
Abstract
Background:
Diabetic retinopathy, a common microvascular complication of diabetes mellitus, is one of the leading causes of vision loss worldwide. Although some oral drugs have been suggested to affect the risk of diabetic retinopathy, systematic evaluation about the associations between medications and diabetic retinopathy is still absent.
Objective:
To comprehensively investigate associations of systemic medications with incident clinically significant diabetic retinopathy (CSDR).
Design:
Population-based cohort study.
Methods:
From 2006 to 2009, more than 26 000 participants residing in New South Wales were enrolled in the 45 and Up study. Diabetic participants with self-reported physician diagnosis or records of anti-diabetic medication prescriptions were finally included in the current analysis. CSDR was defined as diabetic retinopathy cases requiring retinal photocoagulation recorded in the Medicare Benefits Schedule database from 2006 to 2016. Prescriptions of systemic medication from 5 years to 30 days prior to CSDR were retrieved from the Pharmaceutical Benefits Scheme. The study participants were equally split into training and testing datasets. Logistic regression analyses were performed for the association between each of systemic medication and CSDR in the training dataset. After controlling the false discovery rate (FDR), significant associations were further validated in the testing dataset.
Results:
The 10-year incidence of CSDR was 3.9% (n = 404). A total of 26 systemic medications were found to be positively associated with CSDR, among which 15 were validated by the testing dataset. Additional adjustments for pertinent comorbidities suggested that isosorbide mononitrate (ISMN) (OR: 1.87, 95%CI: 1.00–3.48), calcitriol (OR: 4.08, 95% CI: 2.02–8.24), three insulins and analogues (e.g., intermediate-acting human insulin, OR: 4.28, 95% CI: 1.69–10.8), five anti-hypertensive medications (e.g., furosemide, OR: 2.53, 95% CI: 1.77–3.61), fenofibrate (OR: 1.96, 95% CI: 1.36–2.82) and clopidogrel (OR: 1.72, 95% CI: 1.15–2.58) were independently associated with CSDR.
Conclusion:
This study investigated the association of a full spectrum of systemic medications with incident CSDR. ISMN, calcitriol, clopidogrel, a few subtypes of insulin, anti-hypertensive and cholesterol-lowering medications were found to be associated with incident CSDR.
Introduction
Diabetic retinopathy (DR) is one of the most common microvascular complications of diabetes mellitus (DM) and the leading cause of acquired vision loss worldwide among the working-age population. 1 With the increasing global burden of DM and population aging, an estimated 245 million people will have DR globally by 2045. 2 Visual impairment and blindness due to DR have a significant impact on the quality of life and impose a tremendous socioeconomic burden for both individuals and society. 3
With the rapid development of the pharmaceutical industry, an increasing number of medications are available for use and polypharmacy has become more common. This leads to growing interest in the associations between systemic medications and DR. Recently, the effects of anti-hypertensive,4,5 cholesterol control,6–9 anti-diabetic, 10 and anti-depressant 11 drugs on DR have been intensively investigated. However, previous studies mostly focused on only one or a few systemic medications and estimated medication exposures based on questionnaires, which might be subject to selective reporting bias and recall bias.
Genome-wide associated study (GWAS) is an unbiased and statistically powerful method and has been widely used for identifying genotype–phenotype associations through testing millions of genetic variations. We have proposed a medication-wide association study (MWAS) which is analogous to GWAS in basic principles. This approach allows us to comprehensively search for and validate the associations between all available medications and a specific disease, thus avoiding selective reporting bias. 12 A comprehensive understanding of the association between systemic medications and DR may provide insights into the underlying mechanisms of DR and facilitate the development of new treatments.
Therefore, we aimed to comprehensively investigate associations of systemic medications with clinically significant diabetic retinopathy (CSDR) in working-age Australian populations.
Methods
Data sources
This study was conducted based on the data obtained from the Sax Institution’s 45 and Up Study, which is the largest population-based cohort study in the Southern Hemisphere. The methodology of this study has been described in detail elsewhere. 13 In brief, participants aged 45 years and above residing in New South Wales were randomly sampled from the Services Australia (formerly the Australian Government Department of Human Services) Medicare enrollment database and invited to join the study by mail. Baseline recruitment commenced in February 2006 and was completed by the end of 2009. Participants joined the study by completing questionnaires and written consent forms for linkage of their medical information to health databases and long-term follow-up. A total of 267,153 participants, about 10% of the New South Wales general population aged 45 years and above, were enrolled in the study at the baseline, and the overall response rate was estimated to be 18%.
The demographic and social characteristics and general health-related data were collected from the self-report questionnaire at baseline, which is available at https://www.saxinstitute.org.au/solutions/45-and-up-study/use-the-45-and-up-study/data-and-technical-information/. Medical information was extracted from two Australian healthcare databases, the Medicare Benefits Schedule (MBS) and Pharmaceutical Benefits Scheme (PBS) databases, which were linked to the 45 and Up Study participants by the use of an identification number assigned by the Services Australia. The MBS database records all the information on claims for medical and diagnostic services provided through Medicare, while the PBS database records the claims for prescribed medications. Both the MBS and PBS data were available from January 2004 to December 2016.
Study population
Diabetic participants aged 45–64 years were included in the present study. The methods used to identify diabetes status were consistent with previous studies, which had been proven to be of high sensitivity and specificity.14,15 Specifically, participants who reported physician-diagnosed diabetes or had records of anti-diabetic medication prescriptions before the baseline recruitment were identified as diabetic participants. Exclusion criteria of this study included (1) gestational diabetes, defined as no anti-diabetic medication records after the last childbirth but report a history of diabetes in the questionnaire; 14 (2) a history of vitrectomy prior to 1 January 2006 (MBS code: 42725); and (3) a history of retinal photocoagulation (RPC) treatment prior to 1 January 2006 (MBS code: 42809). The process of participant selection is summarized in Figure 1.
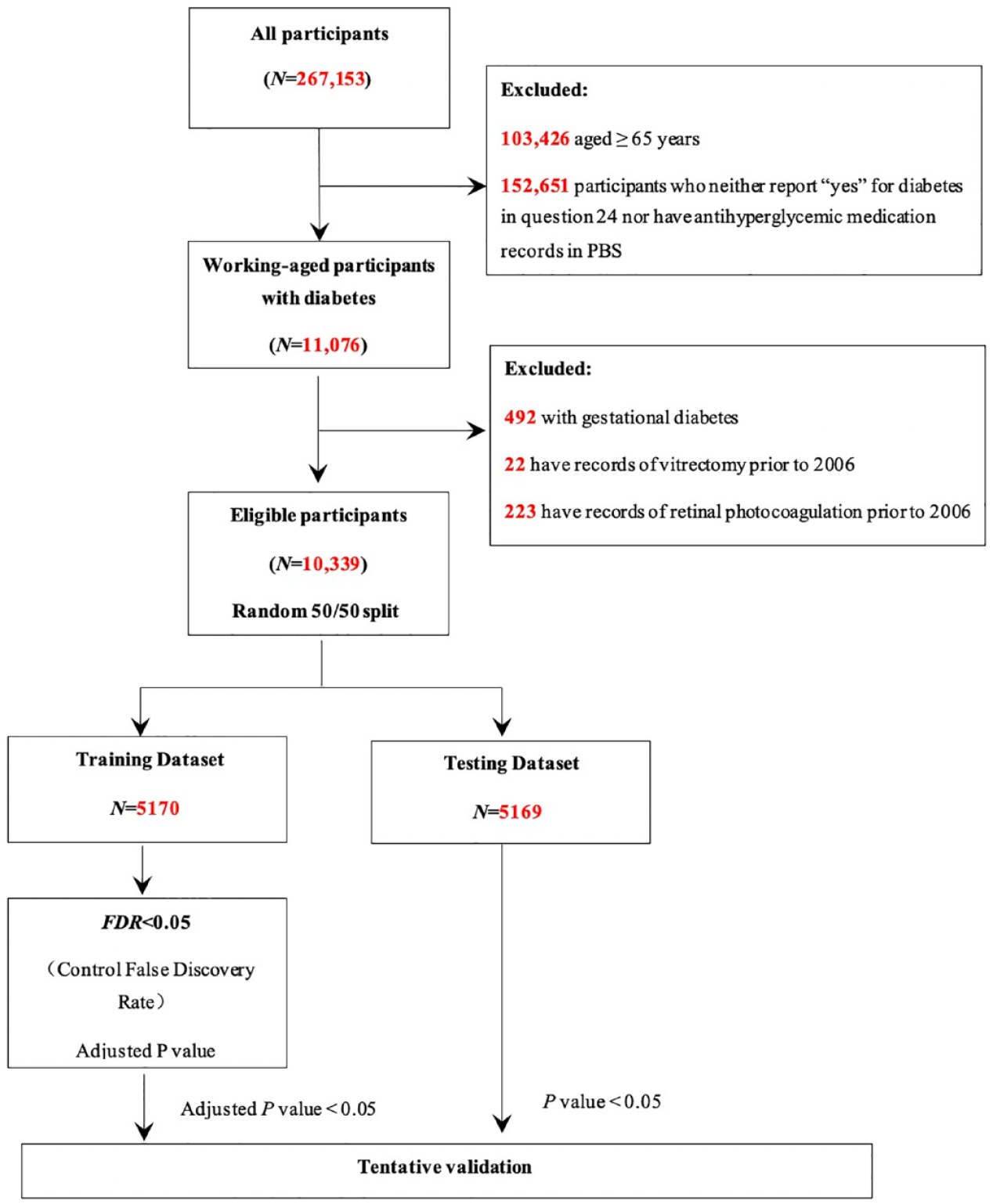
Methodology to identify eligible participants and scan for systemic medications associated with clinically significant diabetic retinopathy.
Definition of CSDR
CSDR, representing proliferative diabetic retinopathy (PDR) or diabetic macular edema (DME) requiring laser therapy, was defined as incident RPC treatment from 1 January 2006 to 31 December 2016 (MBS code, 42809). The index date was defined as the date of the first RPC treatment.
Definition of medication exposure
We obtained medication information from the PBS database for each participant during their identification period, that is, from 5 years to 30 days prior to the index date for participants with CSDR, and from study entry to 31 December 2016 for those without CSDR. Medications prescribed for ophthalmic indications or used by less than 1% of the included participants were excluded from the analysis. Systemic medications were analyzed by the fifth level code of the Anatomical Therapeutic Chemical (ATC) classification system. Participants with at least three fillings of a particular systemic medication during the identification period were classified as exposed to that medication; participants without such records were classified as non-exposed. Those with one or two fillings were classified as having uncertain exposure and were excluded from the analysis for that particular medication analysis.
Potential confounders
Potential confounders included sociodemographic characteristics (age, gender, education level, household income per year, health insurance status, and remoteness index) and comorbidities (history of hypertension, dyslipidemia, cardiovascular diseases [CVD], and osteoporosis). Age was classified into four groups: 45–49, 50–54, 55–59, and 60–64 years. Household income per year was categorized into four groups: <AU$20,000, AU$20,000–AU$40,000, AU$40,000–AU$70,000, and >AU$70,000. Education level was divided into three classes: no qualifications, completion of a certificate or diploma or trade but lower than a university degree, and a university degree or above. Health insurance types included private with extras, private with no extras, veteran’s card, health care concession card, and others. The remoteness index was classified into major cities, inner regions, outer regions, and remote and very remote areas. A history of CVD was defined as a self-reported physician diagnosis of any type of heart disease or stroke, or any treatment received in the last month for heart attack, angina, or other heart diseases. Histories of hypertension, dyslipidemia, and osteoporosis were based on information from questionnaires.
Statistical analysis
The software used for statistical analysis in the study included SAS version 9.4 and R version 3.3.0 (R Foundation for Statistical Computing, www.R-project.org). To validate our results, a random 50:50 split was performed to divide participants into the training dataset and the testing dataset (Figure 1). Baseline characteristics of the participants were reported using means and standard deviations (SDs) for continuous variables and numbers and proportions for categorical variables. Student’s t test for continuous data was used for comparison between participants in the training and testing dataset, while Pearson’s chi-square test was used for the comparison of categorical data. A two-sided p value < 0.05 was considered statistically significant.
Logistic regression models (model 1) adjusting for age, gender, education level, household income, health insurance status, and remoteness index were used separately to assess the association of each systemic medication with incident CSDR. To reduce the risk of overadjustment, pertinent comorbidities including the history of hypertension, dyslipidemia, CVD, and osteoporosis were adjusted for in further analyses (model 2) of those medications which were significantly associated with CSDR in the first analyses (model 1). The odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. In the training dataset, the Benjamin–Hochberg procedure was used to control the false discovery rate (FDR) at the level of 5%. If a systemic medication achieved FDR <5% significant in the training dataset and nominal statistical significance in the testing dataset (p < 0.05), it was deemed tentatively validated.
To improve the generalizability of our findings, a sensitivity analysis was performed to investigate the association between tentatively validated systemic medications and incident CSDR among participants stratified by the remoteness index. Participants who lived in major cities were selected as the training dataset, while the remaining participants were classified as the testing dataset. Subgroup analyses were conducted to explore whether pertinent comorbidities could modify the associations between systemic medications and incident CSDR. The interaction between medication and pertinent comorbidity was considered statistically significant when p value for their interaction was less than 0.05 and then a further subgroup analysis would be conducted.
Results
Study population
Among 267,153 participants at baseline, a total of 10,339 participants met the inclusion and exclusion criteria. Figure 1 provides more details on the participant selection process. The mean age of included participants was 57.2 years with a standard deviation of 5.2 years, and 45.2% of participants were female. Comparisons of baseline participants’ characteristics between the training and testing datasets are shown in Table 1. Participants in the training and testing datasets had similar baseline characteristics.
Baseline characteristics of participants in the training and testing datasets.

CSDR, clinically significant diabetic retinopathy.
Associations between medications and incident CSDR
During the study period, the number of participants who developed CSDR was 404 (3.9%). There was no significant difference in the incidence of CSDR between training and testing datasets (3.8% versus 4.0%, p = 0.610). Participants in the present study were exposed to 209 prescribed systemic medications in total. The three most commonly prescribed systemic medications in the training dataset were metformin, atorvastatin, and gliclazide, which were used by 73%, 49%, and 38% of participants, respectively. All systemic medications used by the participants in the training dataset are presented in Supplementary Table 1.
A total of 26 systemic medications were significantly associated with incident CSDR (FDR <5%) in the training dataset, and 15 of them were tentatively validated (p < 0.05) in the testing dataset. Figure 2 and Supplementary Table 1 show the associations between each of the analyzed systemic medications and incident CSDR in the training dataset. The results for associations between systemic medications and incident CSDR in the testing dataset are presented in Supplementary Table 2.
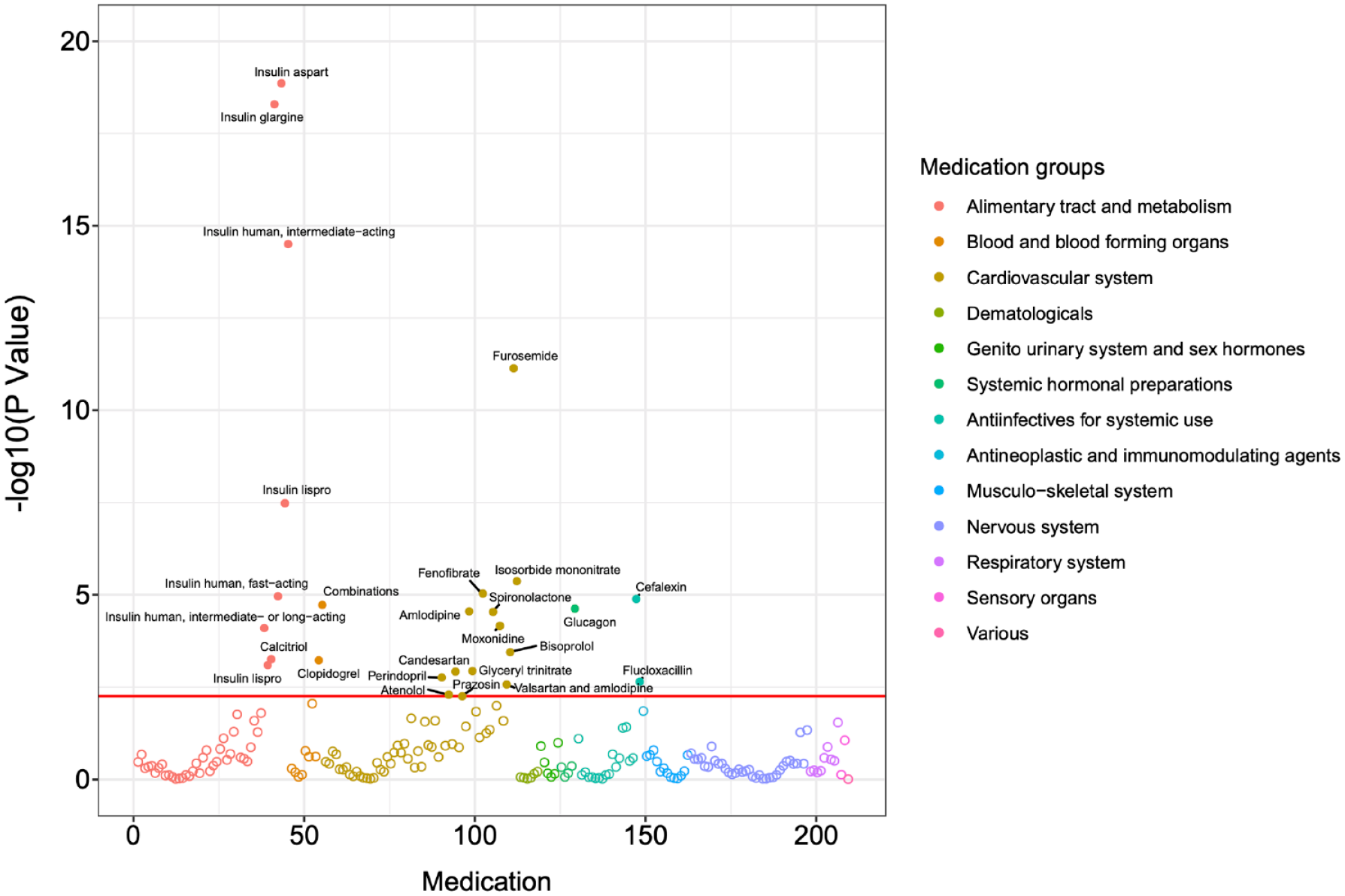
Manhattan plot shows results for the association between systemic medications and incident clinically significant diabetic retinopathy in the training dataset.
Table 2 presents the 15 validated systemic medications positively associated with incident CSDR. After further adjustments for demographic characteristics and pertinent comorbidities mentioned above (model 2), insulins and its analogs were associated with the largest risk of developing CSDR. The risk of CSDR in this medication subcategory ranged from the insulin glargine (OR: 2.22, 95% CI: 1.08–4.54) to intermediate-acting human insulin (OR: 4.28, 95% CI: 1.69–10.8). Five anti-hypertensive medications, including two diuretics (e.g., furosemide, OR: 2.53, 95% CI: 1.77–3.61), one calcium channel blocker (CCB) (amlodipine, OR: 1.47, 95% CI: 1.02–2.11), and two α-antiadrenergic agents (e.g. moxonidine, OR: 2.41, 95% CI: 1.51–3.85), were significantly associated with an increased risk of CSDR. One cholesterol-lowering agent (fenofibrate, OR: 1.96, 95% CI: 1.36–2.82), one vasodilator (isosorbide mononitrate [ISMN], OR: 1.87, 95% CI: 1.00–3.48), one vitamin D analog (calcitriol, OR: 4.08, 95% CI: 2.02–8.24), and one platelet aggregation inhibitor (clopidogrel, OR: 1.72, 95% CI: 1.15–2.58) also had significant positive associations with incident CSDR.
Systemic medications with positive associations with clinically significant diabetic retinopathy progression in the training and testing datasets.

CI, confidence interval; FDR, false discovery rate; ISMN, isosorbide mononitrate; OR, odds ratio. Boldface indicates statistical significance.
Number of participants: the number of participants exposed to each drug in the dataset.
Model 1: Adjusting for demographic covariates, including age, gender, educational level, household income, health insurance status, and remoteness index.
Model 2: Adjusting for covariates in model 1 plus hypertension, dyslipidemia, cardiovascular disease, and osteoporosis.
Sensitivity and subgroup analysis
In the sensitivity analysis (Supplementary Table 3), the results remained consistent with those of the main analyses apart from fast-acting human insulin (urban dataset: OR: 2.02, 95% CI: 0.96–4.23, p = 0.063) and prazosin (rural dataset: OR: 1.34, 95% CI: 0.77–2.34, p = 0.299). In the subgroup analyses, no interaction effects between medications and their pertinent comorbidities were statistically significant, except for fenofibrate and dyslipidemia (p-value for interaction = 0.007). Fenofibrate was consistently associated with an increased risk of CSDR for participants without dyslipidemia (OR: 2.79, 95% CI: 2.04–3.81), but no significant association was found for those with dyslipidemia (OR: 1.29, 95% CI: 0.84–1.98) (Supplementary Table 4).
Discussion
The present study was the first to comprehensively explore associations of systemic medications with incident CSDR using an approach analogous to GWAS. Exposures to subtypes of anti-diabetic (human insulin, insulin aspart, and insulin glargine), anti-hypertensive (diuretics, CCBs, and α-antiadrenergic agents), and cholesterol-lowering drugs (fenofibrate) were found to be associated with increased risks of developing CSDR. Novel associations of incident CSDR with ISMN and calcitriol were also identified, which had not been reported before.
One of the challenges in interpreting the association between medication use and disease outcome is to differentiate whether this association is caused by the medication or the disease for which the medication was indicated. Our study found that the use of diuretics (furosemide and spironolactone), CCBs (amlodipine), or α-antiadrenergic agents (moxonidine) was associated with an increased risk of developing CSDR. However, no significant association was found between the risk of developing CSDR and the most prescribed anti-hypertensive drug (perindopril: number of participants with perindopril exposure: 2416; training dataset: OR: 1.63, 95% CI: 1.20–2.21, FDR = 0.017; testing dataset: OR: 1.23, 95% CI: 0.89–1.69, p = 0.214). In addition, after adjusting for comorbidities including hypertension, the association between these anti-hypertensive drugs and incident CSDR remained significant. No significant interaction effects between hypertension and anti-hypertensive drugs were found. These findings support the hypothesis that these subtypes of anti-hypertensive drugs, rather than hypertension, were associated with increased risks of CSDR. 16 Similar findings were also observed for cholesterol-lowering drugs. After adjusting for relevant comorbidities such as CVD and hypertension, the associations remained significant.
We found that exposure to ISMN was associated with an increased risk of CSDR, which had not been reported before. Previous studies reported that the long-term use of oral nitrate might result in adverse cardiovascular events,17,18 possibly through nitrate tolerance, endothelial dysfunction, and oxidative stress.17,19,20 These pathophysiological processes may partly explain the positive association between ISMN and CSDR, as systemic and retinal vessels have many similarities in structure and physiology, 21 although further studies are needed to explore the exact mechanisms.
Calcitriol, the active form of vitamin D, was shown to be positively associated with CSDR in our study. Some indirect evidence has suggested that calcitriol may have an inhibitory role in the pathogenesis of DR. For example, a few epidemiological studies have found an increased risk of DR among participants with vitamin D deficiency.22–24 Vitamin D receptor and the enzymes involved in vitamin D metabolisms, such as 1a-hydroxylase and vitamin D3–inactivating enzyme 24-hydroxylase, were detected in the retina, suggesting it may function as a paracrine/autocrine regulator.25–27 In addition, its effects in reducing retinal neovascularization28,29 and inflammation,30,31 and improving glucose homeostasis and insulin sensitivity 32 provide further support for this association. However, the role of calcitriol supplementation in the formation or progression of DR still lacks direct evidence. We might speculate that calcitriol or additional vitamin D may not be beneficial to DR as patients taking calcitriol may have had a deficiency of vitamin D levels. Nevertheless, we could not obtain information on the serum vitamin D level and could not adjust for conditions requiring calcitriol treatment other than osteoporosis (i.e. renal disease).
Consistent with previous studies, insulins and its analogs were significantly associated with CSDR. 33 One possible explanation is the ‘early worsening’ phenomenon, which is the deterioration in DR precipitated by rapid reductions in serum glucose level and upregulation of vascular endothelial growth factor (VEGF) levels.33,34 Other potential explanations for this association include the insulin-associated vascular leakage mediated by betacellulin and signaling via the epidermal growth factor receptor 35 or the fact that insulin users may be more likely to have suboptimal glycemic control than those who were not on insulin. Regarding anti-hypertensive drugs, their associations with CSDR remain inconclusive.4,36,37 Positive associations of diuretics and CCBs with CSDR observed in our study were partially consistent with findings from Lin and Lai, 4 who were able to show angiotensin-converting enzyme inhibitors and/or angiotensin receptor blockers, CCBs, and diuretics were associated with higher risks of developing sight-threatening diabetic retinopathy in comparison with β-blockers. The discrepancy in associations between various anti-hypertensive drugs and CSDR may be partly explained by their differential effects on glycemic and metabolic control. 37 Spironolactone has been reported to have a glycemic worsening potential of 0.2% on patients’ hemoglobin A1c (HbA1c), 38 and this poor glycemic control may have negative effects on CSDR. As for clopidogrel, there is no direct evidence from human research on associations between clopidogrel and CSDR, although aspirin, another kind of antiplatelet agent, had no impact on DR progression or the rates of vitreous hemorrhage. 39 Findings on the association between fibrates and DR remain controversial.6,8,9,40,41 Two large clinical trials showed that fenofibrate slowed the progression of DR and reduced the need for laser treatment in type 2 diabetic patients with pre-existing retinopathy,9,40 whereas two real-world observational studies did not find such associations.6,8 The discrepancy between our findings and those of previous studies may be explained by different patient populations, different confounding factors controlled for, and the lack of data on lipid profiles in our study.
To the best of our knowledge, we were the first to investigate the association of a full spectrum of medications with incident CSDR using the MWAS approach. The MWAS approach used in the present study has several advantages. First, compared with previous studies that explored only one or a few medications at a time, MWAS enables investigations of associations between a wide range of medications and the target disease, thus reducing the risk of selective reporting bias. Second, the internal cross-validation by splitting randomly or based on the remoteness index in the included participants and FDR controlling add to the robustness of the results. Third, MWAS is a systematic and thorough method that may be applied to a wide range of other diseases in future studies. Last but not the least, novel associations identified by MWAS can provide insights into the biochemical and pathogenesis pathways behind diseases, as well as help to identify new therapeutic targets and potential side effects of a specific drug. A comprehensive understanding of all available medications’ association with a specific disease can guide clinicians and pharmacists in making management decisions. In addition to the advantages of the MWAS methodology, other strengths of the present analysis include the large sample size, the wide range of covariates adjusted for in the final models, and the use of the national claim data to estimate the exposure to systemic medications.
Several limitations of our study should also be noted. First, due to the data-driven and hypothesis-independent nature of MWAS, it is hard to determine whether these identified associations are casual or due to relevant comorbidities, which is also a limitation of other observational studies. The list of CSDR-associated systemic medications needs to be replicated using an independent sample and validated by further prospective interventional trials. Second, fundus imaging data were not available in this study; hence, the records of RPC were used to define CSDR, leading to potential biases. Some patients with CSDR may be treated with anti-VEGF or vitrectomy. However, according to the PBS schedule and Australian guidelines for the management of diabetic retinopathy in 2008, aflibercept or ranibizumab must be used in combination with RPC when treating DME, and RPC is also recommended before vitrectomy. Thus, almost all the patients receiving intravitreal injections or vitrectomy should be covered within the cases we tracked by RPC, although the actual number might be relatively underestimated. Third is the fact that information on other baseline systematic diseases (i.e. renal disease), types of diabetes, blood tests (i.e. HbA1c), and reasons for the prescription was not available in the 45 and Up study and was hence not taken into account in this analysis. The possibility of residual confounding could not be completely ruled out in this research, despite the fact that as many confounders as possible were adjusted for in this analysis. Further well-designed, hypothesis-dependent studies are required to validate the current findings. Finally, records from the PBS database could only provide information on the prescription of medications rather than the use of medications by participants. In future studies, electronic medication monitoring devices may be able to more accurately estimate the exact medication exposure.
In summary, the present analysis is the first to systematically explore associations between a full spectrum of systemic medications and CSDR to date. The novel positive associations observed between ISMN or calcitriol and incident CSDR may inspire future research into the relevant biochemical and pathogenic pathways underlying DR. The associations of insulin, anti-hypertensive, and cholesterol-lowering medications with incident CSDR may guide future clinical practice. Additional observational and experimental studies are needed to further validate these associations.
Supplemental Material
sj-docx-1-oed-10.1177_25158414221139002 – Supplemental material for A medication-wide association study to identify medications associated with incident clinically significant diabetic retinopathy
Supplemental material, sj-docx-1-oed-10.1177_25158414221139002 for A medication-wide association study to identify medications associated with incident clinically significant diabetic retinopathy by Ruilin Xiong, Wei Wang, Xianwen Shang, Yixiong Yuan, Yifan Chen, Lei Zhang, Katerina V Kiburg, Zhuoting Zhu and Mingguang He in Therapeutic Advances in Ophthalmology
Footnotes
Acknowledgements
This research was completed using data collected through the 45 and Up Study (![]() ). The 45 and Up Study is managed by the Sax Institute in collaboration with major partner Cancer Council NSW and the following partners: the Heart Foundation; NSW Ministry of Health; NSW Department of Communities and Justice; and Australian Red Cross Lifeblood. We acknowledge that Services Australia supplied the Medicare Benefits Schedule (MBS) and Pharmaceutical Benefits Scheme (PBS) data to the Sax Institute. We thank the many thousands of people participating in the 45 and Up Study.
). The 45 and Up Study is managed by the Sax Institute in collaboration with major partner Cancer Council NSW and the following partners: the Heart Foundation; NSW Ministry of Health; NSW Department of Communities and Justice; and Australian Red Cross Lifeblood. We acknowledge that Services Australia supplied the Medicare Benefits Schedule (MBS) and Pharmaceutical Benefits Scheme (PBS) data to the Sax Institute. We thank the many thousands of people participating in the 45 and Up Study.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.