
Abstract
Glaucoma is a serious complication after corneal transplantation and itself a common cause for graft failure and leading cause of vision loss post-keratoplasty due to corneal endothelial decompensation. Endothelial keratoplasty procedures like Descemet stripping automated endothelial keratoplasty (DSAEK) and Descemet membrane endothelial keratoplasty (DMEK) may be superior to penetrating keratoplasty (PK) regarding the incidence of elevated intraocular pressure (IOP) and development of glaucoma. There are indications that regardless of the method of keratoplasty, some corneal diseases like pseudophakic bullous keratopathy, corneal perforation, and graft rejection have a higher risk for developing post-keratoplasty glaucoma than keratoconus and corneal dystrophies and likewise respond less to IOP lowering therapy. In this review, the pathophysiology of post-keratoplasty glaucoma, the diagnostic tools with focus on different devices, and their limitations with regard to measuring IOP and the treatment modalities are presented.
Keywords
Introduction
Glaucoma is one of the leading causes for irreversible blindness worldwide and affects more than 70 million people.1,2 It can be categorized in open-angle glaucoma and angle-closure glaucoma, and is characterized by structural damage to the optic nerve head and visual-field defects. 3 Also, glaucoma is an important complication after corneal transplantation and a common cause for graft failure and the leading cause of vision loss post-keratoplasty. 4 Other relevant complications which could occur after keratoplasty are irregular astigmatism, infections, graft decompensation, or graft rejection. Post-keratoplasty glaucoma is causing corneal endothelial decompensation and centrally decreased endothelial cell densities. 5 Corneal transplantation is one of the most frequently performed transplantation worldwide and the number is still rising. The total number of by US eye banks supplied tissue for keratoplasty was increasing up to 85,601 in 2019. Especially due to Descemet Membrane Endothelial Keratoplasty (DMEK) surgery, the endothelial keratoplasty increased 1.0% up to 30,650 in the United States, whereas the number of performed penetrating keratoplasty (PK) showed a weaker rise (0.4%) on 17,409. 6 For a long time, PK was the most widely implemented technique for corneal transplants in general. But since in developed countries Descemet stripping automated endothelial keratoplasty (DSAEK), DMEK, or laser-assisted keratoplasty became more preferred methods for several diseases such as pseudophakic bullous keratopathy or Fuchs’ corneal dystrophy, it became very important to consider the advantages and risks of each technique.5,7 An advantage of endothelial keratoplasty compared to PK concerning post-keratoplasty glaucoma is described by Kosker and colleagues and Moisseiev and colleagues, who compared the incidence of secondary glaucoma and the development of intraocular pressure (IOP) in patients with endothelial dysfunction, respectively.5,8,9 Other studies reported no significant difference between DSAEK and PK for patients with Fuchs’ dystrophy. 10 Recently, Woo and colleagues 11 highlighted the better outcome in graft rejection and IOP after DMEK in comparison with DSAEK and PK for Fuchs’ dystrophy and bullous keratopathy. Zheng and colleagues 12 recently described a glaucoma surgery rate of 6.1–9.4% without significant difference between different surgery techniques. Post-keratoplasty in general, the 10-year cumulated incidence of elevated IOP and elevated IOP requiring treatment has been described to be 46.5% and 38.7%, respectively. 13 In this comparison, endothelial keratoplasty showed a lower incidence of elevated IOP than PK. 13 Regardless of the performed method of keratoplasty, plenty of studies highlight the influence of the underlying disease on the development of post-keratoplasty glaucoma. Patients with pseudophakic bullous keratopathy, corneal perforation, and graft rejection showed a higher risk for developing post-keratoplasty glaucoma than patients with keratoconus and corneal dystrophies.14–17 Likewise, the response to medical treatment of the post-keratoplasty glaucoma for cases with keratoconus and corneal dystrophies was better than for cases with pseudophakic bullous keratopathy, corneal perforation, and herpes keratitis. 17 As pioneers in this field, Irvine and Kaufman reported as early as 1969 on increased IOP higher than 25 mm Hg in the first week postoperative after PK. They accentuated the differential incidence of 37% in phakic eyes and of 88% in aphakic eyes.7,18 Liesenborghs and colleagues 19 published a semiquantitative systematic review about risk factors for the development of ocular hypertension after keratoplasty. They identified 110 risk factors out of 76 relevant articles (1993–2019) and defined preexisting glaucoma, high preoperative IOP, and combined keratoplasty with removal or exchange of an intraocular lens (IOL) as definitely associated with an increased risk of ocular hypertension after keratoplasty. Furthermore, comparing aphakia and pseudophakia (with anterior or posterior chamber IOL) to phakic lens status, the first mentioned was also described to be definitely associated with an increased risk. Liesenborghs and colleagues 19 defined the following cases as probably associated with an increased risk of ocular hypertension after keratoplasty: glaucoma in the contralateral eye, indication of bullous keratopathy, African American descent, preoperative treatment with cyclosporine or olopatadine 0.1%, postoperative treatment with prednisolone acetate 1%, and combined surgery. Another meta-analysis from 2017 20 focusing on only post-PK glaucoma describes similar pre- and intraoperative risk factors, which largely coincide with the results of Liesenborghs and colleagues. As an evident difference, Wu and Xu 20 mentioned also trauma being an associated risk for the development of post-PK glaucoma. The cause, the mechanism, and the grade of IOP elevation after keratoplasty and its management differ between the corneal transplantation techniques and the associated preexisting anterior segment changes. 21 Sharma and colleagues 22 compared the IOP outcome after PK and DSAEK and concluded that IOP lowering treatment was significantly less needed after DSAEK during the early postoperative period, but the difference was not significant after 24 weeks.
This article reviews the current literature on definition, pathophysiology, diagnosis, and different therapy options for post-keratoplasty glaucoma including new approaches in minimally invasive surgical management (Figure 1).
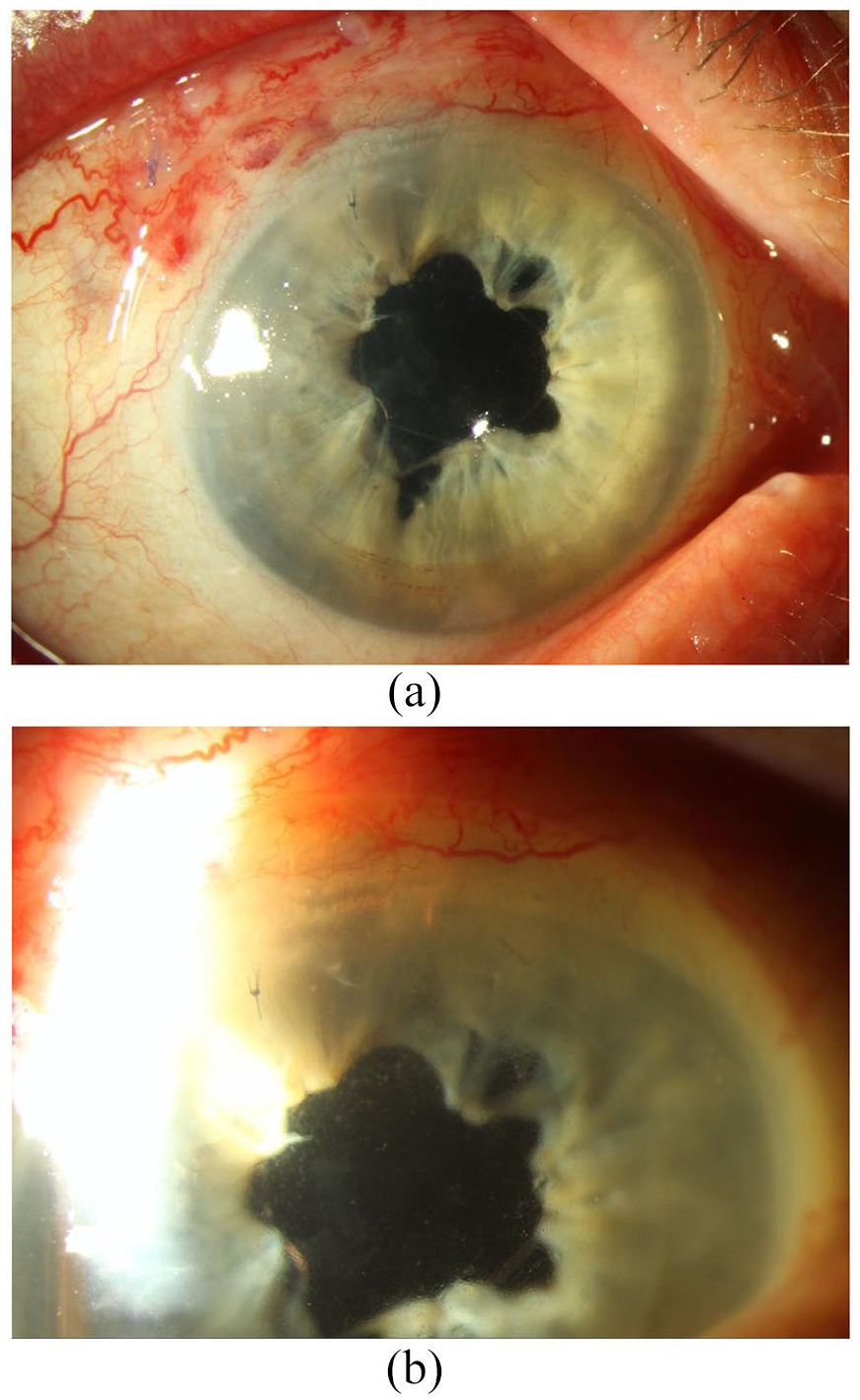
(a) Ultrathin-DSAEK in an aphakic, vitrectomized eye with reconstructed pupil. (b) Preserflo distal end is visible at 12 o’clock. DSAEK, Descemet stripping automated endothelial keratoplasty.
Definition
Glaucoma is including heterogeneous diseases having the cupping of the optic nerve head and loss of retinal ganglion cells in common. 3 The IOP is too high compared to the pressure needed to damage the optic disc and in turn leading to visual-field defects. 3 Glaucoma is highly associated with older age and it affects up to 3.5% of individuals over 40 years of age worldwide 3 Typically, symptoms only appear in advanced stages of glaucoma, when optic nerve damage has already progressed. Therefore, early diagnosis via fundoscopy, tonometry, and perimetry is of great impact. Glaucoma progression can be stopped or at least slowed down by several therapy steps such as medical and laser treatment or surgery to lower IOP around 30–50%. 3 To review the incidence of glaucoma after keratoplasty, a standardized terminology would be needed for comparison of the results of different studies. That is why the variation of prevalence for post-keratoplasty glaucoma or elevated IOP after keratoplasty ranges from 5,5% 23 to 68%. 22 A common definition for ocular hypertension after keratoplasty is an IOP greater than 21 mm Hg. This is also the only criterion used by some authors to define post-keratoplasty glaucoma; other literature added the need of surgical or medical treatment for more than 4 weeks to lower the IOP.19,20,24 Liesenborghs and colleagues 19 also mention a persistently increased IOP greater than 10 mm Hg compared to the baseline value with or without medical or surgical treatment as a widely used cutoff for post-keratoplasty glaucoma. This is specified in some papers by the conditions of visual-field loss and optic nerve head changes.17,20,23–28 A special case is the definition for cases with preexisting glaucoma, where the terminology of post-keratoplasty glaucoma is used for elevated IOP under original medication after keratoplastic surgery when adaptation of the treatment is necessary to control the IOP postoperatively. 20 Another reason for difficulties in definition of post-keratoplasty glaucoma is the variety of the timepoint of IOP measurement in published literature. An early timepoint, which includes around half of the incidence of the reported post-keratoplasty glaucoma cases, refers to an early period including 2 days to 3 months postoperatively.20,23,25,29 Liesenborghs and colleagues focused on studies with 6-month outcomes of IOP measurement. 19 In this setup, they avoid incorrect IOP data due to early postoperative fluctuations. Furthermore, the lack of widely used gold standards for IOP control after keratoplasty and other outcome measures lead to varying reports about the development of post-keratoplasty glaucoma. The reliability, the validity, as well as the sensitivity of different diagnostical approaches for IOP measurement are widely spread. 20 Goldmann applanation tonometry (GAT) is a commonly used method for IOP measurement although it is reported by Neuburger and colleagues that it could lead to underestimated IOP in corneal transplants or corneal edema. They propose the use of Tono-Pen XL and the iCare in probably edematous cornea. 30
Pathophysiology
Although the exact mechanism of post-keratoplasty glaucoma has not been discovered, several causative factors and possible mechanisms are suggested. The mechanism may also differ in this diversified clinical entity depending on previous corneal transplantation indication. An intraoperative cause for post-keratoplasty glaucoma could be the distortion of the anterior chamber angle with a collapse of the trabecular meshwork.4,5,31 This collapse can be caused intraoperatively by a loss of the anterior support afforded by Descemet’s membrane.4,32 Aphakic eyes have already preoperatively potential mechanical instability caused by the loss of fixation by the ciliary body-lens support system posterior to the angle.7,32 Other explanations for the higher incidence of post-keratoplasty glaucoma in aphakic or pseudophakic eyes could be an effect of IOL material, inflammatory reaction after surgery, and also, as described above, the influence of mechanical changes due to aphakia or pseudophakia on the peripheral anterior angle anatomy.20,29 Olson and Kaufmann attempted to explain the exceptionally high incidence of post-keratoplasty glaucoma in aphakic eyes using a mathematical model. They tried to correlate the increase in IOP with the amount of anterior chamber angle distortion. According to this model, the anterior chamber angle distortion is attributed to be aggravated by several variables, including tight suturing, long suture bites (more compressed tissue), increased peripheral corneal thickness, and same-sized donor–recipient trephination. Vice versa smaller trephine sizes, donor corneas larger than the recipient, thinner recipient corneas, and larger overall corneal diameter lead to less anterior chamber angle distortion.4,20,33 However, this clinical hypothesis was not evidentially proven until today. In general, postoperative inflammation, hemorrhage, potential steroid response, iritis, malignant glaucoma, pupillary block, or retained viscoelastic can occur after keratoplasty and cause post-keratoplasty glaucoma. 7 After DMEK, an increased IOP in early postoperative period may also occur because of air bubble–related mechanisms.34,35 A steroid-induced increase of the IOP after corneal surgery is the most common reason for ocular hypertension after keratoplasty. 19 The effect of corticosteroids acts through an elevation of the outflow resistance and thereby impeding the drainage of aqueous humor by inducing molecular transformations in the trabecular meshwork.19,36,37 Erdurmus and colleagues evaluated the frequency of steroid-induced IOP elevation, which is an important cause for late-onset post-keratoplasty glaucoma, after PK in patients with keratoconus and in patients with Fuchs’ endothelial dystrophy. These diseases are expected to have a low risk for the development of post-keratoplasty glaucoma. 38 Erdurmus and colleagues 38 reported a frequency of IOP elevation of at least 10 mm Hg over preoperative baseline of 24% in keratoconus and 20.7% in Fuchs’ cases and a frequency of IOP elevation ⩾22 mm Hg of 22% and 29.3%, respectively. Additional possible reasons for post-keratoplasty glaucoma are peripheral anterior synechiae caused by recurrent infections, vitreous prolapse, anterior mesenchymal dysgenesis, previously performed PK, posttraumatic cases, and a long-lasting hypotonic phases during surgery.23,25,39 Banitt and Lee 7 reported the difficulties of treating angle-closure glaucoma caused by peripheral anterior synechiae after keratoplasty and thus the need for surgical IOP adjustment. Gatzioufas and colleagues 40 described a significant correlation of early-onset ocular hypertension after PK in keratoconus cases with anatomical changes in the anterior chamber. Surgical stress and postoperative inflammation are reported to probably induce an increase in corneal thickness and subsequently a reduction of the anterior chamber angle. The compression of the trabecular meshwork by these changes in anterior chamber architecture is attributed to disturb the drainage of the aqueous humor.40,41 It has not yet been conclusively determined under which conditions these changes are permanently and in combination with the development of anterior synechiae leading to post-keratoplasty glaucoma. 41
Diagnosis
GAT (Haag-Streit AG, Switzerland) is actually the best established technique for IOP evaluation and is the gold standard in clinical use.5,42,43 It is described to be a robust method with a low variability intra- and interobservers.44,45 The calibration for optimal results was carried out for a mean corneal thickness of 520 µm.42,43 However, GAT is inaccurate in edematous corneas or after corneal transplantation because of its dependency on central corneal thickness (CCT), curvature, and hydration.30,42 There are various correction algorithms and nomograms to adjust the GAT results according to the corneal thickness. However, the accuracy of GAT in some biomechanical corneal properties is questionable.45,46 To get around this limitation, numerous other tonometers have been developed and put into clinical use aiming to measure IOP more accurate regardless of the biomechanical properties of the eye.30,42,46–50 The ocular response analyzer (ORA; Reichert, Inc., Depew, NY, USA) is a non-touch, air-puff-based device measuring parameter related to corneal biomechanical properties such as the corneal hysteresis (CH), which describes the viscous and elastic characteristics, and the corneal resistance factor (CRF).30,48 Based on those parameters, ORA calculates a so-called cornea-compensated intraocular pressure (IOPcc) which is reported to be less prone to failure due to abnormal CCT than GAT.48,51 Clemmensen and Hjortdal described no correlation between the IOPcc evaluated by ORA and the CCT, what is supported by other studies as well.52,53 Contrarily, one study was reporting a slight correlation of ORA measurements with increasing CCT. 54 The Pascal dynamic contour tonometer (DCT; Ziemer AG, Port, Switzerland) is measuring IOP in a non-applanation contact technique with a concave tip with pressure sensoring by contour matching with minimal corneal distortion.45,46,48,50 Therefore, it is also claimed to not be affected by corneal biomechanical properties such as corneal thickness and rigidity.45,46,48 Several studies showed an overestimated IOP measured by DCT compared to GAT measurements in post-DSAEK eyes.42,46,50,55,56 However, Clemmensen and Hjortdal 48 found that the IOP values in Fuchs’ dystrophy and post-DSAEK eyes are similar when measured by GAT and DCT but significantly higher measured by ORA. Ceruti and colleagues proposed to use DCT for IOP measurements after deep lamellar and penetrating keratoplasties having a strong correlation with GAT values in those cases. Overall, in their study, the DCT readings were 2.5 ± 1.7 mm Hg higher than the GAT values with increasing differences between the tonometers in high or low IOP ranges. 47 Yi and colleagues 50 compared the following tonometers for IOP measurement after DSAEK surgery in bullous keratopathy eyes: GAT, DCT, non-contact tonometry (NCT; Topcon Corporation, Tokyo, Japan), and Schiøtz indentation tonometry (SIT; Rudolf Riester GmbH & Co. KG, Jungingen, Germany). The latter is no standard tonometer in clinical use but rarely used in special conditions such as in children, in experiments, or because of its low costs and usability.50,57–59 Yi and colleagues 50 concluded that SIT is no reliable outcome measure after DSAEK because of high variations and extreme differences compared to the results of other tonometers. As in other studies, the DCT results are higher than those measured by GAT and NCT in post-DSAEK eyes. 50 NCT, whose advantages are no risk of infection and no need for local anesthesia, showed the lowest IOP values in their study. 50 However, GAT and NCT presented a moderate agreement at all measurement timepoints with the lowest intertonometry difference in this study. 50 This IOP correlation between GAT and NCT measurement is supported by the results of Tonnu and colleagues. 60 The handheld tonometers Tono-Pen XL (Reichert, Inc.) and iCare (iCare Finland Oy, Helsinki, Finland), which have only a small contact area with the cornea, are recommended to use in cases with corneal edema by Neuburger and colleagues. 30 However, the iCare significantly underestimated IOP compared to GAT results in post-keratoplasty and in control groups.46,49 On the contrary, the iCare was overestimating IOP in corneal edema and seemed to be less influenced by edematous eyes. 49
In the early postoperative period, the most important technique for diagnosing post-keratoplasty glaucoma is the previously described IOP measurement, whereas in later timepoints also visual-field assessment and fundus imaging gain in importance. 4 Glaucomatous optic disc changes in fundus examination are used as a diagnostic criterion for post-keratoplasty glaucoma.17,25 An adequate assessment of the optic disc is challenging, though, because of pre- and postoperative media opacification.4,25,61 For nevertheless detecting early post-keratoplasty glaucoma, Nguyen and colleagues proposed the temporal contrast sensitivity testing using full-field flicker stimulation (Erlangen flicker test) because of its independency of corneal topographic changes.5,62 For the same reason, also frequency-doubling perimetry could be useful in eyes after PK. 63 Also the frequently used automated luminance-increment, static perimetry testing is restricted by postoperative corneal distortion with irregular astigmatism.4,25 Anterior segment optical coherence tomography is described by several authors as a diagnostic method in post-keratoplasty glaucoma to penetrate opaque grafts via infrared light.5,64,65 Furthermore, visual acuity, slit-lamp examination and gonioscopy to examine the anterior chamber depth, ultrasound biomicroscopy, and non-contact specular microscopy of the graft endothelium are common diagnostic methods to evaluate patients with potential post-keratoplasty glaucoma.25,61 Several difficulties in performing fundus diagnostics, visual-field testing, and IOP assessment in post-keratoplasty patients are widely acknowledged.20,25 Therefore, the incidence and prevalence of post-keratoplasty glaucoma are supposed to be underestimated. 25
Therapy
Regardless of the technique of corneal transplantation, there is a high incidence of steroid-induced ocular hypertension or steroid-induced glaucoma after keratoplasty.38,66,67 In cases of steroid response, topical corticosteroid therapy should be reduced to the minimum required or discontinued by substituting alternatives.66–68 To minimize the corticosteroid therapy and decrease the risk of IOP elevation, less potent steroids such as fluorometholone, loteprednol, and rimexolone could be used. 69 As an alternative, Perry and colleagues described that cyclosporine A 0.5% caused a mean IOP reduction of –8.7 mm Hg, but with a potentially increased risk of immune rejection.66,70 As a second-line immunosuppressant in the management of high-risk keratoplasties, Dhaliwal and colleagues proposed topical tacrolimus 0.03% as a promising replacement for corticosteroids.66,71
The topical medical therapy remains the first-line treatment for post-keratoplasty glaucoma, independently of the technique of corneal transplantation and equally to general glaucoma medical treatment.66,68,72,73 Most cases with post-keratoplasty glaucoma respond positively to medical treatment;25,66,68,74 however, adverse side effects of some eye drops and effects on graft failure, long-term survival, and optical clarity should be discussed. The commonly used beta-adrenergic blockers, such as Timolol, may cause a decrease in corneal epithelial barrier function and dry-eye-like surface changes.5,75,76 Also alpha-2-adrenergic agonists may lead to dry eyes and allergic reactions after keratoplasty.31,72,77 Latanoprost is associated with anterior uveitis, cystoid macular edema, and may reactivate herpes simplex keratitis.78–81 The miotic pilocarpine may increase the risk of graft rejection by enlarging the permeability of the blood-aqueous barrier.7,82 The protracted topical administration of the carbonic anhydrase inhibitor dorzolamide may initiate graft decompensation in cases when corneal endothelium is compromised as reported by Konowal and colleagues.66,72,83 Generally, preservatives may also damage the corneal epithelium; that is why preservative-free drops are recommended especially after PK and in cases of other ocular surface impairments.25,66,72,84 Vajaranant and colleagues 42 reported failure of medical therapy after DSAEK and therefore the requirement for glaucoma surgery in only 0.3% of patients without preexisting glaucoma. This efficiency of the medical antiglaucomatous treatment after DSAEK is supported by Maier and colleagues, whereas Chan and colleagues found the need for standard surgery trabeculectomy with mitomycin-C in 29.4% of the cases.10,68,85 These differing results in the latter could be related to the prolonged use of high-potency steroids in 94.2% of the cases.10,68 In cases of refractive to medical treatment, early surgical intervention or combined corneal transplantation and antiglaucomatous surgeries could be a promising option, since combined surgeries did not show an increased risk of IOP elevation after transplantation. 73
Regarding surgical antiglaucomatous options, trabeculectomy is considered to be the oldest and the standard of the established glaucoma surgeries.86,87 Trabeculectomy is a filtering procedure, which is very effective in draining the aqueous humor through a penetration of the anterior chamber into subconjunctiva and thereby creating a filtering bleb. 87 It is performed with and without antimetabolites. The antimetabolite mitomycin-C has the advantage to reduce the fibrotic reaction on the surgical site and improving IOP control by remaining the fistula leaky.3,7 Compared to non-penetrating surgery, for example, canaloplasty, trabeculectomy has a higher risk for complications though it is a very effective procedure with convincing long-term IOP adjustment in glaucoma treatment in general.3,87,88 Canaloplasty is a more recent antiglaucomatous option for open-angle glaucoma, which is based on circumferential viscodilation of the Schlemm’s canal by introduction of a microcatheter and tensioning by intracanalicular suture.88–90 Compared to trabeculectomy, canaloplasty showed less postoperative hypotony and choroidal effusions and because of the non-bleb-dependency also the subconjunctival fibrosis is not such a relevant complication.88–90 Ayyala and colleagues 88 proposed to take canaloplasty into consideration especially for patients with high myopia, already taken place choroidal effusions or patients at high risk for suprachoroidal hemorrhage. Another less invasive method compared to standard trabeculectomy is the ExPRESS mini-glaucoma shunt. It is a little, non-valved device anchored stable in the anterior chamber and causing minimal intraoperative complications and inflammations while having similar efficacy as standard trabeculectomy.17,91,92 Other glaucoma drainage devices (GDDs) such as the commonly applied Ahmed or Baerveldt valves are the most frequently used surgical intervention when medication is not sufficient to control post-keratoplasty glaucoma. 7 GDDs are valved tubes reducing the IOP by conducting the aqueous humor from the eye to subconjunctival space. 3 Haddadin and colleagues reviewed a generally equivalent sufficiency of IOP regulation with tube shunts in the anterior chamber and vitreous cavity. 5 A poor graft survival of the corneal transplant is reported for GDDs because they lead to relevant changes in the protein content in the anterior chamber caused by disruption of the blood-aqueous barrier.93,94 Parihar and colleagues 95 compared conventional Ahmed valves and a pars-plana-modified variant in patients with post-PK glaucoma. They found comparable outcome measures for both techniques, but a slightly better corneal graft survival and reduced complications in pars-plana-modified Ahmed valves. 95 A more sufficient IOP control of tube shunts compared to cycloablation was described by Kirkness and colleagues as an alternative therapeutically option after the failure of medication and trabeculectomy.5,96 In cyclodestructive procedures, the goal is to decrease aqueous humor secretion by ablation of the ciliary epithelium and stroma. This leads to lower IOP and was historically the first attempted surgical intervention in cases with post-keratoplasty glaucoma. 7 Yttrium aluminum garnet (YAG) cyclocoagulation is reported to be very effective in regulating post-keratoplasty glaucoma even after a single laser application, with a success range from 66% to greater than 90%. Nevertheless, it is causing relevant complications such as inflammation, postoperative hypotony, pupillary block, hyphema, phthisis bulbi, macular edema, and graft failure.5,94,97 A tissue-sparing alternative to the standard cyclophotocoagulation is the pulsed transscleral cyclophotocoagulation. 94 The better safety profile of the pulsed transscleral cyclophotocoagulation is supposed to be due to the pause periods, which are in between the repetitive and shorter laser pulses.94,98 Subramaniam and colleagues investigated the outcomes of pulsed transscleral cyclophotocoagulation for IOP control after keratoplasty. They reported an IOP reduction of a mean of 35% after 12 months and insignificant postoperative inflammation and pain as well as unremarkable rejection episodes, endothelial cell loss, and graft failure. 94
A new and quickly expanding treatment option for mild to moderate post-keratoplasty glaucoma is the microinvasive glaucoma surgery (MIGS). MIGS is distinguished by minimal trauma, ab interno microincision, fast recovery, moderate efficacy, and high safety profile.66,99 The most common MIGS also including investigational procedures could be categorized in three target-dependent subgroups. 100 The first group targeting Schlemm’s canal and trabecular meshwork includes devices bypassing the trabecular meshwork (iStent and iStent inject; Glaukos Corp., San Clemente, CA, USA and Hydrus Microstent; Irvine, CA, USA), devices microincising the trabecular meshwork (Kahook Dual Blade; New World Medical, Rancho Cucamonga, CA, USA and Trabectome; NeoMedix Corp., Tustin, CA, USA), and devices dilating Schlemm’s canal such as ab interno canaloplasty or gonioscopy-assisted transluminal trabeculotomy (GATT) with the illuminated microcatheter iTrack (iTrack 250; Ellex, Adelaide, Australia).100,101 The second group is targeting the suprachoroidal space in order to augment uveoscleral outflow and is including CyPass device (CyPass; Alcon, Ft. Worth, TX, USA) as a first-generation apparatus and other techniques still in development (iStent Supra; San Clemente, CA, USA and MINIject device; iStar Medical, Wavre, Belgium).100,101 The CyPass implant was recalled from the global market in 2018 after a 5-year evaluation due to significant loss of corneal endothelial cells probably caused by positioning issues.100,102,103 The third group of MIGS is targeting the subconjunctival space and is including Xen gel stent (Allergan, Inc., Irvine, CA, USA), InnFocus MicroShunt (InnFocus, Inc., Miami, FL, USA), and the investigational Preserflo device (Santen Co., Osaka, Japan).100,101 In general, the advantage of MIGS compared to traditional tube systems is their smaller tube size, which is supposed to be less prone to corneal endothelial impairment. 66 However, well-designed randomized clinical trials with long-term follow-up are necessary to evaluate efficacy and safety profile over time in particular because currently MIGS is frequently performed in combination with other antiglaucomatous therapies, which impedes the specific evaluation of MIGS.100,101 Moreover, there are only single case reports describing the effects of MIGS devices in post-keratoplasty glaucoma.104,105 Rahmania and colleagues 105 analyzed in a retrospective case series Xen45 Gel Stent (Allergan plc, Dublin, Ireland) implantation in patients with post-keratoplasty glaucoma or ocular hypertension refractory to medical antiglaucomatous therapy. They reported an average IOP decrease of 70.5%, a needling rate of 20%, and as adverse events just one IOP spike on 7th postoperative day without long-term consequences. 105
In conclusion, the use of MIGS may be a promising treatment option in mild to moderate post-keratoplasty glaucoma. However, efficacy, tolerability, safety profile, and long-term follow-up in this indication need further investigation, as there are not much data supporting the use of MIGS in post-keratoplasty glaucoma. In general, topical medical therapy remains the first-line treatment for this specific glaucoma. In order to prevent steroid-induced glaucoma after keratoplasty, topical corticosteroid therapy should be minimized or replaced by alternatives. To evaluate the surgical options for post-keratoplasty glaucoma, safety profile and severity of glaucomatous changes are key and should be considered individually for each patient when deciding between trabeculectomy and less invasive methods like canaloplasty, GDD, and ExPRESS mini-glaucoma shunts. Finally, cyclodestructive procedures may be a valuable and effective option in cases where surgery is too risky.
Footnotes
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.