
Abstract
COVID-19 is a disease caused by a SARS-CoV-2 viral infection, a disease that was first detected in December 2019 in Wuhan, Hubei Province, China. COVID-19, formerly known as 2019 Novel Coronavirus (2019-nCoV) respiratory disease, was officially named COVID-19 by the World Health Organization (WHO) in February 2020. By 25 May 2021, there were 33,579,116 confirmed cases with 599,109 COVID-19 deaths worldwide. The purpose of this review article is to provide an update on what is currently known about COVID-19 ocular symptoms in adults, the elderly, and children in the literature. Finally, this article will review the eye protection precautions that should be implemented in our clinics. To assess the current literature, PubMed was searched from December 2019 to 25 May 2021. Randomized trials, observational studies, case series or case reports, letters of research, and letters to editors were selected for confirmed cases of COVID-19. According to current scientific literature since the outbreak in December 2019, 205 articles have been published. Conjunctivitis, conjunctival hyperemia, and chemosis have been reported in adults with COVID-19. There have been few studies on children and elderly patients, and further research in these age groups is needed. Finally, wearing eye protection when seeing patients on a daily basis during the pandemic is essential.
Keywords
COVID-19 is a disease caused by a SARS-CoV-2 virus infection first reported in Wuhan city, Chinese province of Hubei, in December 2019. COVID-19 presents with a wide range of severities and presentations for unclear reasons/mechanisms that may range from asymptomatic infection to severe disease and mortality. Systemic manifestation may precede ocular manifestation in around 0.28% of COVID-19-related patients with ocular symptoms. Furthermore, ocular manifestation was not linked to a severe type of COVID-19. 1 One study reported that one-third of patients with COVID-19 had ocular abnormalities, which occurred more frequently in patients with more severe COVID-19. 2
COVID-19 ocular symptoms have been related to positive upper respiratory infection symptoms and decreased creatine phosphokinase levels. 3 Despite negative nasal swab tests, the presence of SARS-CoV-2 viral RNA in aqueous indicates the persistence of virus beyond the blood-ocular barrier in asymptomatic people, raising the potential that the virus might survive in immunoprivileged spaces despite the lack of symptoms. 4 The discovery of SARS-CoV-2 RNA in ocular samples emphasizes the importance of the eye as a potential route of disease transmission. 5 SARS-CoV-2 RNA was found in the tears of 24% of individuals with laboratory-confirmed moderate to severe COVID-19. SARS-CoV-2 can be found in tears and conjunctival secretions6,7 and can be transmitted through the eyes. 2
Conjunctival swab is still the gold standard for reverse transcription polymerase chain reaction (RT-PCR) tear collection. Patients with moderate to severe COVID-19 have a substantially increased risk of viral transmission through tears. 8 Severe pneumonia was seen in 6.9% of patients with ocular manifestations. 9
Conjunctivitis2,10,11 and keratoconjunctivitis 12 are the most prevalent ocular symptoms in adults. 13 Conjunctival irritation was the most prevalent ophthalmological finding (50.8%), followed by diplopia (27.8%) and cotton wool patches (27.8%). 14 Males have been diagnosed with viral conjunctivitis at a higher rate than females. 15 The majority of the cases were acute COVID-19 cases, with some chronic COVID-19 cases observed in each case. Chronic COVID-19 cases have been termed ‘Long COVID’ or ‘COVID Long-Haulers’. 16 In China, Long COVID-19 has been reported, with COVID-19 symptoms lasting 6 months after the hospital discharge. 17
A number of literature reviews in ocular manifestations have been published, 13 and couple of the review articles concluded that further studies are required to determine the ocular manifestations in children and geriatric patients. 13 This article will examine the gaps by including ocular manifestations in children and geriatric patients, in addition to currently reported ocular manifestations in adults. Finally, the eye protection precautions that should be applied in our clinics will be covered.
Search strategy
PubMed search was performed from December 2019 to 25 May 2021. The key words ‘COVID-19’, ‘Ocular Manifestations’ and ‘SARS-COV-2’ were used individually or in combination. Randomized trials, observational studies, case series or case reports, letters of research, and letters to editors for confirmed cases of COVID-19 were covered. According to current scientific literature since the outbreak in December 2019, 205 papers have been written (Figure 1).
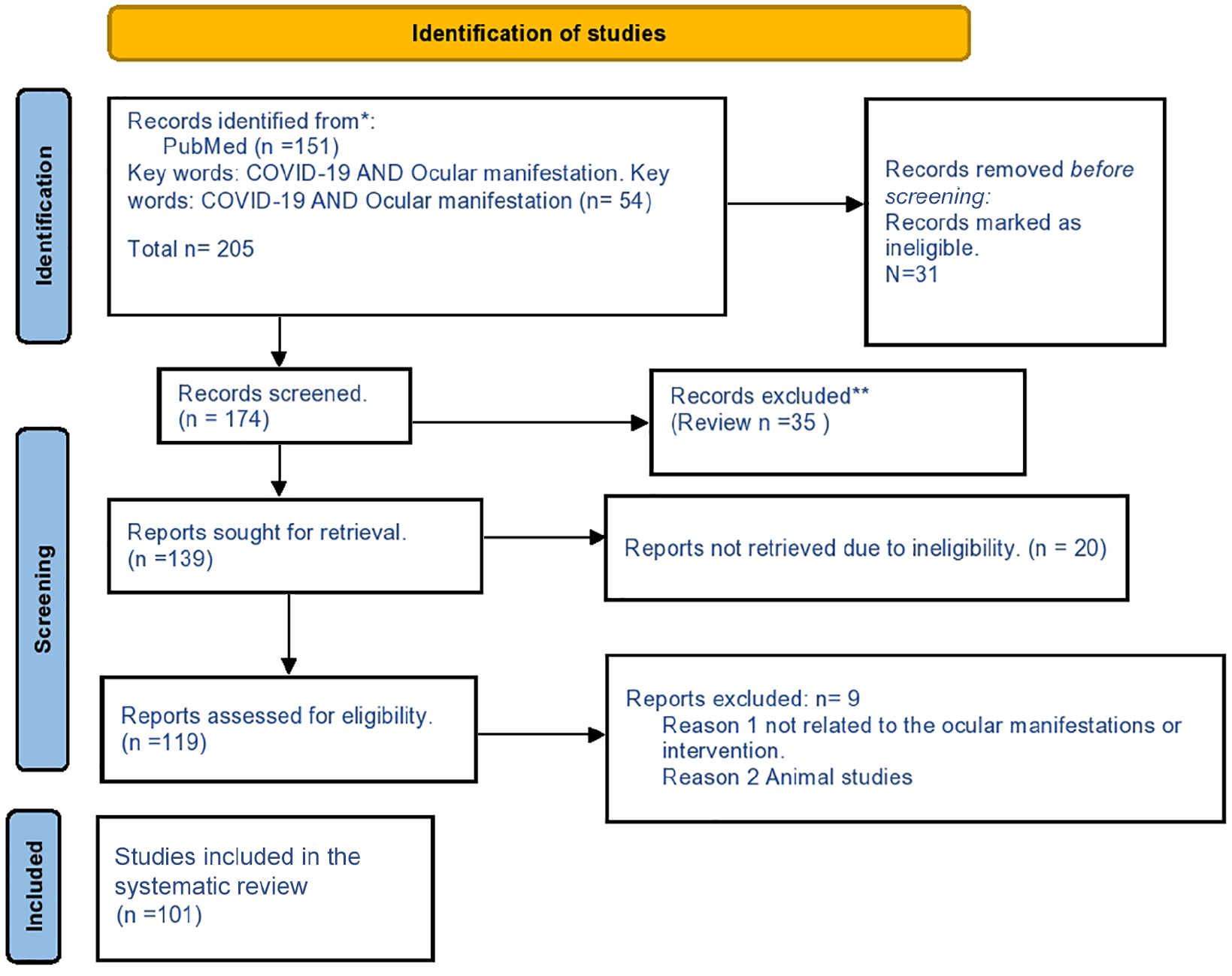
PRISMA 2020 flow diagram.
Adults’ ocular manifestations
Anterior segment
According to several studies, ocular symptoms are uncommon and unlikely to represent the presenting clinical impression in COVID-19 infection. 19 Furthermore, no epiphora, no secretion, or decreased vision has been reported. 20 Other studies concluded no eye problem reports in Thailand that could be related to the severity of the disease and low sample size. 21
In a study covering 43 COVID-19 patients, only one developed conjunctivitis with a foreign body sensation (2.3%). 22 Conversely, another study reported that 31.63% of COVID-19 confirmed cases demonstrated ocular symptoms, including conjunctiva hyperemia, chemosis, epiphora, and elevated secretions suggesting acute conjunctivitis.23,24
Ocular symptoms were found to be present in 2–32% of COVID-19-infected patients.15,25
The prevalence rate of acute conjunctivitis has been shown to range from 1.1% to 31.6%.2,15,23,26
Aggarwal et al. performed a meta-analysis with a total of 16 investigations, including 2347 verified COVID-19 cases. Ocular surface manifestations were found in 11.64% of COVID-19 patients, according to pooled data. The most common symptoms were ocular discomfort (31.2%), discharge (19.2%), redness (10.8%), and follicular conjunctivitis (7.7%). Severe pneumonia was seen in 6.9% of patients with ocular symptoms. In 3.5% of patients, viral RNA was found in their ocular sample. Ocular discomfort, redness, discharge, and follicular conjunctivitis were the most commonly reported ocular manifestations of COVID-19. In a small number of patients, viral RNA was found in their conjunctival/tear samples. There is a lot of publication bias and heterogeneity in the research that are available. 9
Cavalleri et al. hypothesized that although ocular symptoms are common in COVID-19 patients, the presence of SARS-CoV-2 in ocular secretions is rare. Ocular symptoms in COVID-19 hospitalized patients can also be caused by respiratory support treatment. It is nevertheless suggested to avoid potential transmission via ocular secretions. 27
Paradoxically, a large number of studies have reported ocular manifestations in COVID-19 patients. As shown in a meta-analysis study of the prevalence of COVID-19 ophthalmic manifestations, the prevalence of ocular manifestations in COVID-19-infected individuals ranged from 2% to 32%.15,25
Daruich et al. reported unilateral conjunctivitis as first sign of COVID-19 in 27-year-old male.11,28,29
The study by Bozkurt et al. 30 found that COVID-19 patients showed pathological conjunctival abnormalities and that pathological ocular surface abnormalities can occur even before clinically relevant ocular manifestations. Because viral RNA was found in 7% of patients’ conjunctival secretions, the possibility of ocular transmission should be considered even in the absence of visual symptoms.22,31
Conjunctivitis was the most common ocular condition among COVID-19 patients, accounting for 88.8% of all reported ocular disorders such as foreign body sensation, tearing, and dry eyes. According to the findings, one out of every 10 COVID-19 patients had at least one eye symptom. The sensitivity of COVID-19 detection among patients can be improved by paying attention to ocular symptoms, particularly conjunctivitis. 32 Positive upper respiratory infection symptoms were linked with conjunctival congestion in these patients. 3 Conversely, meta-analysis study showed that the non-severe COVID-19 patients appearing to be more likely to develop conjunctivitis. 33
Ocular symptoms might develop as a prodromal symptom in the presymptomatic phase (12.5%, 13/104 cases), implying viral transfer through the conjunctiva 34 and due to viral shedding of tears, extreme care must be taken.22,35,36
Conjunctival injection was the most frequent ocular abnormality, followed by visual changes and ocular irritation. 37 Méndez Mangana et al. 38 reported the first 31 White female who had episcleritis in a COVID-19-positive patient. Sriwastava et al. 39 reported the first case of myasthenia gravis in a 65-year-old female COVID-19-positive patient. HSV-1 keratitis had been reported in five cases. 40
Other ocular manifestations include dry eye syndrome and episcleritis. 41 Follicular conjunctivitis,9,41–44 conjunctival hyperemia, 11 chemosis, epiphora, and increased secretions have been reported.2,28 Increased conjunctival secretions, ocular pain, 9 ocular discharge and redness, 9 photophobia, dry eye, tearing, and conjunctival congestion, as well as xerophthalmia and keratitis, are chronic COVID-19 ocular manifestations. 26
Acute follicular conjunctivitis with preauricular lymphadenopathy (LAP) and anterior uveitis were observed. 45 Other study reported severe viral conjunctivitis with pseudomembranes on the tarsal conjunctiva with enlarged submaxillaries and preauricular lymph nodes. 46
Hemorrhagic conjunctivitis with pseudomembranes was reported in a 63-year-old male COVID-19 patient. 47
In one case study, a 53-year-old white male COVID-19 patient was diagnosed with blepharitis, and he was advised to keep using the warm compresses and take 100 mg of doxycycline if the symptoms persisted or did not improve. 48
This study found the same rate of positive findings in groups with and without conjunctivitis, indicating that identifying SARS-CoV-2 in ocular secretions is not dependent on conjunctivitis. 5
The SARS-CoV-2 virus can produce ocular symptoms such as viral conjunctivitis. Infected individuals with conjunctivitis and fever may benefit from conjunctival sampling. 49
As a diabetic, hypertensive, and asthmatic 65-year-old COVID-19 patient, while on a ventilator, he developed severe follicular conjunctivitis of the right eye. The resolution of visual symptoms was observed over a period of 2 weeks with no problems. This case discussed and illustrated the sequence of events in individuals with COVID-19 infection who have long COVID-19 late ophthalmic symptoms. 50
During a lengthy COVID-19 lockdown, contact lens compliance was low, particularly in terms of handwashing and storage case cleanliness, emphasizing the necessity for patient–practitioner communication methods to reduce the risk of ocular transmission and viral tropism. 51 Despite the fact that the influence of eye allergy on everyday activities and emotions was limited, the influence of eye allergy symptoms during the quarantine period was determined to be considerable. 52
Posterior segment
Optic neuritis, disk edema, vascular tortuosity, acute macular neuroretinopathy (AMN), vasculitis retinal occlusion (RVO), retinal artery occlusions, intraretinal hemorrhages, cotton wool spots, uveitis, and endogenous endophthalmitis have all been reported in COVID-19 patients.53–58
A 22-year-old female with a history of absolute inferior scotoma in the right eye for 4 days and a fever and sore throat 10 days prior presented with parainfectious optic neuritis associated with acute COVID-19. Disk edema and vascular tortuosity were seen on a fundus examination. 53
A 33-year-old Malay man with concurrent cytomegalovirus (CMV) and COVID-19 infection was the first case of frosted branch angiitis (FBA) in a HIV-infected patient. He complained of impaired vision, ocular redness, dryness, and a foreign body sensation. 59
AMN as the presenting symptom of active COVID-19 infection is reported in this case report in a 70-year-old man. 54 Sheth et al. 55 reported a 52-year-old man who had RVO as a result of COVID-19 and experienced vision loss in his left eye 10 days after testing positive for SARS-CoV-2.
Retinal artery occlusions and hemorrhages, as well as cotton wool spots induced by complement-mediated thrombotic angiopathy, are all possible intraocular consequences. Miller-Fisher syndrome or infarct-related central blindness are two neuro-ophthalmological consequences that might develop in extremely uncommon situations. 41
A 59-year-old man with COVID-19 was reported to have bilateral intraretinal hemorrhage. 56
Three days after COVID-19 infection, a 66-year-old Asian man developed a vascular occlusion with panuveitis. 60 A case of unilateral panuveitis and optic neuritis as initial presentation of acute COVID-19 has been reported in a 60-year-old woman. 61 Less commonly, hemorrhagic conjunctivitis or retinal involvement might develop. 41
A COVID-19 patient with a systemic inflammatory syndrome had uveitis, erythema, and skin nodules, as well as cardiovascular (edema) signs. The anterior uveitis caused a rise in intraocular pressure that did not respond to therapeutic therapy, necessitating surgery to save the vision. This is the first case of COVID-19-related ocular hypertension to be reported. 57
In 7% of patients, patients with severe COVID-19 presented with abnormal magnetic resonance imaging (MRI) results of the globe. 62 Cavernous sinus thrombosis associated with central retinal artery occlusion in a 37-year-old male COVID-19 patient. There is no light sensitivity in the left eye, as well as optic atrophy and macular pucker. His previous medical history indicated severe pneumonia caused by a SARS-CoV-2 infection 3 months before. 63 A healthy 33-year-old male probable COVID-19 patient presented with unilateral central retinal vein occlusion (CRVO), which might be a COVID-19 consequence. 3 Four cases of suspected fungal endogenous endophthalmitis in individuals who recovered from COVID-19 have been reported which could be an example of long COVID-19 sequence of events. 58
Following COVID-19 infection, a 42-year-old Asian Indian female developed unilateral multi focal central serous retinopathy (CSCR). As a result, CSCR can develop during COVID-19 therapy due to steroid administration, and patients should be sent to an ophthalmologist as soon as possible. 64
Infection with COVID-19 causes recurrent manifestations in individuals. Infections such as endogenous endophthalmitis, candida retinitis, tubercular choroidal abscess, and bilateral pre-foveal hemorrhages were among the vision-threatening symptoms. Paracentral acute middle maculopathy, central serous chorioretinopathy, and voriconazole-induced visual complaints were among the milder signs. 65
In conclusion, long-term COVID-19 patient follow-up is recommended to identify any posterior segment manifestations that may develop over time.
Neuro-ophthalmology and neurological manifestations
Diplopia, ocular pain, and myasthenia gravis are among the reported neuro-ophthalmology signs and symptoms.66,67
Vertical diplopia has been present for 10 days in a 58-year-old male. Internuclear ophthalmoplegia was suspected based on extraocular movement testing findings. 68 Fever, cough, and headache were followed by retro-ocular pain and reading impairment in a 51-year-old woman. She was diagnosed with Adie’s syndrome and multifocal chorioretinitis. 66
Lidder et al. 69 reported the first case of a Kawasaki-like syndrome in a COVID-19-infected adult.
A 25-year-old man with no history of coagulopathy was reported to have experienced a COVID-19 cytokine storm, which resulted in Lock In Syndrome secondary to pontine strokes. 70
The neurological symptoms linked with acute COVID-19 include acute cerebellar ataxia and myoclonus (ACAM) with or without opsoclonus. 71
Myasthenia gravis has been diagnosed in a 21-year-old female COVID-19 patient. 67 Table 1 summarizes the ocular manifestations.
COVID-19 Ocular signs and symptoms.

CRA, central retinal artery; CRV, central retinal vein; FBS, foreign body sensation.
The risk factors of ocular involvement include older age, high fever, elevated neutrophil/lymphocyte ratio, and elevated levels of acute phase reactants. 81
Finally, the presence of neuro-ophthalmologic symptoms may increase the viral infection likelihood, especially if fever and respiratory symptoms are present.
Ocular COVID-19 and children
The most recent recommendations state that all individuals, including children, are generally vulnerable to SARS-CoV-2. 82 According to preliminary research, children in China are equally as likely as adults to be infected with COVID-19, although they are less likely to become symptomatic or develop severe symptoms. However, it is unknown how crucial children are in terms of viral transmission. When compared with adults, children experience greater gastrointestinal symptoms. 83
Children hospitalized with COVID-19 in Wuhan, China, had symptoms including fever, cough, and ocular signs such conjunctival discharge, eye rubbing, and conjunctival congestion, according to this cross-sectional study. Ocular symptoms were linked to patients’ systemic clinical symptoms, such as cough. Eventually, ocular problems recovered or improved. 74
A low incidence of COVID-19 infection was identified among babies in an uncontrolled case series of Brazilian newborns of women with COVID-19 infection, and none exhibited ocular abnormalities. 84
Fifteen SARS-CoV-2-positive infants had ocular symptoms. Cotton wool patches, vitreous hemorrhage, and microvascular damage appeared on fluorescein angiography as patchy choroidal filling, peripapillary hyperfluorescence, delayed retinal filling and venous laminar flow, and boxcarring in all cases. 75 From 17 April to 1 May 2020, the New York City Health Department identified 15 patients aged 2–15 years who were hospitalized in pediatric intensive care units (ICUs) with symptoms consistent with typical Kawasaki disease, incomplete Kawasaki disease, and shock. 69 A 17-year-old girl who had recently been diagnosed with COVID-19 presented with CRVO, which might have been caused by her recent COVID-19 infection. 76
In children with multisystem inflammatory syndrome (MIS-C) caused by COVID-19, bilateral non-granulomatous acute anterior and corneal punctate epitheliopathy was reported. Inflammatory ocular symptoms in MIS-C can be found as a result of COVID-19. 85 COVID-19 was evaluated in children with a mean age of 84 months; of the 27 patients, 4 (15%) were asymptomatic, 15 (56%) had respiratory symptoms, and 8 (30%) had gastrointestinal symptoms. In four patients, ocular symptoms consistent with moderate viral conjunctivitis were found (15%). COVID-19 ocular symptoms appear to have a milder clinical course in young patients than in adults in their study population. SARS-CoV-2 transmission through tears may be possible, despite the low incidence and rapid resolution of viral presence in the conjunctiva, even in patients who do not appear to have ocular involvement. 77 Late-onset rash and transient loss of taste were reported by a 15-year-old boy. Furthermore, infection with the SARS-CoV-2 virus in children and adolescents can be asymptomatic, but it can also cause fever, dry cough, tiredness, and gastrointestinal symptoms. 86 Conversely, some studies did not report any ocular manifestations of COVID-19 in children.73,87 The most common symptoms and signs in 551 COVID-19 children aged 1–17.5 years old were 53% fever, 39% cough, and 14% sore throat/pharyngeal erythema; however, 18% were asymptomatic. 73 74% of patients were administrated antivirals, six patients required invasive mechanical ventilation, and one of them died.
Future research
Only a few studies in the geriatric population and children have been published. To assess the ocular symptoms in children and geriatric patients, more retrospective studies are needed.
Conclusion
The probability of viral transmission through tears is much higher in patients with moderate to severe COVID-19. For RT-PCR tear collection, the conjunctival swab remains the gold standard. In addition, wearing eye protection when seeing patients on a daily basis during the pandemic is essential. Follicular conjunctivitis, conjunctival hyperemia, chemosis, and epiphora are the most prevalent ocular symptoms in adults. Optic neuritis, disk edema, retinal artery occlusions, intraretinal hemorrhages, cotton wool spots, and uveitis have all been reported in COVID-19 patients as posterior segment ocular manifestations. Finally, neuro-ophthalmology signs and symptoms include ocular pain, diplopia, and myasthenia gravis. Long-term follow-up is advised to determine the long-term COVID-19 ocular manifestations that may develop over time. Finally, more retrospective studies in the geriatric and pediatric populations are required.
Footnotes
Author contributions
Conflict of interest statement
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.