
Abstract
Background:
Ocular biometry and anterior segment evaluations are important to determine ocular development and pathological changes, especially in thalassemia patients in Mediterranean countries such as Turkey.
Objectives:
The objectives of this study were to compare ocular biometry and anterior segment parameters in children with thalassemia major and healthy controls and to examine the relationship between ferritin levels, anthropometric measurements, and ocular parameters.
Design:
This is a prospective case-control study.
Methods:
The height, weight, body mass index, and occipitofrontal circumference values of the participants were recorded. Anterior and vitreous chamber depth, lens thickness, axial length, central corneal thickness, anterior chamber volume, iridocorneal angle, pupil diameter, and mean keratometry were measured. Measurements were compared between patients and healthy children, and between patients with ferritin levels above and below 1000 ng/mL.
Results:
This study included 40 patients and 45 controls. Height, weight, and body mass index were significantly lower while ferritin level and occipitofrontal circumference were significantly higher in patients compared with the controls (p < 0.001 for all). There were no statistically significant differences in the other ocular parameters (p > 0.05). In comparisons between patients with ferritin levels below (n = 15) and above 1000 ng/mL (n = 25), there were no significant differences in age, height, weight, body mass index, occipitofrontal circumference, or ocular parameters (p > 0.05). Occipitofrontal circumference and mean keratometry value were positively correlated in patients with ferritin levels below 1000 ng/mL (r = 0.573, p = 0.025), while body mass index was negatively correlated with pupil diameter in patients with ferritin levels above 1000 ng/mL (r = −0.469, p = 0.018).
Conclusion:
Children with thalassemia showed significant growth retardation and large occipitofrontal circumference but did not differ from controls in terms of biometrics and anterior segment morphology. Our results demonstrated a positive correlation between the occipitofrontal circumference and mean keratometry value in children with ferritin levels below 1000 ng/mL and a negative correlation between body mass index and pupil diameter in children with ferritin levels above 1000 ng/mL.
Introduction
Thalassemia occurs as a result of a genetic defect in amino acid biosynthesis of the globin chain of hemoglobin and shows autosomal recessive inheritance. It is one of the most common genetic diseases in the world. There are 80–90 million carriers, representing approximately 1.5% of the global population. 1
Patients with beta thalassemia major (TM) have impaired β-globin chain synthesis. 2 Despite the rapid activation of bone marrow cells, patients are anemic due to ineffective erythropoiesis and premature destruction of produced erythrocytes. Transfusion reduces bone marrow hyperactivity and protects against chronic hypoxia. Iron chelators are used to remove the excess iron that accumulates after multiple transfusions. Pronounced cranial abnormalities occur as a result of medullary expansion against the bone secondary to increased hematopoietic tissue activity. Patients develop a typical thalassemia facies involving prominence of the bones in the maxillary region, depression of the nasal bridge, and frontal bossing. Growth retardation also occurs as a result of premature epiphyseal fusion in long bones such as the humerus and femur. 3
Both the disease itself and its treatment can lead to various ocular problems, which are reported in between 10.5% and 74% of thalassemia patients. 4 This difference in rates can be attributed to the analyzed parameters, patient age groups, treatment methods, transfusion frequency, and the type and dose of iron chelator agents. 4 Some of the ocular problems seen in TM patients receiving chelation therapy include retinopathy, lens opacification, color vision loss, depressed visual field, reduced visual acuity and contrast sensitivity, nyctalopia, and abnormal electrophysiological test results. 4 Numerous studies have indicated that these problems are caused by various underlying factors such as anemia, iron overload, chelation therapy, and orbital bone marrow expansion. 5
In this study, we aimed to compare ocular biometry and anterior segment parameters between children with TM and healthy controls and to examine the relationship between serum ferritin level and anthropometric and ocular parameters in TM patients receiving chelator therapy.
Methods
The study included 40 patients who were between 8 and 18 years and followed up regularly in the pediatric hematology clinic of Adana City Training and Research Hospital between March 2021 and September 2021 and 45 healthy age- and sex-matched children who presented to the ophthalmology clinic for routine check-up. The study size of the patients was calculated with power analysis. As a result of the G-Power analysis (95% confidence, 80% test power, and d = 0.5 effect size), a total of 85 participants were included in the study.
All children in the TM group were receiving blood transfusion and iron-chelating agents. Inclusion criteria for both groups were being 8–18 years of age and having adequate fixation and ocular media clarity to enable the acquisition of high-quality Pentacam images. Exclusion criteria were any systemic disease other than TM, presence of covid 19 infection, best corrected visual acuity (BCVA) worse than 20/25, amblyopia, glaucoma, keratoconus, history of any ocular trauma or surgery, and contact lens use.
The height, weight, body mass index (BMI), occipitofrontal circumference (OFC), and serum ferritin levels of all participants were recorded. BCVA measurement with Snellen chart, slit-lamp anterior segment and dilated fundus examinations, intraocular pressure (IOP) measurement by Goldmann applanation tonometry, keratometry, biometry, and corneal topography measurements were performed. IOP and biometric measurements were obtained at the same time of day (9:00–12:00) to minimize diurnal variation. In addition, all measurements were made by the same technician for each instrument. Mean keratometry (Kmean) was determined using an auto kerato-refractometer.
Contact A-scan ultrasound (Aviso, Quantel Médical, Clermont-Ferrand, France) was used to measure anterior chamber depth (ACD), vitreous chamber depth (VCD), lens thickness (LT), and axial length (AL). A drop of topical benoxinate 0.5% was instilled for topical anesthesia before measurement. The average of five measurements with a standard deviation less than 0.1 was obtained for each eye.
Anterior segment parameters were evaluated using a Scheimpflug imaging system (Pentacam, Oculus Optikgerate, Wetzlar, Germany). Pentacam measurements were obtained without mydriasis in a darkened room using the instrument’s automatic acquisition mode to exclude user-dependent variables and standardize measurements for all patients. Three measurements were performed for each participant and the measurement with the best quality was included in the analysis. Central corneal thickness (CCT), anterior chamber volume (ACV), iridocorneal angle (ICA), and pupil diameter (PD) were measured in all participants. Data from the right eyes were compared between the TM and control groups and between TM patients with ferritin levels above and below 1000 ng/mL.
Statistical analysis
Continuous variables were tested for normal distribution using the Shapiro–Wilk test. Student’s t test was used to compare normally distributed variables, and Mann–Whitney U test was used to compare non-normally distributed variables between groups. Spearman’s rho correlation coefficient was calculated to examine the linear relationships between height, head circumference, ferritin, and the other variables. Sex distribution in the groups was compared using chi-square test. SPSS version 21.0 software was used to analyze the data. The statistical significance level was accepted as 0.05.
Results
In total, 85 participants were included in this study. Of these participants, 40 were TM group (14 girls, 26 boys) while 45 (15 girls, 30 boys) were healthy group. There was no significant difference between TM and control groups in terms of age (range, 8–18 years) or sex distribution (p = 0.224 and p = 0.871, respectively). Girls comprised 35% of the TM patient group (n = 14) and 33.3% (n = 15) of the control group.
BCVA assessed with Snellen chart was 20/20 in both groups. Mean intraocular pressure was 13.2 ± 1.95 mmHg in the TM group and 13.33 ± 1.67 mmHg in the control group (p = 0.765).
Height, weight, and BMI were significantly lower in the TM group compared with the control group, while ferritin level and OFC were significantly higher (p < 0.001 for all) (Table 1).
General characteristics and ferritin levels.

BMI, body mass index; OFC, occipitofrontal circumference; SD, standard deviation.
p: Student’s t test *Mann–Whitney U test.
Comparison of Kmean, ACD, VCD, LT, AL, CCT, ACV, ICA, and PD measurements between the two groups revealed no statistically significant differences (p > 0.05) (Table 2).
Ocular biometry and anterior segment parameters.

ACD, anterior chamber depth; ACV, anterior chamber volume; AL, axial length; CCT, central corneal thickness; ICA, iridocorneal angle; Kmean, mean keratometry; LT, lens thickness; PD, pupil diameter; SD, standard deviation; VCD, vitreous chamber depth.
p: Student’s t test *Mann–Whitney U test.
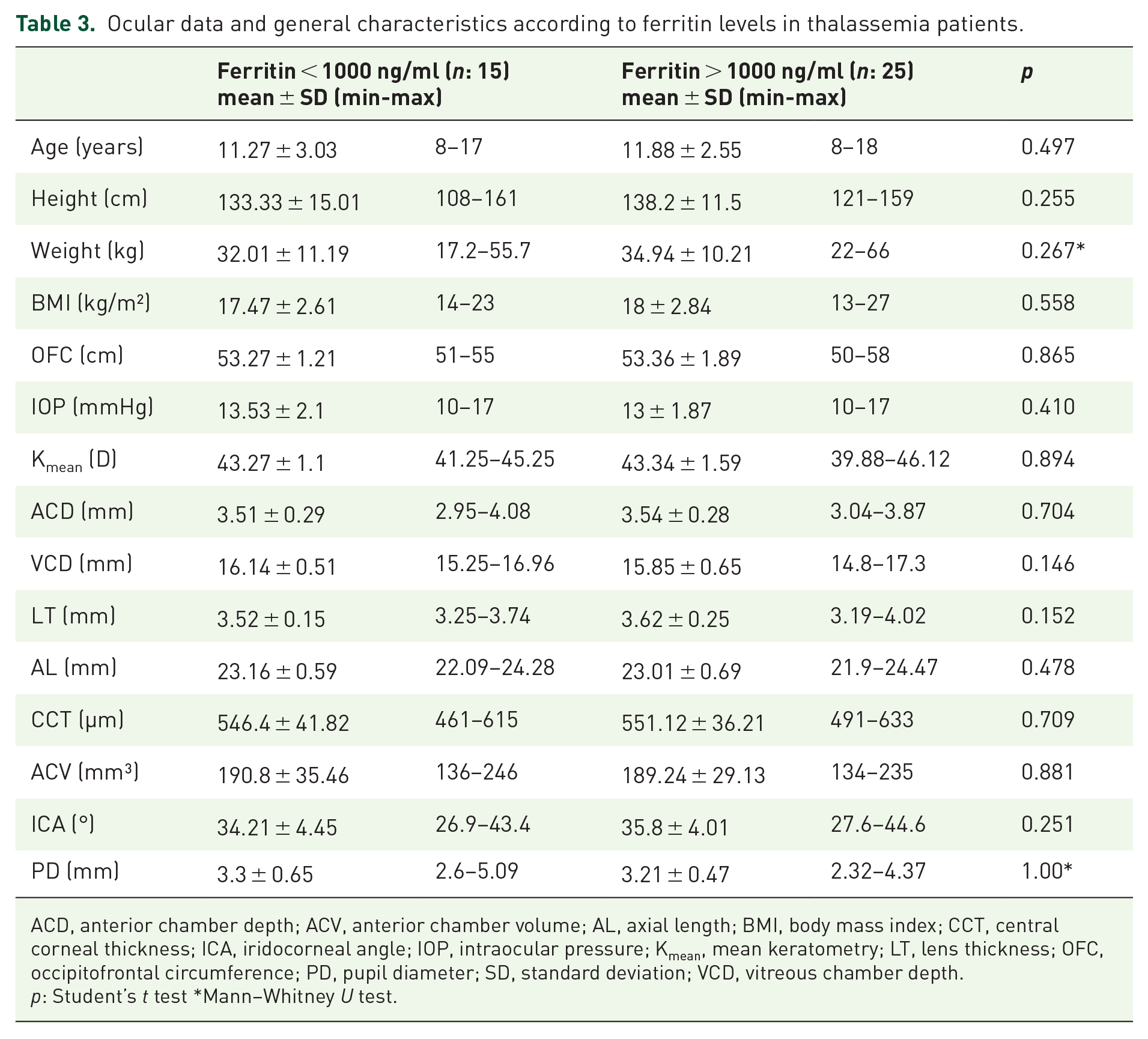
When TM patients were grouped according to ferritin level, there were no significant differences in age, height, weight, BMI, OFC, or ocular parameters between those with ferritin levels below 1000 ng/mL (n = 15) and above 1000 ng/mL (n = 25) (p > 0.05) (Table 3).
Ocular data and general characteristics according to ferritin levels in thalassemia patients.
ACD, anterior chamber depth; ACV, anterior chamber volume; AL, axial length; BMI, body mass index; CCT, central corneal thickness; ICA, iridocorneal angle; IOP, intraocular pressure; Kmean, mean keratometry; LT, lens thickness; OFC, occipitofrontal circumference; PD, pupil diameter; SD, standard deviation; VCD, vitreous chamber depth.
p: Student’s t test *Mann–Whitney U test.
In correlation analysis between height, BMI, and OFC values and ocular parameters in TM patients grouped according to ferritin levels (Table 4), a significant positive correlation was detected between OFC and Kmean in patients with ferritin levels below 1000 ng/mL (r = 0.573, p = 0.025) (Figure 1). In addition, there was a significant negative correlation between BMI and PD in patients with ferritin levels above 1000 ng/mL (r = −0.469, p = 0.018) (Figure 2).
Correlations between height, BMI, and OFC measurements and ocular data in thalassemia patients grouped by ferritin levels.

ACD, anterior chamber depth; ACV, anterior chamber volume; AL, axial length; BMI, body mass index; CCT, central corneal thickness; ICA, iridocorneal angle; IOP, intraocular pressure; Kmean, mean keratometry; LT, lens thickness; OFC, occipitofrontal circumference; PD, pupil diameter; VCD, vitreous chamber depth.
p: Spearman’s rho correlation.

Correlations between OFC and Kmean in patients with ferritin levels below 1000 ng/mL.

Correlations between PD and BMI in patients with ferritin levels above 1000 ng/mL.
Discussion
Thalassemia major is a disease that requires lifelong regular blood transfusions and chelation therapy. Therefore, it causes serious socioeconomic problems in regions where it is common. In Greek and Turkish populations in Cyprus, the carrier prevalence was reported to be as high as 15%. 6 There is a paucity of data regarding ocular changes in TM patients. 7 Therefore, it is important to conduct studies on thalassemia in this region.
Growth retardation is a frequent problem in children with TM after multiple transfusions, particularly after 10 years of age. 8 In a study including subjects between 8 and 30 years of age, it was found that height and weight were lower in TM patients, while OFC did not differ from the control group. 9 In a study by El-Haddad et al., 10 TM children with a mean age of 16.43 ± 3.99 years had shorter height and larger OFC. Elkitkat et al. 11 evaluated participants with a similar mean age to those in our study (12.79 ± 1.87 years and 11.65 ± 2.72 years, respectively) and reported that children with TM had lower height, weight, and BMI but no difference in OFC compared with healthy controls. In our study, height, weight, and BMI were lower in TM patients compared with the healthy control group, while OFC was higher.
Craniofacial alterations may be the most common cause of an abnormal bony orbit. 12 In a study evaluating biometric parameters together with anthropometric measurements, TM patients were found to have short AL, short VCD, thicker crystalline lens, and steeper corneal keratometry readings. 11 In a study evaluating only AL, no significant difference between the TM and control group was observed. 13 In a study by Heydarian et al. 14 in which the mean age was higher than in our study (25.40 ± 6.9 years; range, 14–38 years), AL and VCD were significantly smaller in TM patients, but there was no significant difference in ACD or LT values. In the present study, there were no significant differences in AL, ACD, VCD, LT, or Kmean compared with the control group. However, even if the differences were not statistically significant, we observed that AL, ACD, VCD, and LT values tended to be lower and Kmean values tended to be higher in TM patients than in the control group. We believe that the changes in AL, LT, and thus in the other biometric parameters may be related to disease duration and the difference in the age groups in the studies. The TM patients already got blood transfusion and iron-chelating agent treatment. It is conceivable that blood transfusions and chelation therapy may affect the results of the study, but we know that despite treatment, patients develop typical craniofacial appearance with bone abnormalities and changes in ocular biometry and refraction with enlargement of orbital bones. 9
In our study, we observed no significant difference in CCT, ACV, or ICA between the TM and control groups. El-Haddad et al. 10 evaluated ICA and reported no difference in nasal ICA but narrower temporal ICA in TM patients compared with healthy controls. The authors attributed this narrowing of the temporal angle to increased LT displacing the iris anteriorly. In our study, although ICA was moderately narrower in the TM group compared with the control group, the difference was not statistically significant (p = 0.239). We can associate this with the absence of an increase in lens thickness in the TM patients in our study and the use of different measurement methods in the two studies. In addition, as in the study by El-Haddad et al., 10 no significant difference in CCT was observed between the groups in our study.
In another study of patients receiving chelation therapy, none of the patients had uncorrectable changes in visual acuity, and the authors concluded that chelation therapy was safe in terms of retinal and optic nerve function. 7 The recommended target range for serum ferritin levels is between 500 and 1000 ng/mL. If serum ferritin level falls below 500 ng/mL in a patient receiving regular transfusions, the chelator dose should be reduced but treatment should not be discontinued unless the patient develops signs of chelator toxicity. 15 High ferritin indicates poor disease control that may affect the patient’s growth rate. 11 In our study, there was no significant difference between the groups in terms of height, weight, BMI, OFC, and ocular parameters in patients receiving oral deferasirox (DFX; Exjade®, Asunra®). This may be due to the difference in the number of patients in the two groups and the fact that the effect of the disease duration was not examined. However, there was a positive correlation between OFC and Kmean in patients with ferritin levels below 1000 ng/Ml (r = 0.573, p = 0.025). This confirms that disease control is better in patients with low ferritin levels and that OFC should be smaller and Kmean lower, similar to healthy controls.
One study demonstrated decreased choroidal thickness in TM patients. 16 As the ciliary body is a part of the uveal tract, this decrease in choroidal thickness will also be reflected in the ciliary body. Reduced ciliary body thickness may cause zonular relaxation and increased lens thickness, resulting in anterior displacement of the iridolenticular diaphragm. 17 This movement may also cause an increase in PD. In our study, there was no statistically significant difference in PD measurements between TM patients and healthy controls. We were unable to find any data on this subject in the literature. However, we believe the statistically nonsignificant tendency toward higher PD despite slightly lower LT in the TM patients in our study may have been associated with displacement of the iridolenticular diaphragm due to a change in choroidal perfusion. In addition, a significant negative correlation was detected between BMI and PD in patients with serum ferritin levels above 1000 ng/mL (r = −0.469, p = 0.018). This shows that in patients with high serum ferritin levels, PD also increases in parallel with the decline in BMI resulting from poor disease control.
The first step in the management process of thalassemia patients is regular blood transfusion. While transfusions are applied more regularly in developed countries, they can be applied only when the risk of heart failure occurs in developing countries. The difference in the results of the studies may also be due to the difference in the frequency of transfusion.
The major limitation of this study was that the participants in the TM group were receiving chelation therapy.
In conclusion, children with TM had significant growth retardation and large OFC, but biometrics and anterior segment morphology were not different from healthy children. There was a positive correlation between OFC and Kmean in children with ferritin levels below 1000 ng/mL, which indicates good disease control, and a negative correlation between BMI and PD in children with ferritin levels higher than 1000 ng/mL.