
Abstract
Continuous control of intraocular pressure (IOP) is crucial to preventing long-term damage to the optic nerve in glaucoma. Recently, a novel telemetric IOP sensor (EYEMATE-IO™, Implandata Ophthalmic Products GmbH, Hannover, Germany) has been developed that continuously records IOP. The patient can read the IOP measurements wirelessly using a hand-held reading device. We present the case of a 70-year-old patient with primary open-angle glaucoma who had been implanted with an EYEMATE-IO™ and recently underwent minimally invasive bleb-filtering surgery with the PreserFlo® MicroShunt (Santen, Osaka, Japan). This case demonstrates both the benefits of continuous pressure measurement with EYEMATE-IO™ and the ability of the PreserFlo® MicroShunt to significantly reduce IOP fluctuations.
Keywords
Introduction
Continuous control of intraocular pressure (IOP) is crucial to preventing long-term damage to the optic nerve in glaucoma. 1 Normally, IOP measurement can only be performed during the opening hours of the doctor’s office, and elevations in IOP in the evening and at night or other fluctuations may remain unnoticed. The number of IOP examinations was even lower than usual during the coronavirus disease 2019 (COVID-19) pandemic. 2 In this context, remote and continuous monitoring of telemetric IOP measurements is a valuable tool in glaucoma management as it can potentially prevent visual loss. 3
The novel telemetric IOP sensor EYEMATE-IO™ (Implandata Ophthalmic Products GmbH, Hannover, Germany) is implanted in the ciliary sulcus and enables continuous IOP monitoring. The sensor performs 10 individual measurements (‘samples’) within 2 s, which are then averaged. The device has been described in detail elsewhere. 4 The patient can access the IOP measurements wirelessly using a hand-held reading device. Previous studies have shown good correlation between telemetric IOP and Goldmann applanation tonometry (GAT). 4
The PreserFlo® MicroShunt (Santen, Osaka, Japan) is effective in lowering IOP in primary open-angle glaucoma. 5 It, however, is currently unclear whether it can reduce IOP fluctuations and to what extent. Here, we report the case of a patient who performed telemetric self-measurements with an EYEMATE-IO™ and underwent minimally invasive filtering bleb surgery with the PreserFlo® MicroShunt.
Case
A 70-year-old patient with primary open-angle glaucoma was implanted with a second-generation EYEMATE-IO™ device during cataract surgery in the right eye as part of a clinical trial in 2015. At that time, he had been diagnosed with glaucoma for 29 years. He had not undergone previous eye surgery at the time of EYEMATE-IO™ implantation. Glaucoma was mild in both eyes, with a mean visual field defect of 4.8 and 2.4 dB in the right and left eye, respectively. The IOP was well regulated with local latanoprost and brimonidine. We followed the patient regularly until the outbreak of the COVID-19 pandemic in 2020. During that time, visits to the clinic were highly restricted, and the patient was seen only twice per year. In addition, the patient’s wife had a serious illness and was in constant need of care, so the patient was additionally restricted in his visits the Eye Hospital. In May 2021, the EYEMATE-IO™ recorded an increase in the IOP in the right eye. During a visit arranged at short notice, the EYEMATE-IO™ measurements revealed IOP values between 24.8 and 26.6 mmHg, which were verified by three GAT measurements showing values between 26.0 and 28.0 mmHg in the right eye. The antiglaucoma medication was changed to a preservative-free combination of bimatoprost/timolol and dorzolamide; however, severe allergic eczema of the eyelids and the periocular skin developed. In December 2021, the patient’s GAT IOP values were between 34.0 and 37.0 mmHg (three measurements). Self-measurements obtained via the EYEMATE-IO™ during the same visit showed IOP values between 41.3 and 42.0 mmHg (three measurements). On gonioscopy, the anterior chamber angle was Shaffer grade IV in all quadrants, with normal pigmentation of the trabecular meshwork. Furthermore, there was no change in the position of the EYEMATE-IO™, which could have explained the IOP elevation. Several mechanisms might have caused the increase in IOP, including the course of the disease, loss of IOP reduction capacity of the antiglaucoma medications, and loss of adherence to therapy due to the adverse effects caused by the medications. 6 In addition, optical coherence tomography (OCT) demonstrated progressive loss of the retinal nerve fiber layer of 2.9 µm per year in the last 2 years.
Because the glaucoma was progressive on OCT and the IOP was elevated on maximal-tolerated medication, the decision was made to perform minimally invasive bleb surgery in the right eye with the PreserFlo® MicroShunt. Antiglaucoma medications were stopped in the right eye 2 weeks prior to surgery, and systemic acetazolamide 250 mg twice daily was given instead. Unpreserved dexamethasone eye drops were given three times daily in the right eye 1 week before surgery. The surgery was uncomplicated, and the postoperative care was unremarkable. Moxifloxacin eye drops were given for 1 week four times daily, and unpreserved dexamethasone eye drops were tempered over 6 weeks. The patient continued to conduct IOP self-measurements with the EYEMATE-IO™ postoperatively. At 3-month follow-up, we observed a moderately elevated, posterior, well-functioning filtering bleb in the right eye. The IOP was 14.5 mmHg (mean of two measurements) with GAT and 15.5 mmHg (mean of two measurements) with the EYEMATE-IO™. The patient was medication free in the operated eye. A further follow-up was scheduled in 6 months, and the patient was instructed to continue the IOP self-measurements. The patient was prompted to contact the clinic immediately if his IOP increased over 20.0 mmHg to arrange an earlier visit. The telemetrically obtained IOP data between January 2021 and the time of publication of this report are presented in Figure 1.

The intraocular pressure (IOP) curve obtained from self-measurements recorded using the novel telemetric IOP sensor EYEMATE-IO™. The data from 2772 IOP measurements recorded from January 2021 to November 2022 are shown. The PreserFlo® MicroShunt was implanted on 1 February 2022, as demonstrated by the sudden drop in IOP after that date.
Statistical analysis was performed to compare the mean IOP values collected by the EYEMATE-IO™ during follow-up. IOP decreased significantly from 28.7 ± 8.3 mmHg at baseline (range = 13.5–49.1 mmHg, 76 measurements) to 14.6 ± 2.7 mmHg at 3 months (range = 8.1–22.4 mmHg, 137 measurements), 12.7 ± 2.2 mmHg at 5 months (range = 6.8–17.9 mmHg, 120 measurements), 14.1 ± 2.2 mmHg at 7 months (range = 8.6–19.7 mmHg, 81 measurements), and 14.6 ± 2.7 mmHg at 9 months after surgery (range = 8.4–22.3 mmHg, 73 measurements), respectively. The self-measured IOP values during the preoperative month and postoperative months 3, 5, 7, and 9 – depending on the time of the day – are presented in Tables 1 and 2 and Figure 2. In addition, the 24-h IOP fluctuations were considerably lower at all follow-up time points compared with the fluctuations recorded during the preoperative month (Figures 2 and 3).
Preoperative and postoperative intraocular pressure (IOP) recorded by the EYEMATE-IO™ sensor.

The monthly number of measurements, mean value ± standard deviation (SD) IOP, minimal (Min) and maximal (Max) IOP, and the difference between the monthly mean and preoperative mean IOP are shown.
Diurnal preoperative and postoperative intraocular pressure (IOP) recorded by the EYEMATE-IO™ sensor.

The number of measurements and mean value ± standard deviation (SD) IOP during each period are shown.

The diurnal distribution of intraocular pressure (IOP) measurements in the month before PreserFlo® MicroShunt implantation and at 3, 5, 7, and 9 months after implantation.
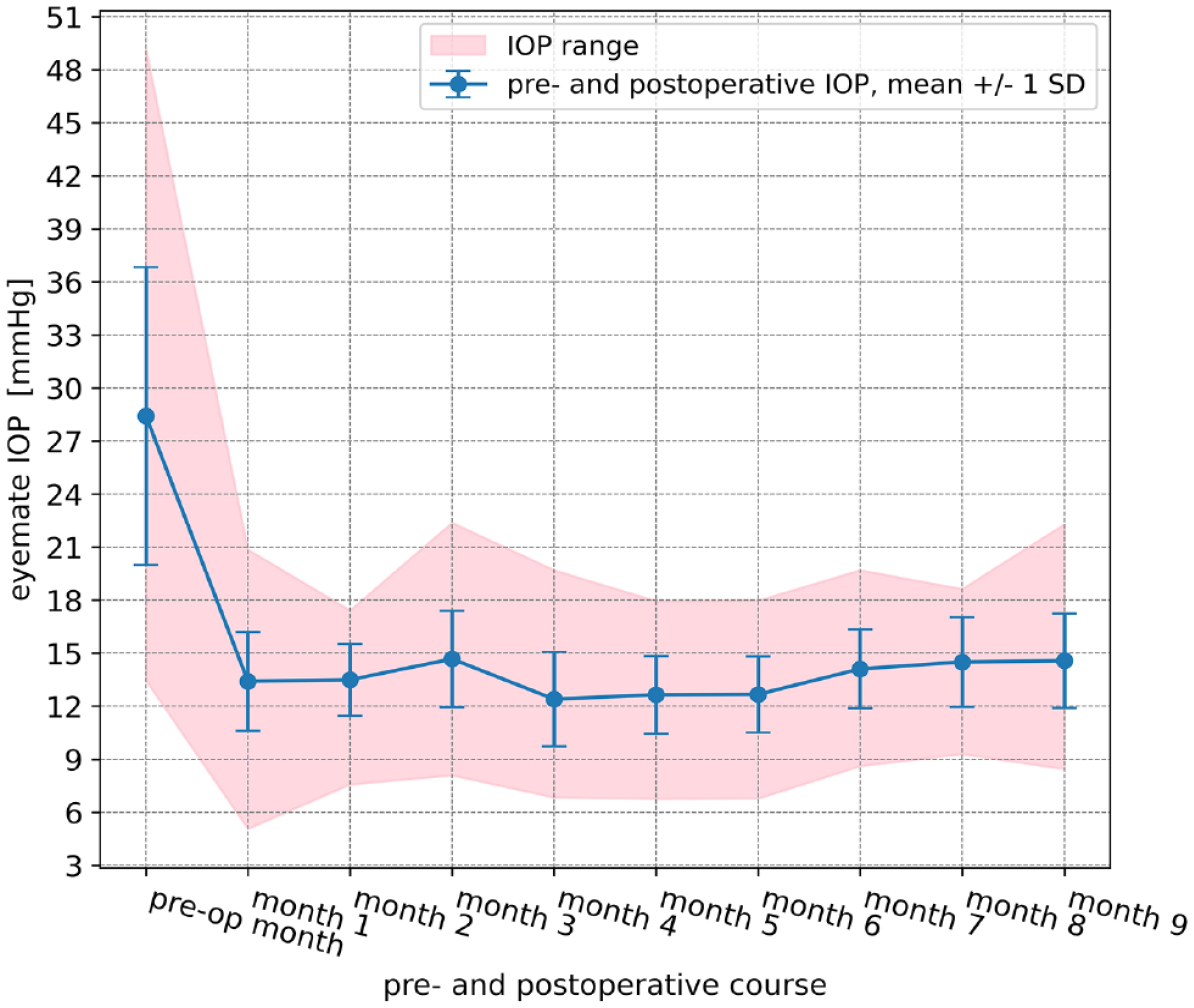
Mean intraocular pressure (IOP) ± standard deviation (SD) and range 1 month before and up to 9 months after implantation of the PreserFlo® MicroShunt.
Discussion
The number and frequency of IOP measurements of glaucoma patients are usually restricted by the opening hours of the doctor’s office; the COVID-19 pandemic caused further restrictions in the medical care of these patients. This case study shows the advantages of self-tonometry with a telemetric IOP sensor in the management of glaucoma patients. In addition, the EYEMATE-IO™ measurements demonstrated that the PreserFlo® MicroShunt effectively reduces IOP and IOP fluctuations over a follow-up period of at least 9 months.
Unlike other telemetric devices that measure IOP-related changes in the eye, the EYEMATE-IO™ measures actual IOP. 7 High agreement was demonstrated between the IOP values measured with the EYEMATE-IO™ and those measured with GAT. 4 Several studies have reported diurnal IOP fluctuations and poorly repeatable IOP patterns from day to day in patients with primary open-angle glaucoma.8,9 Furthermore, large IOP fluctuations alone are an independent risk factor for glaucoma progression. 10 Usually, IOP measurements are only collected from a patient during the normal opening hours of practices and clinics, and critical IOP elevations can thus be completely overlooked. Even daytime IOP profiles or inpatient night-time IOP measurements do not capture as many values as a telemetric sensor. In our case, the patient was restricted in his visits to the clinic on a regular basis due to both the COVID-19 pandemic and his wife’s serious illness. The telemetric measurements were the only possible method of follow-up of his treatment success, and it was the data from his EYEMATE-IO™ that first notified us of his increasing IOP despite antiglaucoma medication. Therefore, telemetry played a key role in the decision to perform surgery. Postoperatively, we were able to arrange fewer visits to the clinic than usual because the patient was instructed to continue the telemetric IOP measurements and to contact us immediately in case of an increase in IOP. Interestingly, the patient measured the IOP at different time points during the day despite not being specifically instructed to do so. These data demonstrated that both the IOP and IOP fluctuations during a 24-h period were greatly reduced. It is unclear whether some of the measurements were taken during sleep by a second person; this is possible with the EYEMATE-IO™, which enables position-dependent and activity-dependent IOP measurements.11,12
Nonadherence is common in glaucoma patients; nonadherence rates in these patients range from 5% to 80%. 6 Patient adherence to therapy can be improved by putting them in charge of their glaucoma care and providing them with the means for accurate self-measurements, as demonstrated by Astakhov et al. 13 for the iCare® Home tonometer (iCare Finland Oy, Vantaa, Finland). Furthermore, a study assessing the impact of self-tonometry on clinical treatment decisions demonstrated that higher IOP values detected via the iCare® Home tonometer led to intensification of medical glaucoma treatment. 14 The case of a patient who observed paradoxical IOP responses to dorzolamide administration in telemetric measurements with the EYEMATE-IO™ is illustrative of the benefits of the telemetric sensor. 15 In our case, the COVID-19 pandemic and the serious illness of his wife both impacted the patient’s adherence to follow-up examinations. Nevertheless, the IOP was still recorded meticulously using the EYEMATE-IO™.
It should be noted that the EYEMATE-IO™ itself might influence the IOP, as the procedure requires slightly more manipulation compared with stand-alone phacoemulsification with intraocular lens implantation. Topical steroids are often prescribed after implantation, which can lead to a temporary increase in IOP. In addition, the sensor can influence the flow dynamics of the aqueous humor and cause pigment dispersion from the iris due to its localization in the sulcus ciliaris. 15 Most of these factors, however, play a role in the early postoperative phase; in the case presented here, the EYEMATE-IO™ had been in place for 7 years. According to gonioscopy, the anterior chamber angle was Shaffer grade IV in all quadrants, with normal pigmentation of the trabecular meshwork, and there was no change in the position of the EYEMATE-IO™ over time.
A recent study reported that the PreserFlo® MicroShunt is as effective and safe as trabeculectomy but is less invasive in the treatment of primary open-angle glaucoma. 16 A number of studies have also demonstrated a good safety profile and favorable postoperative outcomes for the PreserFlo® MicroShunt.17–20 Similarly, our case study showed a significant reduction in IOP over a period of 9 months. Even more interestingly, the PreserFlo® MicroShunt was able to significantly and reliably decrease IOP fluctuations over a 24-h period and over 9 months.
We acknowledge that this is a single case with a follow-up of only 9 months. We will continue to follow-up the patient to learn more about the long-term efficacy of the PreserFlo® MicroShunt. In addition, we plan to study the influence of different physical activities on IOP and IOP fluctuations in this patient.
Conclusion
To our knowledge, this case report is the first to demonstrate a significant reduction in IOP and IOP fluctuations after the implantation of a PreserFlo® MicroShunt using a novel telemetric IOP sensor. Continuous IOP self-measurement with the EYEMATE-IO™ can play an important role in glaucoma management despite limited resources or individual factors limiting access to a healthcare system, as demonstrated in our case.