometry facilitates the evaluation of risks associated with reduced macular pigment optical density (MPOD).
Objectives:
To investigate the predictors and anthropometric indices associated with MPOD in healthy adult in Arab population.
Design:
This is a cross-sectional study.
Methods:
The MPOD was measured at 0.5° from fovea using a heterochromatic flicker photometer. Healthy participants aged between 20 and 40 years were recruited. The study evaluated the following data of the participants: height, weight, body mass index, body fat percentage, basal metabolic rate, visceral fat level, muscle mass, bone mineral content, and percentage of protein and body water. The correlation between MPOD with anthropometrics and demographic data was evaluated using Spearman’s correlation test. The differences among genders were investigated using the Mann–Whitney U test. The smoking effect on MPOD was analyzed using the Friedman test.
Results:
In all, 143 participants were recruited. The median ± interquartile range was calculated for age (23 ± 4 years), visual acuity (0.00 ± 0.00 logMAR), and MPOD (0.41 ± 0.18). The average MPOD was higher in males than in females but it was not statistically significant (p > 0.05); on the other hand, they were statistically significantly different in most of the anthropometric data. A significant relationship was found between MPOD and percentage of body fat, protein, and body water (r = 0.30, p < 0.05). The observed median MPOD value was higher in this study than that found in previous studies in white populations, but lower than that found in studies investigating Asian populations.
Conclusion:
One of the most important risk factors of age-related macular degeneration is associated with a relative absence of macular pigment. This study brought into focus percentage of protein and body water for further studies as well as the well-established links with body fat and obesity. Unknown predictors of MPOD remain uncovered. The study also provided first report on normative values of MPOD for Arab population and confirmed the differences from other ethnicities.
Keywords
Introduction
Carotenoids are a group of pigments that can be categorized into two main groups: carotenes and xanthophylls. 1 Carotenoids are generally found in various tissues of the human body including retina, lens, iris, choroid, and retinal pigment epithelium (RPE).2,3 The three carotenoid forms, lutein (L), zeaxanthin (Z), and meso-zeaxanthin (MZ), are found at high concentrations in the macula lutea and declines rapidly with increasing eccentricity, and those carotenoids are collectively called as macular pigment (MP). 4 Those carotenoids are found in the retina as blue light (or short-wavelength light) filter, and they reduce chromatic aberration and antioxidants.5–7 The macular pigment optical density (MPOD) is the measurement of the ability of the MP to absorb or filter the blue light. Some studies have provided evidence that high-energy visible light may contribute to age-related macular degeneration (ARMD). 8 The ARMD was also linked to other factors including chronic inflammation, oxygen metabolism, and hemodynamic processes.4,9–11 Specifically, the MPOD was found to be significantly lower in ARMD.12,13 The MPOD has become a valuable biomarker for predicting the risk for disease and visual function.14–16 In clinical practice, the most common method for measuring the MPOD is based on heterochromatic flicker photometry (HFP), which is used to measure the spectral sensitivity of the human visual system.12,17
Since three decades, the prevalence of obesity has increased in both adult and child populations as well as in high- and low-income populations. 18 Obesity can be defined as an excess of body fat. Body fat is a major storage organ for carotenoids.7,19 The discrepancy in body fat suggested that it would negatively impact carotenoid levels.7,19 It has also been suggested that obesity increases oxidative stress and inflammation, and shows changes in the lipoprotein profile. 20 It would also result in greater destruction and reduction in circulatory delivery of L and Z to macula. 20 The relationship between body composition indices and MPOD has been inconsistent. Briefly, a significant relationship between body mass index (BMI), 21 waist–hip ratio,21,22 and percentage of body fat was found,2,7 whereas some studies did not find any relationship between MPOD and obesity.23,24
In general, the BMI is a good predictor of variation in lean body mass and fat mass. 25 However, due to small decreases in the weight BMI observed the reduction of: muscle mass and changes in the type and redistribution of body fat, with increased visceral fat, reducing subcutaneous fat and inter- and intramuscular fat might be masked. 25 This may emphasize the fact that investigating MPOD relationship with BMI and body fat may be inadequate and that it could be necessary to examine other anthropometric indices that may be more related to the MPOD. The relationship between MPOD and other important body composites such as basal metabolic rate (BMR), visceral fat level (VFL), muscle mass, bone mineral content (BMC), protein, and body water percentage has been scarcely investigated.
The majority of studies of MP were based on white participants and few investigations in East and South Asian populations.26–28 However, to the best of our knowledge, the profile of MPOD in Saudi Arabia has not yet been investigated. In this study, we aim to assess MPOD in a healthy group of Saudi adults, which would provide this crucial baseline for any future intervention and/or study. Furthermore, to investigate whether any of the body composites mentioned earlier or participants’ characteristics are related to the inter-participants variations in MPOD. Finally, as first report to our knowledge, this study compares the MPOD in Arab adult group with those of Asian and white groups.
Methods
This cross-sectional study was conducted on healthy participants who do not have any ocular disorders and aged between 20 and 40 years. Potential participants were excluded if they had any ocular disorders, previous ocular surgeries, systematic diseases, and color vision abnormality. The participant’s ophthalmic and systemic history was gathered. The best-corrected visual acuity was measured using the Early Treatment Diabetic Retinopathy Study (ETDRS) chart (Precision Vision, LaSalle, IL, USA), 29 the MPOD was examined using the macular pigment screener II (MPS-II®; Elektron Eye Technology, Cambridge, UK), and color vision with Ishihara test. Previous report has suggested that the estimated MPOD value obtained by MPS-II is applicable to both healthy and ARMD individuals. 30 The aforementioned ocular examinations were assessed monocularly (i.e. right eye) to facilitate comparison with previous studies which used similar procedure. This is also to avoid any eventual correlation present between both eyes in a single participant.31,32 This study was conducted from March 2020 to June 2021 in Riyadh, Saudi Arabia.
Visual acuity
The ETDRS chart is one of the most widely LogMAR charts to measure visual acuity (VA). It was designed to be conducted at 4 m. The VA was assessed with the participant’s best refractive correction. The smallest legible letter is recorded for each eye monocularly. The test was stopped when four consecutive letters were incorrectly identified. The ETDRS has five letters per row, each letter has been assigned a value of 0.02 LogMAR, and the VA was recorded based on the identification.
Color vision
The Ishihara test is simple, widely available, and frequently used to screen for color vision deficit. Each plate has a matrix of dots arranged to camouflage a certain number that the participants were asked to identify. Each plate was presented for 4 s and each error made was noted. A participant with ⩾5 plate errors was defined as ‘Color Deficient’. 33
Macular pigment optical density
The MPS-II measures the MPOD using a HFP technique. The mechanism of measuring MPOD with MPS-II has been described previously.34,35 The test is taken under dim light, and the examiner entered the participant information, asking the participant to place their eye in the eyepieces while covering the other eye. The measurement was completed without pupil dilation. The participant should look at three targets and fixate on the central one. The stimulus comprises a blue light (a wavelength of 465 nm) and a green light (a wavelength of 530 nm). The light target has a circular aperture of 1° in diameter; thus, we can obtain MPOD with this device from the 0.5° around foveal center. 34 The participant will be given a response button to press it immediately when they see the light target start flickering. If two measurement errors were observed, the outcome was recorded as nonmeasurable and the participant was excluded, although no participant struggled during the current study. In this study, both estimate MPOD and absolute MPOD values were measured, the raw data were explored, and no statistical significant difference was found between them (p > 0.12) (median ± interquartile range of estimate MPOD = 0.41 ± 0.16 and absolute MPOD = 0.41 ± 0.18); therefore an absolute MPOD was considered in the subsequent analysis.
Anthropometric data
The participants’ height was measured with a stadiometer to the nearest 0.10 cm. Huawei body fat smart scale was used (Model AH 100, Huawei Co., Shenzhen, China), participant with barefoot, empty pockets, and light clothes, to measure several anthropometric data, including weight (to the nearest 0.10 kg), BMI (for adults over 20 years old, the BMI can fall into one of the following categories, BMI < 18.5 referring to underweight, BMI between 18.5 and 24.9 referring to normal weight, BMI between 25.0 and 29.9 referring to overweight, and BMI ⩾ 30 referring to obesity 36 ), percentage of body fat (the essential percentage of body fat in male suggested to be between 2% and 5% and in female between 10% and 13% according to American Council on Exercise), BMR, VFL, muscle mass, BMC, and percentage of protein and body water.
Statistical analysis
Data were entered in the Microsoft Excel sheet (Version 26) and then statistical software SPSS (Version 21.0; IBM Corp., Armonk, NY, USA). The data were explored for normality, and nonparametric test was used (Kolmogorov–Smirnov test, p < 0.05). All outcomes were expressed as the median ± interquartile range. Spearman’s correlation test was conducted to investigate the correlations between the MPOD and the anthropometric data. The effects of gender and smoking on the MPOD were analyzed using the Mann–Whitney U test and the Friedman test, respectively. Finally, the a p value of <0.05 was accepted as statistically significant.
Results
A total of 143 participants (111 males and 32 females aged 20–29 years) were included in the study. All participants have normal color vision (<2 plate errors were encountered). Out of all participants, 32% were smokers or have a history of smoking (38 males and 8 females). The summary of MPOD values and anthropometric characteristics is shown in Table 1.
Summary of the median ± interquartile range of the measured MPOD and participants’ anthropometric data as well as Spearman’s correlation test.

BMC, bone mineral content; BMI, body mass index; BMR, basal metabolic rate; cm, centimeters; kcal/d, kilocalorie per day; kg, kilogram; LogMAR, logarithmic of minimum of angle resolution; MPOD, macular pigment optical density; ns, not significant; VA, visual acuity; VFL, visceral fat level.
Indicates statistical significant.
In detail, the BMI varied between participants where 45% (64 participants) had normal weight, 5.5% (8 participants) underweight, 24.5% (35 participants) overweight, and 25% were obese [16 participants obesity class I (BMI: 30–34.9), 12 participants obesity class II (BMI: 35–39.9), and 8 participants obesity class III (BMI > 40)]. With regard to body fat, in the male participants, a sum of 20 participants (18%) have below average body fat of <18%, 40 participants (36%) have an average body fat of 18–25%, and 51 participants (46%) have an obese body fat of >25%. In the female participants, 8 participants (25%) have below average body fat of <25%, 15 participants (47%) have an average body fat of 25–31%, and 9 participants (28%) have an obese body fat of >31%. With regard to percentage of protein, 18 participants (12.5%, out of them 5 females) have a protein of <10%, 86 participants (60%, 21 of them are females) have a protein of 10–20%, and 39 participants (27.5%, 6 of them are females) have a protein of >20%. For the body water percentage, 46 participants (32%, out of those are 17 females) have 43–50% of body water, whereas 97 participants (68%, out of those are 15 females) have 50–62% of body water content.
Gender- and smoking-based differences
The difference between males and females was found in both the anthropometric data and the MPOD values. There were apparent differences between both genders as shown in Table 1. In comparison to the males, the females were shorter, lightweight, less BMI, lower BMR, less VFL, lower muscle mass, lower protein, lower percentage of body water content but higher percentage of body fat, whereas both genders have similar BMC. These observations were statistically significant except for protein as listed in Table 2. In terms of the MPOD, the females have a lower average MPOD than males but this was not statistically significant (Table 2). The smoking has been found to significantly influence the MPOD scores (Friedman test, X2 = 10.5, p = 0.001). The nonsmokers have a median MPOD of 0.44 ± 0.17, smoker MPOD of 0.37 ± 0.19, and the participants’ MPOD with the history of smoking of 0.40 ± 0.28.
The differences in characteristics between genders using Mann–Whitney U test.

BMC, bone mineral content; BMI, body mass index; BMR, basal metabolic rate; cm, centimeters; kcal/d, kilocalorie per day; kg, kilogram; MPOD, macular pigment optical density.
Indicates statistical significant.
The relationship between the MPOD and anthropometric data
Spearman’s correlation coefficient test was conducted for all measured anthropometric data (Table 1). A significant mild relationship was found between the MPOD and the percentage of protein and body fat as well as with the percentage of water in body (Table 1).
Participants with low MPOD
Participants with the highest MPOD values of >0.70 and with lower MPOD values of <0.2 were explored with in-depth insight at their background characteristics (Table 3). It has been observed that the factors found in the earlier analysis seem to be fundamentals for higher or lower MPOD values. From Table 3, gender, smoking, higher body fat, lower protein, and lower water percentage appear to be the main determinants of the MPOD values.
The characteristics of participants having low and high MPOD values.

MPOD, macular pigment optical density.
Arabs versus Asian and white MPOD comparisons
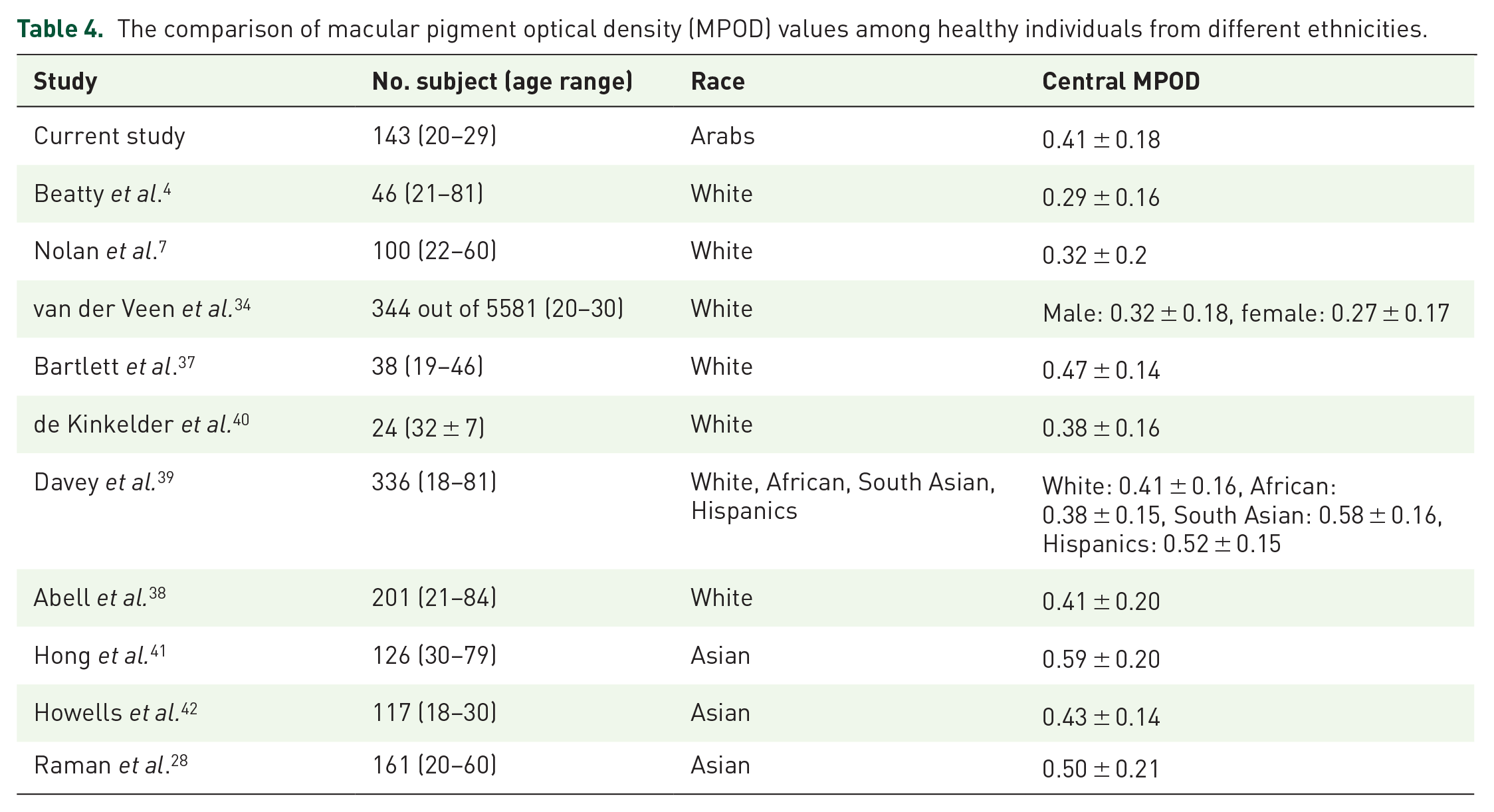
The median MPOD of the Arab participants in the current study (0.41) was higher than most previously published MPOD values in white population, exceptions being the MPOD values reported in Bartlett et al. 37 and was equal to those reported in Abell et al. 38 and in Davey et al. 39 (0.47 and 0.41, respectively) (Table 4). The studies included Asian participants reported higher MPOD values than other predominantly white participants as well as the current study (Table 4).
The comparison of macular pigment optical density (MPOD) values among healthy individuals from different ethnicities.
Discussion
This study was designed to investigate the relationship between MPOD and BMI, body fat percentage as well as other important body composites including percentage of body water and protein, BMR, VFL, muscle mass, and BMC. The ARMD is one of the most frequent causes of vision loss in the central visual field, which is mainly caused by the loss of retinal cells along with MP.43,44 It affects a high number of people at the age of above 65. 45 Specifically, the ARMD prevalence rate in Saudi Arabia is estimated to be 3.3% of the major causes of blindness in patients over 50 years. 46 Previously, it has been suggested that racial background is a factor in developing ARMD. 47 The significance of this study besides investigating the relationship between the MPOD and body composite indices, it has also provided a normative MPOD profile for participants from Arab ethnicity as a first report to our knowledge.
In general, the measurement of MPOD is anticipated to increase the macular protective effect by giving the chance for people with low MPOD to take proactive actions such as taking various supplements. 24 Therefore, routine screening for people over 50 years is suggested to help detecting early low MPOD and identify the people who should take protective actions. 41 The MPS-II is a reliable and reproducible instrument,34,35 and important in terms of ARMD screening in the country and also in planning public health policies.
The group median of MPOD was 0.41 ± 0.18, similar to a previous report with no statistical significant difference based on gender. 28 Although the average MPOD was higher in males than in females, this finding was in agreement with previous reports.2,42 The anthropometric data were significantly different between genders except in the BMC measurements. These differences can be accounted to the physiological and hormonal variances between both genders. For example, the essential body fat percentage is greater in women than in men, due to the demand of hormonal function and childbearing, as would be expected the women tended to have a higher percentage of body fat than did the men, 48 which is supportive to the finding of the current study. In addition, these results can be further explained from the finding of previous studies which indicated that men have a worse lifestyle with lower prevalence of physical activity and a higher prevalence of smoking.25,49
The risk of ARMD was linked to the consumption of fruits and vegetables, which could indicate a healthy lifestyle, as early as 1988. 50 In the current study, an inverse relationship existed between MPOD and the percentage of body fat, and this observation has also been consistent with the results found in previous studies.2,7,51,52 One possible explanation that accounts for the relationship between the body fat and MPOD is the hypothesis that the body fat would be in direct competition with the retina for absorbing lutein and zeaxanthin. 51 Therefore, variation in the percentage of body fat may be estimated to impact carotenoid levels in serum that takes up carotenoids, such as the retina.2,53 Furthermore, a previous study suggested that reticular pseudodrusen, which linked to ARMD, was less frequent in patients taking lipid-lowering drugs. 54 In addition, the previous study reported a significant positive relationship between increases in concentrations of lutein and body fat loss. 53 Obesity is expected to lead to high-density lipoprotein (HDL)-cholesterol, which is believed to be an effective transporter of L and Z to the retina. Thus, a high HDL-cholesterol could subsequently decrease delivery of the macular carotenoids.24,55,56 Finally, a statistical insignificant relationship between MPOD and BMI was found in this study. This was in contrary to findings in previous studies,2,57–59 and another study which reported significant relationship between BMI and MPOD in males and nonsignificant in females. 7 However, as stated earlier in the introduction, the BMI is a good predictor of variation in body fat mass. The relationship between BMI and the percentage of body fat in the current study was a strong significant relationship (r = 0.77, p < 0.0001). Thus, this finding might suggest that both BMI and the percentage of body fat is of good relationship with MPOD, although our finding suggests that the percentage of body fat might be a more sensitive measure.
The second body composition to have a relationship with MPOD in the current study was the percentage of body protein. Protein is one of the crucial functional components of living cells and is involved in maintaining all life processes. 60 Protein oxidation (i.e. alterations in the protein structure which may subsequently lead to compromised protein function) has been suggested to be involved in the progression of aging as well as the development of some age-related diseases. 60 Specifically, protein oxidation has been suggested that it may contribute to pathogenesis of ARMD.61,62 The onset of ARMD is believed to be related with lipofuscin accumulation in the RPE. 63 Lipofuscin is also recognized as the precursor of drusen (i.e. yellow aggregates of extracellular materials such as debris that build up in Bruch’s membrane), which is a major sign of ARMD pathology. 64 These physical changes can lead to chronic inflammation as a target of immune reactions. 65 These suggested roles of the accumulated oxidized proteins and lipofuscin in the pathophysiology of the disease (including ARMD) would lead to clinical studies investigating the efficacy of antioxidant and zinc supplementation to slow down the progression of the disease. 66
The percentage of body water content has also similar relationship with the MPOD to that found with body fat and protein. Water has several functions in the body, it acts as, but not limited to, a building material; a reaction medium and a reactant; and as a carrier for nutrients. 67 Body water is stored predominantly in the fat-free mass. 68 Therefore, body water mainly depends on the person’s fatness. 68 This is supportive to the observed relationship between the percentage of body fat and water content found in the current study (r = −0.95, p < 0.0001). Dehydration can affect many parts of the body organs including the eye level (e.g. hypotonia of ocular globes and dry eye).68,69 The water requirements of the eye vary which is based on numerous factors including climate, physical activity, and diet. 67 Hot countries like Saudi Arabia might impact healthy people’s hydration level; therefore, keeping the body hydrated all the time might improve the MPOD value. Medical practitioner faces challenges to know whether the healthy people is in a good or bad range in terms of their total or extracellular water content due to the unavailability of a reliable reference values with which to compare the measurements. 68
Smoking has also been found to have a link with MPOD in the current study. This finding was consistent with the previous reports; for example, McCarty et al. 70 suggested that smokers over 40 years are two- to four-folds at risk of developing ARMD than nonsmokers of the same age.
In general, it would be possible that the relative reduction in MPOD in people with higher body fat and obesity, lower protein, and low water content may basically reflect a poor diet, and previously it has been established that obesity is associated with lack of dietary intake of carotenoids which are the foundation of the MP.2,7,21 A meta-analysis of six studies proposed that the high intakes of dietary L/Z may be protective against late ARMD, and further studies are suggested to confirm these relationships. 71 Nonetheless, it must be noted that the relationship found between those three body composites and MPOD is relatively low in strength, and it was in agreement with the majority of previous studies.2,7,51,52,57–59 Specifically, the present relationship was 0.30 in strength which means that, for example, the percentage of protein shares only 9% of the variation with the MPOD values and the three body composites collectively could explain about the 25% of the variation in MPOD values. This result points out the need for future studies to investigate what other factors may explain comprehensively the pathogenesis of ARMD.
The differences in MPOD across ethnicities were observed. The Asian population showed the highest MPOD among both white and Arab populations. This was also obvious in Davey et al.’s 39 study in 2020, where participants from Asian and Hispanic background had a higher MPOD than participants from white and African background. In the current study, the MPOD of the Arab participants was higher than those from white populations and lower than Asian populations. This finding might suggest that participants from Arab population are distinct from Asian populations and future studies shall be directed to provide normative profile across Arab populations. Furthermore, the differences in MPOD when considering ethnicities could also be linked to iris color; therefore, future studies might be needed to compare MPOD in participants with lighter and darker iris color in relation to ethnicities. These results also suggest that white population might be at a higher risk of ARMD than people from other ethnicities. It should also be noted that it is difficult to compare MPOD across studies because of the different methodologies, experimental setup, and procedures used. 26 Finally, while those studies listed in Table 4 recruited healthy participants, certainly they vary in terms of their anthropometric data, diet, physical activities, BMI, hydration level, protein, etc. This could also explain the variation observed within, for example, the studies that investigated white ethnicity.
The present study has some limitations as well as strengths. The limitations involve the cross-sectional design and younger age group. A longitudinal research would be needed to explore changes in the anthropometric data on an extended period of time. Furthermore, due to lack of studies of this nature, future study would be needed to investigate anthropometric data in elderly population. These studies shall use a large sample according to age and sex with individuals aged 60–80 years in correspondence to growing number of elderly people in the middle-east region. The recruited sample was 32 males and 111 females, a more balanced gender-based recruitment and conducting a power sample size calculation would be more appropriate; however, this study was conducted during the COVID-19 pandemic which made the recruitment very challenging and the study extended for a long period of time that made keeping it going is not feasible. Furthermore, this study recorded the MPOD in the right eye and although it is probably there is no difference among right and left eyes that would change this study findings, it could be more appropriate in future studies to record the measurements of both eyes and then select one reading randomly from each participant. On the other hand, the core strengths of this study include the use of new anthropometric measurements that brought into focus the protein and body water content as factors linked to MPOD. This study also reported for the first time, to the best of our knowledge, MPOD baseline in a healthy group of Arab adults and compare them with those of Asian and white populations. Future studies shall also focus on factors that would impact MPOD, such as diet or supplement intake to further understand the risk factors associated with lower MPOD measurement. In conclusion, a significant inverse relationship between percentage of body fat and MPOD was found. It has also been demonstrated that there are associations between percentage of protein and body water content and MPOD. These two latter factors were brought into focus for further investigation and exploration. This study also provided normative median MPOD value in people from Arab population and showed the differences between various ethnicities. The median MPOD values in Arab participants were higher than in white population and lower than in Asian population.