
Abstract
Background:
Topical immunosuppressants such as tacrolimus in different concentrations are a breakthrough in the management of recalcitrant vernal keratoconjunctivitis (VKC); however, there is a lacks of comparative studies to guide their use in VKC management.
Objective:
To compare the efficacy and safety of tacrolimus 0.03% and 0.1% eye ointment in the treatment of recalcitrant VKC.
Design:
A retrospective comparative single-centre observational study.
Method:
We reviewed records of a total of 48 recalcitrant VKC patients treated with two different strengths of tacrolimus ointment between April 2016 and March 2017. Of these, 39 fulfilled the inclusion criteria and were categorized into two groups, A and B, depending on the use of strength of tacrolimus (0.03% and 0.1%) used, respectively. Group A had 18 patients, while group B had 21 patients. Thirty-six patients, 18 from each group, were finally analysed and compared. Records of patients were explored for the subjective symptoms and objective sign score of the patient at baseline and at each time point. The main outcome measures were composite scoring and comparison of total subjective symptom scores (TSSSs) and total objective sign scores (TOSSs) within and between the groups at each follow-up. Percentage of patient with significant reduction in symptom and sign scores as compared with baseline was considered success of treatment. Chi-square and t-tests were used for comparison of outcomes between both groups
Results:
Mixed variety was most commonly encountered type of VKC. The signs and symptoms were significantly reduced in patients with treatment in both groups (p = 0.001) in all types of VKC. However, in group B, there was significant improvement in the size of papillae (p = 0.04) as compared baseline in contrast to group A. Side effects like burning and stinging in group B were significantly higher as compared with group A.
Conclusions:
Both strengths of tacrolimus (0.03% and 0.1%) are effective in all forms of recalcitrant VKC. Papillary component of VKC responds better with higher strength (0.1%) but is associated with more significant side effects. Different strengths of tacrolimus can be used strategically depending upon the severity and clinical type of VKC to intensify outcome and minimize side effects.
Introduction
Vernal keratoconjunctivitis (VKC) or spring catarrh is a recurrent, bilateral, chronic ocular inflammatory condition of ocular surface that primarily affects boys living in warm and dry climate in their first two decades of life.1,2 It is an allergic condition with complex interplay between the humoral and cell-mediated immune mechanisms .3,4 Family history of atopy is a common association in most of these patients. 4 Patients with VKC present with a typical set of complaints comprising intense itching, watering, burning sensation, ropy discharge and a red eye. Typical conjunctival signs consist of hyperaemia, giant papillae on superior palpebral conjunctiva, papillary hypertrophy or Horner–Trantas dots that consist of accumulation of gelatinous inflammatory infiltrates around the limbus. 5 The disease may sometime lead to corneal involvement in form of superficial keratitis, shield ulcer or corneal vascularization that causes foreign body sensation, pain and photophobia 6 Although, VKC is a self-limiting disorder resolving around puberty, the characteristic episodes of exacerbation and remission of the inflammatory phase of the disease is generally bothersome. 6 Besides increased risk of vision-threatening complications, the quality of life gets severely compromised. 7 The treatment options of VKC usually include anti-histamines, mast cell stabilizers and non-steroidal anti-inflammatory offered in different permutations and combinations. 8 Moderate to severe sight-threatening cases frequently need topical steroids, or but being chronic disease, long-term use of steroids has notable side effects like glaucoma, cataract and secondary infections. 9 To prevent such complications, steroid-sparing agents like immunosuppressants are a better alternative. 10 They not only inhibit histamine release from mast cell and basophils but also block proliferation of Th2 lymphocyte and subsequent interleukin-2 production.10,11 Two members evaluated in this category are tacrolimus and cyclosporine with encouraging results.12,13 Potency of tacrolimus is reported to be 100 times more than cyclosporine-A. For this reason, it has been useful even in cases refractory to cyclosporine.13,14 Besides being used in steroid resistant, it has even been used as first line therapy in VKC.15,16 Strength of topical tacrolimus being used in clinical practice for the treatment of VKC ranges from 0.005% to 0.1%.17,18 Different studies evaluating its efficacy have used different preparations and strengths of tacrolimus. But till date, to the best of our knowledge, none of the study has compared and evaluated the different formulations or strength of tacrolimus. There is no guideline available regarding the ideal or optimal dose of topical tacrolimus. So, in this study, we have tried to comparatively evaluate efficacy and safety of two different strengths of tacrolimus (0.03% and 0.1%) eye ointment as treatment for recalcitrant VKC.
Materials and methods
A retrospective comparative observational study was designed in accordance to the tenets of the Declaration of Helsinki at a tertiary eye care centre of east India. Case records of patients with recalcitrant VKC who had undergone treatment with two different strength of tacrolimus ointment (Talimus LS or Talimus, Ajanta Pharma, India) between April 2016 and March 2017 were reviewed. All these patients have had previous treatment with either topical corticosteroids or cyclosporine eye drops for at least 4–6 weeks. Steroid therapy ranged from topical therapy with soft steroids like fluorometholone, loteprednol, rimexolone, to potent steroids like prednisolone or dexamethasone. There was no history of supratarsal injections or oral steroids. Topical cyclosporine had been used in strength from 0.05% to 2%. The demographic and clinical data of patients were retrieved from their medical records. Diagnosis of recalcitrant VKC was made clinically according to the presence of active disease with classical signs and symptoms not responding to conventional treatment. Records of clinical scoring of classical signs (conjunctival hyperaemia, conjunctival papillae, Trantas dots, punctate keratitis and limbal infiltration) and symptoms (itching, tearing, photophobia, discharge and foreign body sensation) as suggested by of Bleik and Tabbara, 19 (Table 1) were noted where each variable was graded on a scale of 0–3 depending upon increasing severity. A composite score was calculated by adding the grades to record get a record of total subjective symptom score (TSSS) and total objective sign score (TOSS). 19 Since VKC is a bilateral disease, the worse eye with the higher total symptom and sign score at baseline was selected for comparison of signs in case of asymmetric severity at presentation. In case, the severity was same in both eyes, the right eye was chosen.
Grading of signs and symptoms (Bleik and Tabbara 19 ).

Presence of co-existing ocular diseases, such as glaucoma, uveitis, corneal disease, contact lens users, ocular infection, systemic illness like hepatic or renal dysfunction and any reported hypersensitivity to any drugs or immunosuppressants formed the basis for exclusion from the review.
Records of patients were analysed for their TSSS and TOSS at each time point and compared with baseline. The primary outcome was measured in terms of TSSS and TOSS before and after treatment at each visit. Secondary outcomes included scoring of transient side effects of medications and any recurrence of symptoms and signs after treatment completion. Transient ocular discomfort from drugs, such as burning, blurring, stinging, ocular pain, periorbital oedema, periorbital rash and headache were graded from 0 to 3 depending upon increasing severity was noted from the medical records.
Statistical analysis
All data were analysed with the statistical package for social sciences (SPSS). Continuous variables are presented as mean ± standard deviations (SDs) and the categorical variables as percentages. Student’s t-tests were used to determine the significance of the differences between means in the variables that were normally distributed. The Wilcoxon signed-rank tests were used for paired samples when the data were not normally distributed. Comparison of TSSS, TOSS and side effect scores between and within groups at different time points (at entry, weeks 2, 4, 6, 8, 10 and 12) was performed by analysis of variance (ANOVA) with repeated-measure analysis and with Bonferroni corrections. The p-value < 0.05 was considered to be statistically significant.
Results
Record of a total of 48 recalcitrant VKC patients treated with tacrolimus during the time period (April 2016–March 2017) was identified. Of these, 39 of them were eligible of inclusion and had complete data of fortnightly follow-up till 12 weeks. Demographic history revealed that most of the patients lost to follow-up were from remote area and majority of them attended one or two follow-ups randomly, and hence were marked ineligible for inclusion in the study. Eligible patients were categorized into two groups, A and B, depending on the use of strength of tacrolimus (0.03% and 0.1%) used, respectively. Group A had 18 patients, while group B had 21 patients, of which 18 were randomly selected for comparative analysis (Table 2).
Baseline characteristics of the two groups.

CI, confidence interval; SD, standard deviation; VKC, vernal keratoconjunctivitis.
significant if <0.05.
Of the 36 patients, 31 (86.11%) were male with a mean age of 8.36 (± 1.14) years in group A and 7.125 (± 1.66) years in group B, the difference between the two being statistically insignificant (p = 0.15) (Table 2). Median duration of disease in months was 8.25 and 6.56 in the two groups, respectively.
Mixed variety was the most common form of presentation (n = 21) followed by tarsal type VKC (n = 10) and limbal variant (n = 5) (Table 2) in both groups. Allergic rhinitis was the most common systemic association in either group.
TSSS with 95% confidence interval (CI) at baseline in group A was 7.06 (5.68–8.44), while in group B, it was 7.65 (6.19–9.36). Similarly, TOSS were 4.875 (4.07–5.67) and 4.523 (3.88–5.11) in the two groups, respectively, the difference was clinically insignificant. There was a consistent decrease in TSSS with treatment in both the groups till 8 weeks. The difference was significant as compared with baseline at 6 weeks with 0.1% strength while with 0.03% strength, significant difference from baseline was noticed at 8 weeks (Figure 1).

Total subjective symptom score (TSSS) at different visits.
A consistent decrease in TOSS also was noticed in both the groups and the difference as compared with baseline was significant at 8 weeks in both the groups (Figure 2). Among the signs, there was consistent decrease in the size of the papillae in both the groups as compared with base line but the difference was clinically significant in group B (p = 0.04) (Figure 3). Withdrawal of medication resulted into increase in both TSSS and TOSS in the two groups at 10 and 12 weeks, respectively, without any significant differences in between the groups.

Total objective sign score (TOSS) at different visits.
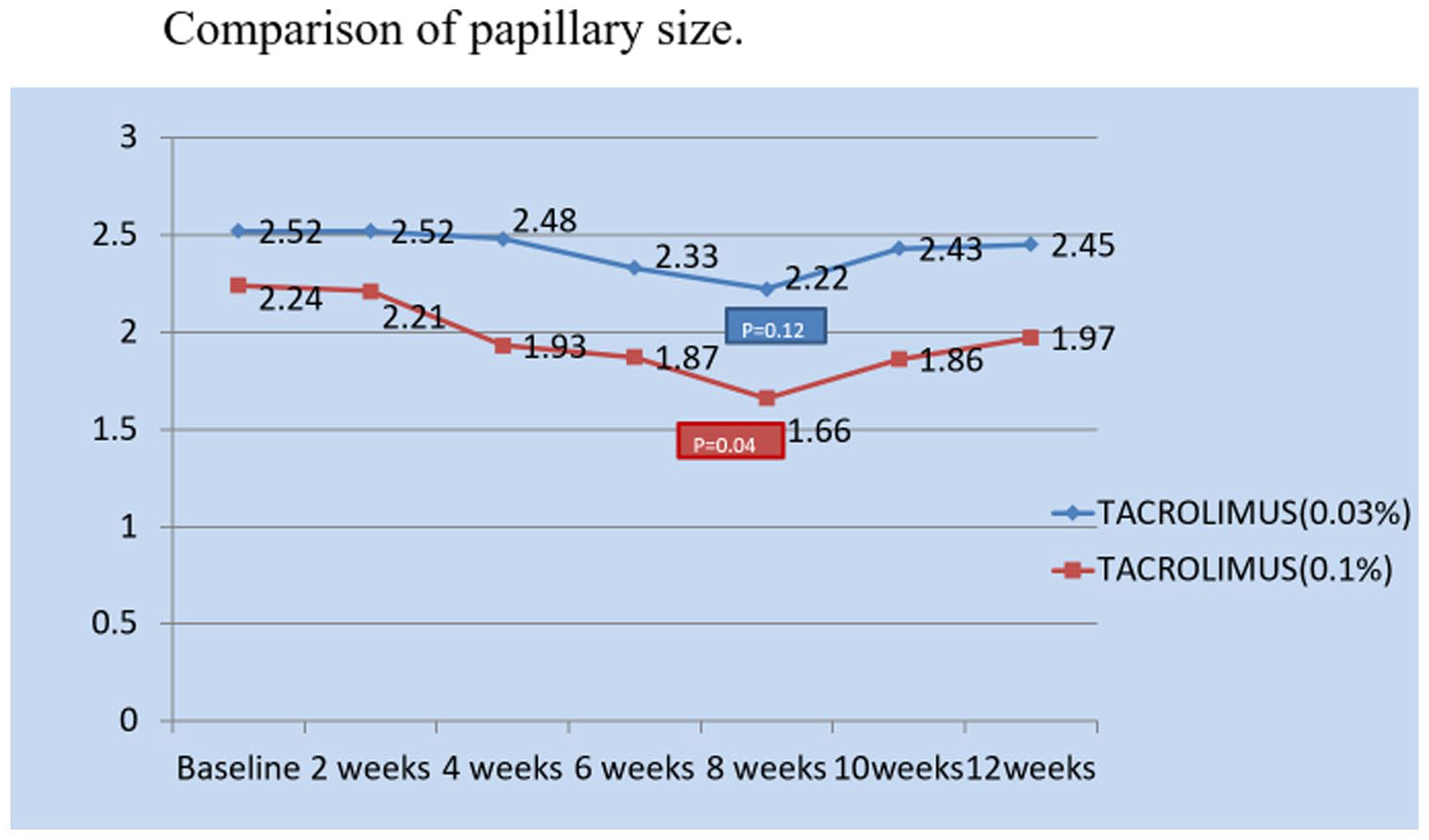
Effect on papillae at different visits.
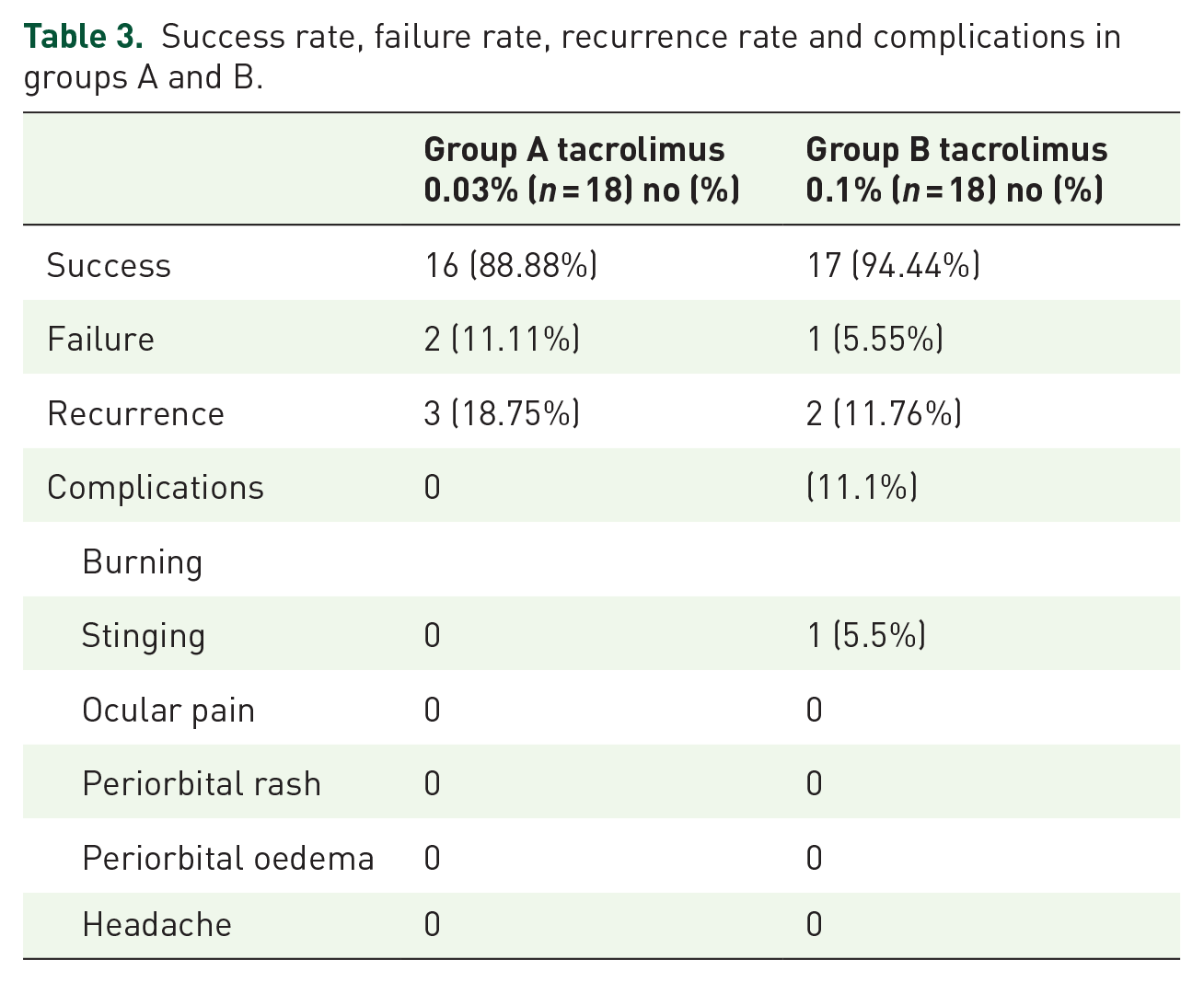
The success rate of treatment of groups A and B was 88.88% and 94.44%, respectively. During the treatment period, side effects like stinging and burning sensations, were present in three (16.67%) patients in group B, while no such complication was observed in group A (Table 3).
Success rate, failure rate, recurrence rate and complications in groups A and B.
Discussion
VKC is a potentially vision-threatening inflammatory disease of cornea and conjunctiva. It usually affects during the first two decades of life with male preponderance as noticed in our study too. 20 Depending upon the area involved, it can be of tarsal, limbal or mixed variety. Our study found mixed variety to be the most common type that is consistent with the findings of Khan et al. 21 and Saboo et al. 22 However, there are studies in favour of the other two varieties as the most commonly encountered one. 23 This signifies prevalence of different subtypes in various parts of the world.
Tacrolimus, a calcineurin inhibitor, leads to marked suppression of various cytokines produced by the activated T cell, hence curtails the mechanism playing major role in the pathogenesis of VKC. Besides the activated T cells, activated eosinophils too release cytokines, chemokines, leukotrienes and epitheliotoxic proteins responsible for ocular surface inflammation and corneal epithelial damage. 24 Tacrolimus inhibits eosinophil chemotaxis thereby reduces recruitment of inflammatory cells on the ocular surface. 18 Hence, tacrolimus seems to an effective agent in VKC. In the past decade, several studies have evaluated tacrolimus in steroid-resistant or refractory VKC or as a steroid sparing with good results. Different strengths or formulations of the drug were used in different studies 25
In our study, 88.88% of the patients receiving 0.03% tacrolimus, and 94.44% of those under treatment with 0.1% tacrolimus, had significant improvement in the severity of their symptoms. This implies that both strengths of tacrolimus are effective options for children with VKC. Although the rate of resolution was faster in group B as compared with group A, but again the difference was not statistically different. Of the five symptoms, itching was the first symptom to respond in both the groups. Among the signs, papillary component responded better with higher strength (0.1%) of tacrolimus as compared with lower strength (0.03%). Similar response on conjunctival papillae was noticed by Shoughy et al. 26 even with concentration of 0.01%. Most probably, response of conjunctival papillae depends directly upon the strength of tacrolimus used. Tacrolimus has been documented safe for long-term use. However, there are reports of complications like stinging, burning, watering, ocular pain or sometimes herpetic keratitis. 27 Our study found only mild burning and stinging sensation in three patients of group B and it did not let any patient to drop out of the treatment. At the same time, there was no such complication noticed in group A. From the observations of this study, we recommend to use higher strength, 0.1%, in cases of palpebral VKC that can gradually be shifted to lower strength in due course to minimize burning and stinging sensation. Other varieties of VKC can be dealt with lower concentration with equal efficacy.
However, small sample size and short follow-up are the major limitations of this study. Moreover, this is a retrospective observational study. For more robust conclusions, we some randomized control trials with large sample size and longer follow-up. These studies can help us stratify the use of different strengths of tacrolimus based on severity and clinical type of VKC to maximize its benefits, minimize recurrences while curtailing its side effects on long-term use.
Conclusion
Both strengths of tacrolimus (0.03% and 0.1%) seem to be equally efficient at all forms of recalcitrant VKC, except in palpebral variety, where 0.1% was more effective but had comparatively more side effects.