
Abstract
Background:
A number of articles report the association of polypoidal lesions and choroidal nevi; however, the relationship between choroidal nevi and pachychoroidal disorders has not been studied.
Objectives:
To study the prevalence of choroidal nevi in central serous chorioretinopathy (CSCR) patients and to elucidate potential differences in the clinical characteristics of CSCR in patients with and without choroidal nevi.
Design:
Case-control study.
Methods:
This study included a retrospective analysis of medical records and multimodal imaging data of CSCR patients and a prospective evaluation of the prevalence of the choroidal nevi in age- and sex-matched healthy controls. All participants received comprehensive ophthalmic examination and multimodal imaging including infrared scanning laser ophthalmoscopy in dark-field mode to detect choroidal nevi in the central 40° × 60° region.
Results:
A total of 199 CSCR patients (160 males and 39 females, 47.9 ± 9.4 years) and 184 age-matched healthy individuals (139 males and 45 females, 44.8 ± 12.5 years) were included. Choroidal nevi were detected in 24 (12.1%) CSCR patients and 10 (5.4%) healthy controls (p = 0.01). CSCR patients with choroidal nevi had statistically significantly higher subfoveal choroidal thickness, lower best-corrected visual acuity, and lower central retinal thickness (p < 0.05) than CSCR patients without choroidal nevi. The odds ratio for the presence of chronic CSCR in patients with choroidal nevi was 27.0 (95% CI: 3.1–231.9, p = 0.003).
Conclusion:
The prevalence of choroidal nevi among patients with CSCR is higher than in age- and sex-matched healthy population. Choroidal nevi may be associated with chronic CSCR.
Introduction
Central serous chorioretinopathy (CSCR) is a macular disorder caused by changes in choroidal hemodynamics followed by secondary alteration of retinal pigment epithelium (RPE) and the accumulation of subretinal fluid.
The choroid plays a key role in pathophysiology of CSCR. Choroidal vessels are subjected to venous overload and demonstrate dilation and hyperpermeability of large choroidal vessels. 1 This leads to compression and dysfunction of the choriocapillaris, alteration of RPE followed by subretinal leakage. 2 Study of the structure of the choroid is therefore crucial for the understanding of the pathophysiology of CSCR.
Choroidal nevus is a benign neoplasm of the choroidal stroma deriving from melanocytes which can potentially affect the morphology and microcirculation of the choroid. 3 Specifically, accumulation of subretinal fluid is a well-known phenomenon in choroidal nevi caused by alteration of the choriocapillaris and RPE similar to CSCR or by the appearance of choroidal neovascularization. 4 Moreover, almost a dozen cases of association between polypoidal lesions and choroidal nevi have been described.5–12 This association may indicate a link between choroidal nevi and the pachychoroidal spectrum proposed by some authors. So far until now, the relationship between choroidal nevi and pachychoroidal disorders has not been studied.
In clinical practice, we observe choroidal nevi in CSCR patients, but their prevalence and clinical relevance for CSCR are not known. This study aims to establish the prevalence of choroidal nevi in CSCR patients compared to age- and sex-matched healthy population and to elucidate potential differences in the clinical characteristics of CSCR in patients with and without choroidal nevi.
Material and methods
This study included a retrospective analysis of a local clinical database of ophthalmology department of S.M. Kirov Military Medical Academy and multimodal imaging data of CSCR patients diagnosed between February 2018 and February 2023 and a prospective evaluation of the prevalence of the choroidal nevi in an age- and sex-matched healthy cohort. Healthy participants were recruited from candidates for laser-assisted in situ keratomileusis after comprehensive ophthalmic examination and from individuals who were undergoing routine ophthalmic examination. The study followed the ethical standards stated in the Declaration of Helsinki. Only Caucasians were included in this study. Inclusion criteria for CSCR patients were an age range of 18–70 years and the presence of active CSCR, defined as the presence of subretinal fluid with an increase of choroidal thickness and vascularity and RPE alteration. Exclusion criteria were optical media opacities affecting quality of multimodal imaging, glaucoma, other retinal diseases except CSCR, previous retinal surgery except for laser treatment, incomplete multimodal imaging data, and significant refractive errors (myopia more than 6.0 D or hyperopia more than 2.0 D). Multimodal imaging data were available for both eyes of every patient and included optical coherence tomography (OCT) and OCT angiography (OCTA) performed with RTVue-XR Avanti (Optovue, Fremont, CA, USA), and scanning laser ophthalmoscopy (SLO) performed with F-10 Scanning Laser Ophthalmoscope (NIDEK, Gamagori, Japan).
Scanning laser ophthalmoscopy
Since infrared light deeply penetrates the choroid, the methods operating with this light including SLO, demonstrate high diagnostic potential in evaluation of choroidal nevi. 13 In this study, we used a specific SLO mode called dark-field scanning laser ophthalmoscopy (DF-SLO), which is routinely performed in all CSCR patients at our center. This modality previously revealed high diagnostic ability in the imaging of choroidal nevi. 13 DF-SLO operates with 830 nm laser source of infrared light and an aperture with a central stop, which allows registration of the infrared light backscattered by the inner scleral surface. Any pigmented mass of the retina or choroid would therefore be displayed as a dark region on the homogeneously bright background due to the blockage of this backscattered light. The DF-SLO image covers 40° × 60° of the eye fundus. Since the study was retrospective, only images centered on the foveal center were included (Figure 1).
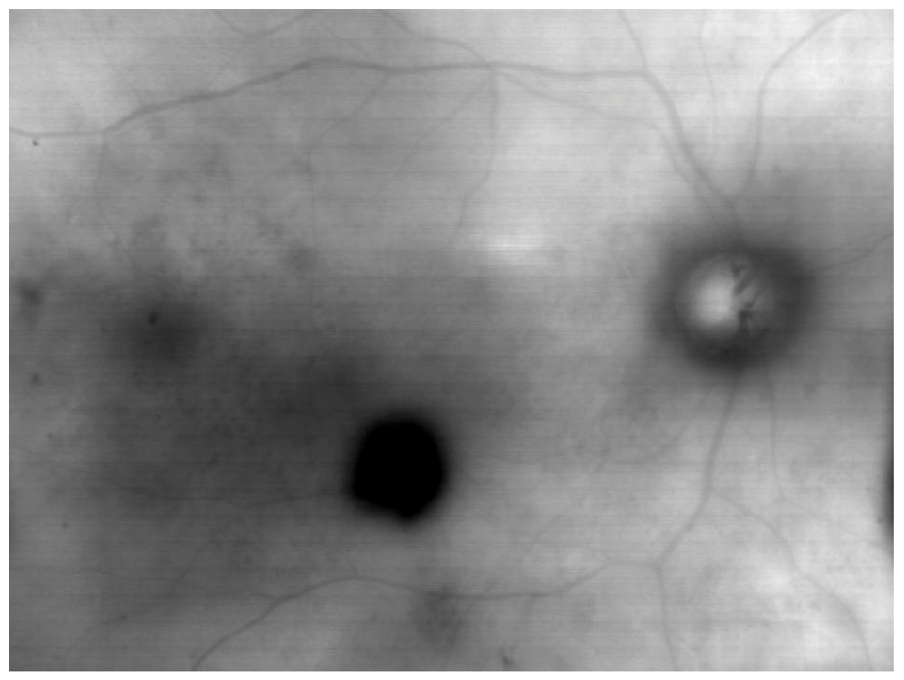
Representative example of choroidal nevus in the healthy eye of a patient with central serous chorioretinopathy displayed with dark-field scanning laser ophthalmoscopy.
Choroidal nevus was defined as a roundish or irregularly shaped dark spot with blurred appearance. This definition allows the differentiation of nevi from pigmented lesions of the RPE, such as congenital hypertrophy of the RPE, which have a clear appearance and sharp borders. If only a part of the nevus was visible on the image, the eye and the patient were considered as having nevi. In every positive case, the number of nevi was counted and the coincidence of the nevi with active CSCR was assessed. In the prospective part of the study, DF-SLO was performed with healthy individuals undergoing routine ophthalmic examination to assess the prevalence of the choroidal nevi.
OCT and OCT angiography
OCT data were retrospectively analyzed to assess central retinal thickness (CRT), subfoveal choroidal thickness (SCT), and the presence of choroidal neovascularization. CRT value was automatically generated by the Macular Map protocol and taken for the analysis. SCT was manually measured on cross-sectional scans with enhanced depth imaging function as a mean of three measurements of the distance between RPE and the sclerochoroidal junction beneath the foveal center. For all patients, 6-mm OCTA scans were evaluated. The presence of choroidal neovascularization was assessed on the OCTA projection of the standard choriocapillaris slab.
Clinical characteristics
All CSCR patients were divided in chronic (more than 6 months of symptoms) and acute forms. Recurrent CSCR was defined as two or more documented episodes of subretinal fluid accumulation due to CSCR. Additionally, the presence of subretinal fluid and/or pigment epithelial detachment and/or outer retinal atrophy after previous CSCR episodes was assessed based on all multimodal imaging data. The patient was considered as having signs of CSCR in the fellow eye in any of those cases.
Statistic
MedCalc 18.4.1 (MedCalc Software, Ostend, Belgium) was used for statistical analysis. The data are presented as a mean ± standard deviation. Chi-square test was applied to assess statistical significance of the difference in prevalence of choroidal nevi between CSCR patients and healthy age- and sex-matched controls. One-way ANOVA was used for assessment of quantitative data including CRT, SCT, and age between CSCR patients with and without choroidal nevi. Since patients with choroidal nevi were significantly less prevalent than those without nevi the latter were randomly selected in comopatible number. A logistic regression model was constructed to evaluate the relationship between presence of the nevi, age, CRT, and SCT. Odds ratio was calculated for the presence of choroidal nevus in CSCR patients versus healthy controls and for the presence of chronic CSCR in a CSCR patient with choroidal nevus. p < 0.05 was considered statistically significant.
Results
A total of 199 CSCR patients (160 males and 39 females, 47.9 ± 9.4 years) met the inclusion criteria. Mean best-corrected visual acuity (BCVA) was 0.12 ± 0.2 LogMAR (≈20/25 Snellen equivalent). Among this group 24 (12.1%) patients with choroidal nevi were detected. The mean age of CSCR patients with and without choroidal nevi was 48.3 ± 11.0 years and 47.6 ± 9.4 years (p = 0.11), respectively, with no difference in the male-to-female ratio (22 males and 2 females, p = 0.22). The control group included 184 healthy individuals (139 males and 45 females, 44.8 ± 12.5 years) and choroidal nevi were detected in 10 individuals (5.4%). No difference in age or male-to-female ratio was found between CSCR and the control group (p > 0.05); however, the prevalence of the choroidal nevi among CSCR patients was statistically significantly higher than among the healthy individuals (p = 0.01). Odds ratio for the presence of a choroidal nevus in either eye of CSCR patients versus healthy person was 2.4 (95% CI: 1.1–5.1, p = 0.026).
In 13 out of 24 patients, a choroidal nevus was found in the eye with active CSCR. Among CSCR patients with nevi, no statistically significant difference was found in mean age, CRT, or SCT between active CSCR eyes with or without nevi (p > 0.05).
Among CSCR patients with choroidal nevi, three (12.5%) patients had choroidal nevi in both eyes (Figure 2). Five eyes of the four patients (16.7%) had multiple choroidal nevi. In those eyes where the nevus at least partially occupies the macular region (n = 13) and was captured by OCTA, no local changes of choriocapillaris perfusion associated with the nevus were found.

Multimodal imaging in a 36-year-old male with central serous chorioretinopathy in right eye persisting over a year. (a) Dark-field scanning laser ophthalmoscopy shows two relatively small choroidal nevi in the right eye. (b) Dark-field scanning laser ophthalmoscopy shows one choroidal nevus in the left eye. (c) Optical coherence tomography cross-sectional scan shows flat neurosensory detachment in the right eye. (d) Optical coherence tomography cross-sectional scan shows normal macula in the left eye.
Among CSCR patients with choroidal nevi 10 out of 24 (41.7%) patients had signs of CSCR in the fellow eye, including pigment epithelial detachment, asymptomatic subretinal fluid, or outer retinal atrophy after a previous leakage.
Twelve (50.0%) and three (12.5%) CSCR patients with choroidal nevi had chronic and recurrent disease, respectively (Figure 3). In six eyes of the six CSCR patients (25.0%) with choroidal nevi, OCTA revealed the presence of choroidal neovascularization (Figure 4) and in one eye (4.2%)—posterior cystoid degeneration. According to OCTA none of these cases had CNV within the nevus.

Multimodal imaging in a 52-year-old female with central serous chorioretinopathy in both eyes with multiple recurrences over 5 years. (a) Dark-field scanning laser ophthalmoscopy shows subtle pigmentary changes in the right eye. (b) Dark-field scanning laser ophthalmoscopy shows one choroidal nevus in the left eye. (c) Optical coherence tomography cross-sectional scan shows flat neurosensory detachment and choroidal folds in the right eye. (d) Optical coherence tomography cross-sectional scan shows flat neurosensory detachment in the left eye.

Multimodal imaging in a 54-year-old female with chronic central serous chorioretinopathy in the right eye. (a) Dark-field scanning laser ophthalmoscopy shows multiple nevi and pigmentary changes in the right eye. (b) Dark-field scanning laser ophthalmoscopy shows multiple lightly pigmented choroidal nevi in the left eye. (c) Optical coherence tomography cross-sectional scan shows flat neurosensory detachment in the right eye. (d) Optical coherence tomography cross-sectional scan shows normal macula in the left eye. (e) Optical coherence tomography angiography (OCTA) projection of outer retina slab shows choroidal neovascularization in the right eye. (f) OCTA projection of choriocapillaris slab shows choroidal neovascularization in the right eye. (g) OCTA projection of outer retina slab shows no abnormal flow signals in the right eye. (h) OCTA projection of choriocapillaris slab shows no abnormal flow signals in right eye.
Among 28 age-matched CSCR patients without nevi, 5 (17.9%) had signs of CSCR in the fellow eye, 1 and 2 patients had chronic and recurrent disease, respectively. Choroidal neovascularization was found in two eyes of the two patients.
The odds ratio for the presence of signs of CSCR in the fellow eye for patients with choroidal nevi was 4.3 (95% CI: 1.1–16.3, p = 0.03). The odds ratio for the presence of chronic CSCR in patients with choroidal nevi was 27.0 (95% CI: 3.1–231.9, p = 0.003). CSCR patients with choroidal nevi had statistically significantly higher SCT, lower BCVA, and lower CRT (p < 0.05) than the CSCR patients without choroidal nevi (Table 1). In the logistic regression model, older age (β = 0.097, p = 0.018) and thicker choroid (β = 0.008, p = 0.025) were statistically significantly associated with the presence of choroidal nevi in CSCR patients.
Characteristics of CSCR in patients with and without choroidal nevi.

BCVA, best-corrected visual acuity; CNV, choroidal neovascularization; CRT, central retinal thickness; CSCR, central serous chorioretinopathy; LogMAR, logarithm of the minimum angle of resolution; PCD, posterior cystoid degeneration; SCT, subfoveal choroidal thickness.
Discussion
In this study, based on the use of dark-field SLO for the diagnosis of choroidal nevi within the central 40°×60° of the eye fundus, we found an increased prevalence of choroidal nevi in patients with active CSCR as high as 12.1% compared to 5.4% in healthy controls. We found no association between the presence of the choroidal nevus and the risk of CSCR in the same eye since the nevus can be presented in the fellow unaffected eye. However, the patients with CSCR and choroidal nevi trended toward a chronic or more severe course of the disease independently of the laterality of both conditions. This agreed with the higher SCT and lower CRT in the eye with active CSCR when a CSCR patient has a choroidal nevus in either eye.
It is well-known that the pathophysiology of CSCR is tightly related to steroid hormones. Particularly, exogenous glucocorticoids is an important risk factor in CSCR and may trigger the active form of the disease. 14 Similar risks seem to exist for exogenous androgens, including testosterone. 15 On the other hand, the data on the level of endogenous sex hormones and aldosterone in CSCR are varying between various studies. Brinks et al. 16 failed to find the changes in sex hormones in males with CSCR. Alternatively, Schellevis et al. 17 has showed increased levels of androsterone, estrone, etiocholanolone, and androstenedione in patients with chronic CSCR. Zakir et al. 18 have found an association between CSCR and an increased serum cortisol level measured at 8.00 a.m. 18 . Androgen and progesterone receptors but not the receptors to estrogens were found in abundance in the tissue of nevi.19,20 Moreover, males with choroidal melanoma have a poorer prognosis and a higher risk of metastasis compared to females. 21 Some authors even consider human melanocytes as androgen target cells. 22 This leads us to a suggestion that sex hormones may play a role in the occurrence of choroidal nevi since melanotic neoplasms. Interestingly, it is known that pregnancy may potentiate melanocytic nevi growth 23 and at the same time, pregnancy increases the risk of CSCR, 24 while maternal serum testosterone concentrations increase by 70% during pregnancy. 25 CSCR patients may therefore have a higher prevalence of choroidal nevi since they share risk factors common to both conditions: male gender and higher levels of steroidal sex hormones including androgens. 26 Since androgens, may exacerbate CSCR, they can also affect the severity of the disease which may explain the greater severity of CSCR in patients with choroidal nevi. The choroidal nevi therefore may be considered as a surrogate biomarker for the severity of CSCR. Indeed, higher choroidal thickness and lower neurosensory detachment, as well as a trend toward higher frequency of fellow eye involvement and choroidal neovascularization, noted in patients with choroidal nevi are the known biomarkers of chronic CSCR.27,28 This agrees with the higher prevalence of chronic CSCR among patients with choroidal nevi. These findings also correlate with a growing number of reports on coincidence of choroidal nevi and polypoidal lesions since both CSCR and polypoidal vasculopathy belong to the pachychoroidal spectrum.5–12
Dark-field SLO, a modification of confocal infrared SLO, used in this study previously demonstrated a high sensitivity and specificity in the detection of the choroidal nevi with an area under the ROC curve of 1.0. 13 This fact as well as routine documentation of the CSCR cases using this option in our center allowed us to conduct this study. Although OCTA in this study was used mostly to detect CNV, some nevi occupying the macular region were captured and available for evaluation with this method. In accordance with previous studies we found no significant changes of choriocapillaris perfusion and this fact agrees with the suggestion that the link between choroidal nevi and CSCR is indirect.29–31
This study has several limitations. Firstly, we used a specific imaging modality, DF-SLO. The use of color fundus photography could lead to other results in prevalence of the choroidal nevi. However, the control group in this study demonstrated significantly lower nevi prevalence with the same imaging technique. Secondly, this study was based on the posterior pole images and a wide-field imaging could further increase the prevalence of the nevi in both groups. 32 This point is important because we do not know if the distribution of choroidal nevi within the eye fundus is dependent on the presence of CSCR. Thirdly, we did not assess the size of the nevi in the study groups since this was beyond the aim of the study and the total number of the nevi was rather small. However, this could help explain the nature of the different prevalence of choroidal nevi between CSCR patients and age- and sex-matched controls. Another limitation was the retrospective nature of the analysis of CSCR patients. Finally, the prevalence of choroidal nevi varies among ethnicities, and since only Caucasians were included in our study we cannot extrapolate our result to other ethnic groups without additional studies.
In conclusion, we found a significantly higher prevalence of the choroidal nevi in CSCR patients compared to the age- and sex-matched controls. In general, CSCR patients with choroidal nevi have thicker choroid, lower neurosensory detachment, lower visual acuity, and higher rate of chronic CSCR. Although, a causative relationship seems unlikely between choroidal nevi and CSCR, these two conditions may share common risk factors. All of this indicate that choroidal nevi may be considered as a potential biomarker in CSCR. Further studies are required on the choroidal nevi as a biomarker in CSCR.