
Abstract
Background:
Cycloplegic drops are commonly used in ophthalmology practice. Changes in anterior segment parameters may occur after cycloplegia. These changes can be evaluated with corneal topography.
Objective:
This study aimed to compare the effects of 1% cyclopentolate hydrochloride and 1% tropicamide on anterior segment parameters using the Sirius Scheimpflug imaging technique.
Design:
A cross-sectional study.
Methods:
One hundred twenty eyes of sixty healthy volunteers with spherical equivalent (SE) values of 0 to ±1 diopter (D) were studied. The right eye of each subject had instillation of cyclopentolate hydrochloride 1% (Group 1) and the left eye of each subject had instillation of tropicamide 1% (Group 2). SE, intraocular pressure, and corneal topography measurements were performed before and 40 min after instillation were compared.
Results:
In Group 1, SE, aqueous depth, anterior chamber depth, iridocorneal angle (ICA), anterior chamber volume (ACV), and pupil size (PS) values were significantly increased (p < 0.001, p = 0.01, p < 0.001, p = 0.03, p < 0.001, and p < 0.001, respectively). In Group 2, SE, ICA, ACV, and PS were significantly increased (p < 0.001 for all). Keratometric values (K1 and K2) and central corneal thickness changed insignificantly in both groups (p > 0.05). The effects of the two administered agents on all parameters were similar (p > 0.05).
Conclusions:
Cyclopentolate hydrochloride and tropicamide affected SE, ICA, ACV, and PS values significantly. These parameters are important in intraocular lens (IOL) power calculations. PS is also important in refractive surgery and cataract surgery with multifocal IOL implantation. Although there was an insignificant difference between the agents, the effects of tropicamide on the parameters were smaller than those of cyclopentolate.
Keywords
Introduction
Cycloplegic agents are a part of eye examinations. Although cycloplegia is commonly used in children with refractive errors and other binocular problems, these agents are used for some situations such as determining the correct refraction, evaluating the anterior segment, and examining the fundus.1,2 The agents that are used most often for cycloplegia are atropine, cyclopentolate, and tropicamide. Clinical use of cyclopentolate and tropicamide agents are more frequent, although atropine is the gold standard for cycloplegia. However, the effects of atropine start later and last longer (2 weeks), and side effects are frequent.3–5 Cyclopentolate is a synthetic antimuscarinic agent. The effects of this agent start at about 25–75 min and recovery may take up to 6–24 h. 6 There are ocular side effects such as irritation, allergic blepharoconjunctivitis, and intraocular pressure increase. Systemic ataxia disorientation, speech impairment, and hallucinations may also occur. 7 Tropicamide is a synthetic analog of tropic acid. Its effects start at 20–30 min and continue for up to 6 h. 8 Systemic side effects such as sensations of the eye sinking, corneal irritation, tachycardia, dry mucous membranes, and flushing can be seen. 7 Tropicamide is preferred more often because its effects start earlier and it has fewer side effects than other agents.
In literature, there are some studies that investigated the effects of the agents in different dosages. Alghamdi et al. reported that a topical dosage of cyclopentolate 1% showed significant changes in anterior chamber angle and anterior chamber volume (ACV) among the hyperopia and myopic groups compared to 0.5%. 9 It has been understood that dosage differences may affect the effects of anterior segment parameters at different levels. In our study, we used same dosage of the agents.
The cornea is responsible for approximately two-thirds of the refractive power of the eye. 10 Therefore, corneal parameters are important for both diagnostic and therapeutic purposes. 11 The evaluation of the anterior segment is important in refractive surgery planning, glaucoma diagnosis, and monitoring, especially in the evaluation of cataracts.12,13 In addition, to calculate the correct intraocular lens (IOL) power, the anterior segment parameters are important, such as in cases of phakic IOL or iris fixation IOL.2,14,15 In these situations, it is important to know how the refraction and anterior segment parameters change after cycloplegia.
In the literature, most studies that investigated the effects of cycloplegic agents on refraction and anterior segment parameters were performed with children or different groups of adults. In this study, we aimed to evaluate and compare the effects of two different agents (1% cyclopentolate and 1% tropicamide) on refraction and anterior segment parameters in the same individuals.
Methods
In this cross-sectional study, a total of 120 eyes of 60 participants randomly selected from among healthy participants aged 20–50 years were included. There were no abnormalities in the anterior segment structures and fundus examination results using slit-lamp biomicroscopy and a 90-diopter (D) lens.
The exclusion criteria were as follows: (1) best-corrected visual acuity (BCVA) worse than 0.00 LogMAR; (2) spherical equivalent (SE) of greater than +1 D or less than −1 D; (3) cataracts; (4) intraocular pressure (IOP) greater than 21 mmHg; (5) cup/disc ratio greater than 0.3; (6) history of intraocular surgery, laser treatment, or trauma and presence or history of any intraocular diseases including glaucoma, uveitis, and retinal disorders; (7) use of contact lenses; (8) any situation affecting the measurement results, such as poor topography images due to corneal disorders or unstable fixation; (9) inability to comply with the topography examination; (10) active ocular infection (conjunctivitis, keratitis); (11) use of any topical eye drops; (12) mental disability; (13) systemic disorders such as hypertension or diabetes mellitus, cardiovascular disease, and respiratory disease; and (14) systemic drug use.
All participants underwent a thorough ophthalmic examination, including refraction and BCVA, slit lamp biomicroscopy, IOP as measured by Goldmann tonometry, and fundus examination. An autorefractor (TOPCON KR-8900; Topcon Corporation, Tokyo, Japan) was used to measure refractive error. SE values were calculated as spherical + 1/2 cylindrical.
Scheimpflug-based corneal topography (Sirius; Costruzione Strumenti Oftalmici, Florence, Italy) was used to evaluate the anterior segment parameters by the same ophthalmologist (SC) with participants in a resting position. Corneal topography measurements were performed consecutively for each eye. Participants were situated with a head and chin rest and asked to stare at an internal fixation point. They were told to blink three times before the corneal topography images were taken. Corneal images were taken within 1–3 s of blinking. If acquisition quality of >90% or better was detected, the topography images were saved. At the same time, pupillography was performed.
For each participant, a drop of 1% cyclopentolate hydrochloride (Sikloplejin; Abdi Ibrahim, Istanbul, Turkey) was instilled in the right eye and a drop of 1% tropicamide (Tropamid; Bilim, Istanbul, Turkey) was instilled in the left eye three times at 10 min intervals. The examiner masked to instilled drops in each eye. To minimize the systemic absorption of the drugs, participants pressed on their inner canthus for about 3 min after each instillation. When it was seen that light reflex was not taken, it was decided to complete the process. Before and 40 min after the last drop, refractive error, IOP, pupillography, and corneal topography measurements were obtained.
Pre-dilatation and post-dilatation measurements were compared. Changes in anterior segment values were defined as Δ.
Statistical analysis
IBM SPSS Statistics 22 (IBM Corp., Armonk, NY, USA) was used in all statistical analyses. In the evaluation of the compliance of data with normal distribution, the Kolmogorov-Smirnov test was used. Values from groups that complied with normal distribution were evaluated with the paired samples t-test, and values that did not comply with normal distribution were evaluated with the Wilcoxon test. Differences between measurements were evaluated with independent t-tests and Mann–Whitney U tests between groups. Values of p < 0.05 were accepted as statistically significant.
Results
In this study, 120 eyes of 60 healthy participants were included. Cyclopentolate drops were applied to the right eyes (Group 1) and tropicamide drops were applied to the left eyes (Group 2). The mean age of the participants was 34.1 ± 9.1 years (range: 20–50 years). Twenty-nine participants were female (48.3%) and 31 were male (51.7%).
Tables 1 and 2 show the average SE, keratometric (K1 and K2), central corneal thickness (CCT), aqueous depth (AD), anterior chamber depth (ACD), ACV, iridocorneal angle (ICA), and PS values before and after the instillation of drops in Groups 1 and 2, respectively. In Group 1, SE, AD, ACD, ICA, ACV, and PS values were significantly increased with instillation (p < 0.001, p = 0.03, p = 0.01, p < 0.001, p < 0.001, and p < 0.001, respectively). In Group 2, SE, ICA, ACV, and PS values were significantly increased with instillation (p < 0.001, p < 0.001, p < 0.001swqx, and p < 0.001, respectively).
Anterior segment parameters of Group 1 before and after drop instillation.

ACV, Anterior chamber volume; AD, Aqueous depth; CCT, Central corneal thickness; D: diopter; K1, Flat keratometry value, K2, Steep keratometry value, SE, Spherical equivalent; Km, Mean keratometry value, ICA: Iridocorneal angle; PS: Pupil size.
p < 0.05.
Wilcoxon test.
Paired t-test.
Anterior segment parameters of Group 2 before and after drop instillation.
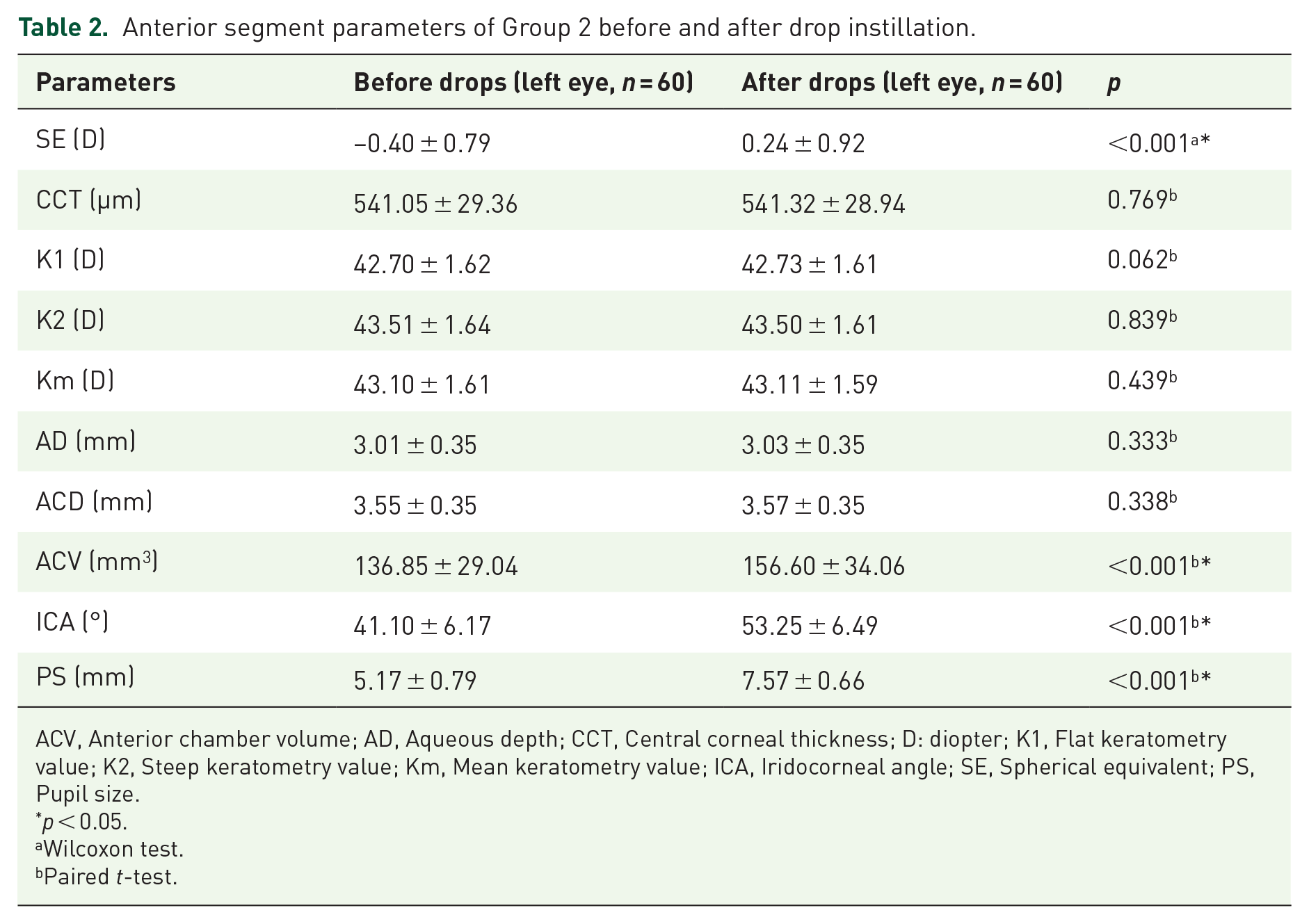
ACV, Anterior chamber volume; AD, Aqueous depth; CCT, Central corneal thickness; D: diopter; K1, Flat keratometry value; K2, Steep keratometry value; Km, Mean keratometry value; ICA, Iridocorneal angle; SE, Spherical equivalent; PS, Pupil size.
p < 0.05.
Wilcoxon test.
Paired t-test.
There was no statistically significant difference (Δ) between the agents in terms of changes in anterior segment parameters. A comparison of the parameters is given in Table 3.
Change in anterior segment values of Groups 1 and 2 before and after drop instillation.

ACV, Anterior chamber volume; AD, Aqueous depth; CCT, Central corneal thickness; D, diopter; ICA, Iridocorneal angle; K1, Flat keratometry value; K2, Steep keratometry value; Km, Mean keratometry value; PS, Pupil size; SE, Spherical equivalent.
p < 0.05.
Mann–Whitney U test.
Independent t-test.
We also investigated the changes on ocular parameters of these drops based on age and sex. We found that changes in Pupil Distance (PS) with cyclopentolate in males (−2.72 ± 0.77 mm) were significantly greater that females (−2.26 ± 0.70 mm) (p = 0.019). Eyes with tropicamide, there was no significant changes in all parameters between males and females (p > 0.05). In addition, we divided the patients into three groups according to their age; group 1 = 20–30 years, group 2 = 31–40 years, group 3 = 41–50 years. Eyes with cyclopentolate, ACV and PD values were significantly different between group 1 and 2, and group 2 and 3 (post hoc analysis; p = 0.007 and p = 0.022, respectively). Eyes with tropicamide, ACV value was significantly different between group 1 and 3 (post-hoc analysis; p = 0.013).
Discussion
The main goal of the current study was to evaluate and compare the effects of 1% cyclopentolate and 1% tropicamide on SE, K1, K2, CCT, AD, ACD, ACV, ICA, and PS values.
In this study, statistically significant differences in SE values were obtained with both cyclopentolate and tropicamide after instillation. In terms of SE, however, there was not a significant difference between the groups (p = 0.71). There were similarly no significant differences between the groups in terms of ΔCCT, ΔK1, ΔK2, and ΔKm. While AD and ACD increased significantly in the cyclopentolate group, there was no significant difference in the tropicamide group. The difference in AD (ΔAD values) was not significant between the groups. In terms of ACV, ICA, and PS, there were statistically significant changes in both groups. However, the two administered agents had similar effects on ACV, ICA, and PS values. On the other hand, two participants had ocular side effects including conjunctival hyperemia with cyclopentolate instillation and no systemic side effects were not observed in any participants.
Refraction changes with cycloplegic drops were reported with hypermetropic shifts in related studies. For example, Bagheri et al. used 1% cyclopentolate and found an average hypermetropic shift of 0.4 ± 0.5 D in their study with 106 subjects (average age: 28 years). 16 Hiraoka et al. used 1% atropine and showed a hypermetropic shift of approximately 1 D in their study. 17 In the study of Krantz et al., which included individuals aged between 22 and 39 years, they found 4.4 D changes in SE with 1% tropicamide. 18 In a study of 7793 young adults, Sun et al. found an average difference of 0.83 D in SE before and after 1% cyclopentolate instillation. 19 In addition, there are some studies that investigated the association between iris/skin pigmentation and effect of cycloplegia. Minderhout et al. reported that skin pigmentation rather than iris pigmentation is the decisive factor for effectiveness of cycloplegics. 20 Bahar et al. reported that change in spherical refraction and pupil diameter for different eye colors revealed a significant difference in these measurements in blue eyes after pilocarpine administration. 21 Eye color may affect the pharmacodynamics of other drugs. In our study, in general the color of the eyes were brown. In the current study, an average hypermetropic shift of 0.80 D was seen in the cyclopentolate group and hypermetropic shift of 0.64 D was seen in the tropicamide group. These differences can be explained by the ages of the participants, the potency of the cycloplegic agents, and a possible excess of participants with hypermetropia. This variation in adults confirms that cycloplegic examinations should be performed for patients, especially for efforts to correct refractive disorders and in evaluations before refractive surgery. The current study differed from previous studies with the instillation of two agents for the same participants. This method allowed us to more objectively evaluate the effects of the agents by eliminating individual response differences. We believe that our findings will contribute to the literature by showing the effects of these agents in the same patient group.
In the present study, there was no significant difference in CCT or K values obtained before and after instillation of the cycloplegic drops. The previous study most similar to ours in terms of study design was conducted by Tasci et al. 22 They compared 1% cyclopentolate and 0.5% tropicamide and they found a significant increase in CCT values in the cyclopentolate group. However, they did not find any changes in the tropicamide group. They explained the increase in CCT values as being due to the deterioration of the epithelium. 23 They further stated that there was a difference of approximately 2 µm in the cyclopentolate group, which was not clinically significant. Parallel to our findings, they reported no significant differences in K1, K2, CCT, ACD, and PS values between the agents. We think that the findings of the present study are more reliable than those of Tasci et al. because in the current study Sirius Scheimpflug-based corneal topography was applied, and the device used here was found to be superior to the Lenstar LS 900 optical biometer in terms of keratometric measurements. 24 At the same time, the two agents were both instilled for all patients and structural and genetic factors that could alter the effects of the agents were thus controlled. Therefore, the effects of these two agents were compared in the present study under the most optimal conditions. Another similar study was conducted by Palamar et al., who investigated the effects of 1% tropicamide on anterior segment parameters using Pentacam topography. 25 Similar to our findings, they reported that tropicamide did not affect the keratometric values or CCT while it increased the ACD, ACV, and PS values. The current study’s population was larger than that of Palamar et al. In addition, the effects of 1% cyclopentolate on these parameters were also investigated in the present study.
Similar to the current study, Ariolla-Villalobos et al. did not find any significant changes in CCT after cycloplegia with 1% tropicamide. 26 In relation to keratometry values, Bagheri et al. did not find any significant changes in mean total and anterior corneal power after dilatation. 16 Megwas et al. studied 42 emmetropic, 54 myopic, and 28 hypermetropic patients. They showed no significant changes in corneal curvature in measurements taken 30, 60, and 90 min after instillation of 1% cyclopentolate hydrochloride. 27 Ozcaliskan et al. found that there was no difference after dilatation in K1 and K2 values upon instillation of 1% cyclopentolate. 1 The results of the current study are consistent with those presented in the literature. It can be said that the cornea, which contributes approximately two-thirds of the refractive power of the eye, does not change with cycloplegia. These results show us that clinicians can safely use third-generation IOL formulas after dilation with both 1% cyclopentolate and 1% tropicamide.
In the literature, many studies reported increases in AD, ACD, and ACV values after dilatation.9,22,25,28,29 These changes were attributed to the effect of accommodation and the flattening and backward movement of the lens. 30 In the present study, a significant increase was found for ACV in both groups (approximately 20 mm3). Although AD and ACD increased significantly in the cyclopentolate group, changes were not significant in the tropicamide group. This may be due to the weaker effect of tropicamide compared to cyclopentolate. However, when evaluated in terms of their ability to change AD and ACD values, no difference was found between cyclopentolate and tropicamide.31,32
Studies in the literature on ICA are contradictory. Many studies found a decrease after dilatation.2,9,29 On the contrary, some studies reported increased ICA values.33–35 In our study, ICA was increased significantly with both cyclopentolate and tropicamide instillation. In the evaluation of the ability to affect ICA values, no difference was found between cyclopentolate and tropicamide. The reason for these differences among studies may be the differences in the instruments used for measurements or the different age distributions of the participating patients and different ethnicities. In our study, PS values increased in both groups and there was no difference in the change in PS between the agents. Due to the posterior movement of the iris lens diaphragm, the ACD has increased and therefore the ICA has increased despite PS values increased in both groups.
It should be kept in mind that fourth-generation formulas (Hoffer Q, Haigis) may have other effects in the calculation of IOL due to changes in the anterior segment after dilatation. In mandatory cases, it can be considered that drops containing tropicamide will affect these parameters similarly or less, and they can be used instead of cyclopentolate drops.
The present study has some limitations. First, the study population was relatively small. Second, the age range of the participants (20–50 years) encompassed only young adults and adults. Since the main purpose of this study was to investigate the effects of these agents in healthy individuals with fully developed eyes, patients in this age group were included in the study. We think that such a study in the pediatric study group can provide valuable information. Further studies are needed to determine the effects of these agents on children and the elderly. Third, individuals with high refractive errors were not included in this study. It is still necessary to investigate how these agents affect that patient population. Last, this study did not include myopic and hyperopic participants and it is possible to compare the findings of cycloplegia with further studies achieved with both drops for myopic SE and hyperopic SE.
Conclusion
The present study is important in that it examines the effects of two different agents with the same concentrations in the same participants, allowing us to compare the effects of these two agents. It was found that both cycloplegic agents (1% cyclopentolate and 1% tropicamide) significantly affected SE, ACV, ICA, and PS values. However, there was no significant change in CCT or K values. For AD and ACD, while there was a significant change in the cyclopentolate group, there was no significant change in the tropicamide group. We can conclude that tropicamide has similar effects to those of cyclopentolate, although it is weaker. When making decisions in cases of phakic IOL and refractive surgery, it is useful to consider these changes in determining the formulas to be used in IOL calculations.