
Abstract
Objective:
The objective of this study was to describe the outcome of surgery for traumatic cataract and associated factors in children aged 16 years and below operated in a tertiary facility.
Methods:
This was a retrospective review of records of children who had surgery for traumatic cataract between August 2015 and August 2019. Information on biodata, preoperative visual acuity, surgical methods, complications, and postoperative visual acuity were retrieved. Data were analyzed using IBM SPSS Statistics 20.0.
Results:
Traumatic cataract accounted for 87 (14.7%) of 593 eyes operated for childhood cataract during the period. Of these, a total of 79 records were available for review. There were 56 (70.9%) males with a mean age of 10.11 (±3.39) years. All injuries were unilateral; closed globe injuries accounted for 70 (88.8%) of the cataracts and the left eye was affected in 42 (53.2%) patients. Fifty-two (67.09%) eyes had other ocular injuries apart from cataracts. The morphology of the cataract was membranous in 44 (55.7%) eyes, and 76 (96.2%) eyes had cataract surgery with intraocular lens (IOL) implantation; 39 (51.3%) of these IOLs were implanted within the capsular bag. The preoperative best corrected visual acuity was worse than 6/18 in all 79 (100%) eyes and improved to 6/18 or better in 32 (40.5%) eyes at 3 months postoperatively.
Conclusion:
Traumatic cataract accounted for less than a quarter of all childhood cataracts in our center. Majority of the eyes had successful IOLs implantation during surgery, and the best corrected visual acuity improved in a moderate proportion of these patients.
Introduction
Childhood cataract is a common cause of childhood blindness, 1 and traumatic cataract accounts for a significant proportion of these cataracts. Traumatic cataract may occur as a sequel of ocular injuries, either as the only injury or may be associated with other injuries such as corneal lacerations, hyphema, vitreous hemorrhage, and retinal detachment. Such cataracts occur following injuries from a wide range of objects. 2 Ocular injury is the leading cause of unilateral visual impairment and is reported more commonly in children and young people, especially among males. This has been attributed to their more aggressive and risky behavior, which places them at a greater risk of injuries generally.
The management of traumatic cataract can be challenging, partly due to the morphology of the cataract and the presence of other ocular injuries. In addition, the reported visual outcome following surgery varies, with many studies reporting residual moderate to severe visual impairment. In a study among 49 children in Ethiopia with an average follow-up of 1 year, postoperative visual acuity of count-fingers or better was observed in 88% of the children. 3 In Kenya, a retrospective study with a minimum follow-up of 1 month reported best corrected vision of 6/9 in 64.7% of 167 eyes. 4 The reported causes of poor postoperative visual outcome included amblyopia and retinal detachment, among other causes. 4
About a decade ago, a study of 32 eyes with traumatic cataract from our center reported good outcome in about a third of the patients. 5 The study however included both adults and children and did not provide detailed information on the outcome in the pediatric age group. Furthermore, there has been improvement in surgical expertise, techniques, and equipment over the years. Therefore, this study became necessary to provide more information on the visual outcome in children in view of the improvements in available facilities. In addition, to the best of our knowledge, this is the first series on the outcome of pediatric traumatic cataract in Nigeria.
The focus of this study is to provide information on the clinical features and surgical outcome of traumatic cataract, including associated factors, in the pediatric age group in our locality. This will provide evidence for advocacy on ocular trauma prevention and counseling of parents on what to expect after surgery, in addition to serving as an audit of our services.
Methods
This was a retrospective cross-sectional study of children aged 0–16 years operated for traumatic cataract at the University College Hospital Ibadan. The study adhered to the tenets of Helsinki. Ethical approval was obtained from the University of Ibadan—University College Hospital Ibadan Research Ethics committee (approval number: UI/EC/20/0409).
Clinical records of all the children with traumatic cataract who were seen and underwent surgery performed by any of the three pediatric ophthalmologists in the Unit between August 2015 and August 2019 were reviewed. Information on biodata, preoperative findings, details of surgery, postoperative findings, visual acuity, complications, and other ocular morbidities were collected. The inclusion criterion was a minimum of 3 months postoperative follow-up while the exclusion criterion was missing or incomplete medical records.
Preoperatively, the clinical examination included visual acuity assessment using age-appropriate methods and a slit lamp examination of the anterior segment, performed with the use of a handheld or mounted slit lamp biomicroscope. Intraocular pressure (IOP) was taken with either a Perkins tonometer under sedation with chloral hydrate (100 mg/kg) for young children or with the Goldmann applanation tonometer for older children. Gonioscopy was performed for cooperative children at the slit lamp to assess the anterior chamber angle.
The morphology and stability of the lens was assessed during slit lamp examination, after dilation with a mydriatic agent. In addition, presence of zonular dialysis, integrity of the lens capsule, and presence of vitreous in the anterior chamber were assessed. Binocular indirect ophthalmoscopy was performed to examine the posterior segment. For children whose posterior segment was difficult to view, B-scan ultrasonography was done preoperatively. All children older than 2 years had a biometry test, and the intraocular lens (IOLs) power was calculated with under-correction as appropriate for age and refractive state.
All surgeries were performed under general anesthesia using a manual small incision approach with or without a side port. Anterior vitrectomy was performed as required, and all incisions were sutured with 10/0 nylon. Subconjunctival antibiotics and steroids were administered immediately after surgery.
On the first day postoperatively, a visual acuity assessment and anterior segment slit lamp examination were performed. All patients were placed on frequent topical steroids (dexamethasone) at hourly intervals, topical antibiotics (ciprofloxacin) at 6 hourly intervals, a mydriatic (Tropicamide), dexamethasone ointment nocte, and systemic steroids at 1 mg/kg on alternate days for a maximum of eight doses. The frequent topical and oral steroid administration was to prevent excessive postoperative inflammation.
For children who developed fibrinous uveitis, the frequency of topical steroids was increased to every 30 min and repeat subconjunctival steroid injections were given as required. Furthermore, frequent dilation of the pupil with phenylephrine was done to encourage fibrin retraction and prevent posterior synechiae. All children spent a minimum of 5 days on admission to ensure proper instillation of eye drops in the early postoperative period and thereby reduce immediate postoperative complications. At discharge, visual acuity assessment, anterior segment examination, IOP measurement, and posterior segment examination were performed on all children.
Follow-up visits were scheduled at a week after discharge, then monthly till 3 months postoperatively with gradual tapering off of steroids as appropriate. In a few individuals, follow-up was more frequent due to presence of other morbidities or postoperative complications such as fibrinous uveitis and elevated IOP. Additional medications were given in such children, as necessary. Refraction was done within the first 3 months after surgery and spectacles dispensed. For the purpose of this study, successful outcome was defined as successful primary implantation of an IOL and postoperative visual acuity of 6/18 or better.
Data were entered into IBM SPSS Statistics 20.0, then cleaned and analyzed. Descriptive summary statistics were computed for quantitative and qualitative variables such as age, gender, cataract type, surgery type, postoperative visual acuity, and so on. Tests of association were performed using chi-square for categorical variables and t test for continuous variables with statistical significance set at a p value < 0.05.
Results
Traumatic cataract accounted for 87 (14.7%) of 593 eyes operated for childhood cataract within the 4-year period. Of these, a total of 79 (90.8%) children’s clinical records were available for review. Males were 56 (70.9%), the age range was from 1 year to 16 years with a mean of 10.11 (±3.39) years. Eight (10.1%) children were aged 1–5 years, 28 (35.4%) were aged 6–10 years, while 43(54.4%) were aged between 11 and 16 years.
All the injuries were unilateral and the left eye was affected in 42 (53.2%) of the children. The time interval between injury and presentation was 3 months or less in 25 (31.6%) of the children and more than 3 months in 54 (68.4%), with a mean duration of 19.7 months and a range of 5 days to 11 years. The place of residence was Ibadan, the city where the hospital is located, for 25 (31.6%) of the patients while the other children resided within 1–3 hours of travel from Ibadan except for 1 (1.3%) child who resided in Edo state which is about 5 hours away (Figure 1).
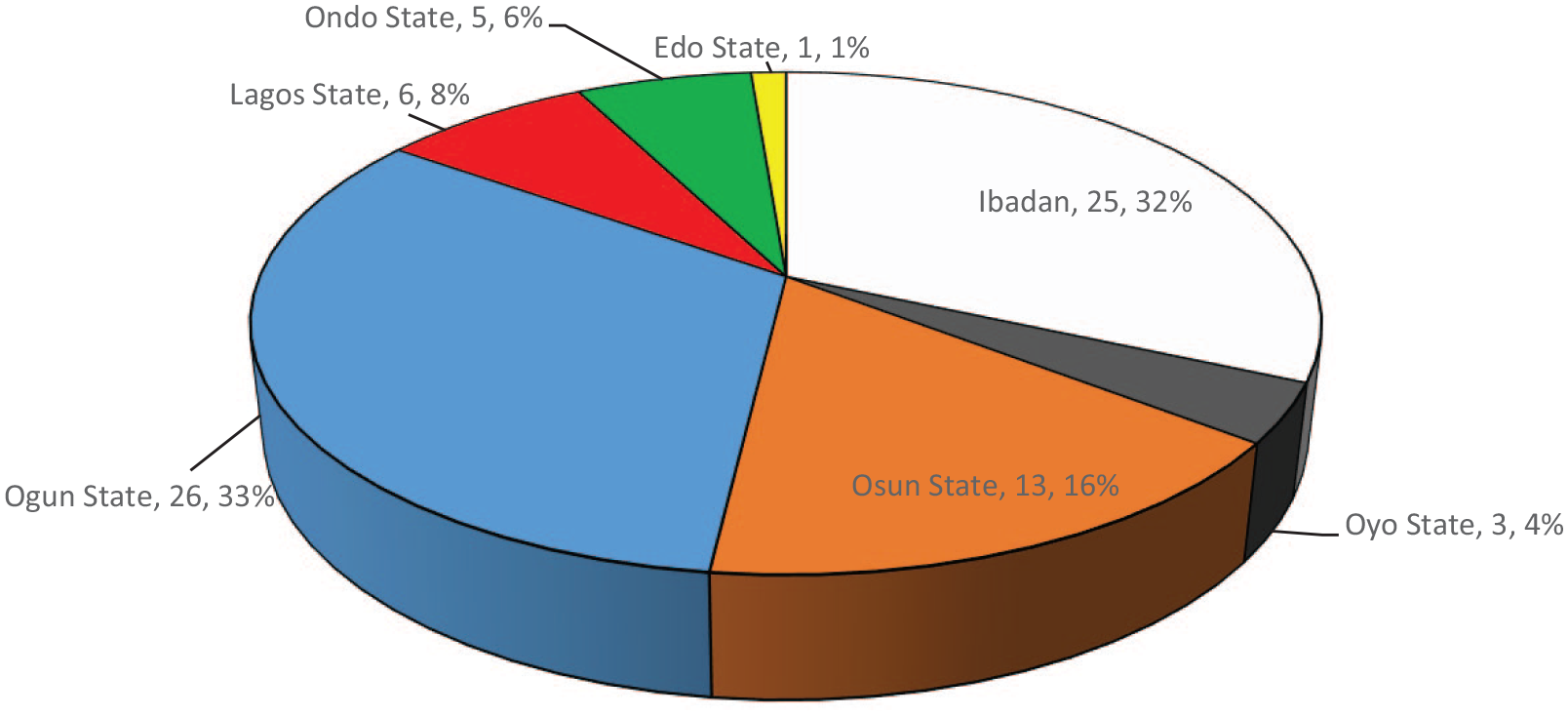
Place of residence of 79 children with traumatic cataract.
The preoperative visual acuity (VA) was worse than 6/18 in all (100%) of the 79 eyes; 66 (83.5%) eyes had VA worse than 1/60, 5 (6.3%) eyes had VA between 3/60 and 1/60, while 8 (10.11%) eyes had VA between 6/24 and 6/60. The morphology of the cataract was membranous/partially absorbed in 43 (54.4%), full cataract in 32 (40.5%), anterior capsular cataract in 2 (2.5%), milky in 1 (1.3%), and cortical opacity in 1 (1.3%). The membranous cataracts had anterior capsule calcification in 17 (39.53%) eyes and posterior capsule fibrosis in 14 (32.56%) eyes. Other preoperative findings are as shown in Table 1.
Preoperative ocular findings among 79 eyes with traumatic cataract.

Small incision cataract surgery with posterior chamber IOLs insertion (SICS + PCIOL) was performed in 76 (96.2%) of the patients, SICS without IOL in 2 (2.5%), and lensectomy without IOL in 1(1.3%). Other surgical details and intraoperative findings are as shown in Table 2. Fibrinous uveitis occurred in 17 (21.5%) eyes after surgery. Fourteen (22.95%) of 61 eyes with polymethyl methacrylate (PMMA) IOL and 3 (20%) of 15 eyes with foldable IOL had fibrinous uveitis. This difference was not statistically significant (p = 0.50). The postoperative IOP was >21 mmHg in 29 (36.77%) eyes in the immediate postoperative period and >21 mmHg in 7 (8.9%) eyes at 3 months’ postoperative period. All children with IOP greater than 25 mmHg were treated with anti-glaucoma medications during the period of this study.
Surgical details and complications in 79 eyes with traumatic cataract.

PMMA, polymethyl methacrylate.
Six eyes (7.6%) of six children underwent more than one surgery for postoperative complications and other ocular injuries from the primary trauma. These surgeries were IOL redialing, 2 (33.3%); scleral buckle, 1 (16.7%); surgical capsulectomy, 1 (16.7%); wound re-suturing with anterior vitrectomy, 1 (16.7%); and intravitreal antibiotics for postoperative endophthalmitis, 1 (16.7%).
The best corrected postoperative visual acuity (BCVA) in the immediate postoperative period (at discharge from hospital) was ⩾6/18 in 4 (5.1%) eyes and was ⩾6/18 in 32 (40.5%) eyes by 3 months after surgery (Figure 2). Identifiable factors that were considered responsible for poor postoperative visual acuity in the immediate postoperative period included posterior capsule opacity in 31 (39.2%), amblyopia in 10 (12.7%) eyes, severe uveitis in 7 (8.9%), corneal opacity in 5 (6.3%), vitreous hemorrhage in 3 (3.8%), and retinal detachment in 2 (2.5%) eyes. Out of the 31 children with posterior capsule opacity, 10 (32.26%) had Nd:YAG capsulotomy during the time of this study and 1 (3.23%) had surgical capsulectomy. At the third month postoperatively, the best corrected visual acuity was less than 6/18 in 47 (59.5%) eyes. The identifiable cause of poor vision was documented in 41 of these eyes and included posterior capsule opacity in 20 (48.9%) eyes, amblyopia in 10 (24.4%) eyes, cornea opacity in 5 (12.2%) eyes, vitreous hemorrhage in 3 (7.3%), retinal detachment in 2 (4.8%), and endophthalmitis in 1 (2.4%) eye.

Postoperative BCVA.
Further analysis showed that a greater proportion of the children who presented within 3 months of injury had a visual acuity ⩾6/18 at 3 months after surgery compared with those who presented later. This difference was, however, not statistically significant (Table 3). In addition, children with membranous cataract were about 3 times less likely to have a visual acuity ⩾6/18 at 3 months after surgery (p = 0.01). On the other hand, the type of eye injury and the occurrence of fibrinous uveitis were not associated with visual outcome at 3 months (Table 3).
Factors associated with successful visual outcome at 3 months among 79 patients with traumatic cataracts.

CI, confidence interval.
Fisher’s exact test.
Note. Bold values signifies p<0.05.
Discussion
Traumatic cataract accounted for less than a quarter of all the eyes operated for childhood cataract within the study period (14.7%). This is much less than previous reports from other African countries: Ethiopia, 63%; 6 Zambia, 25%; 7 and Madagascar, 26%. 8 It is also lower than previous reports from Asia (24%) 9 and Europe (20%). 10 Our finding may suggest that trauma is not a major cause of pediatric cataract in our setting. However, it might be due to poor access and uptake of care following ocular trauma. The dearth of literature from Nigeria on traumatic pediatric cataract made comparison with local data difficult. Nevertheless, to the best of our knowledge, this is the first series on outcome of traumatic cataract in children from Nigeria.
Majority of the patients were males, similar to findings from other studies.4,11,12 The mean age at presentation was 10 years with the youngest being 1 year old. This demonstrates that traumatic cataract can present at any age, and sometimes parents may be unaware as shown in our study where only about a third of the parents initially volunteered a history of trauma without the need for probing questions.
Furthermore, majority of the patients presented after 3 months of sustaining the injury. This late presentation has been observed for all forms of childhood cataract in low- and middle-income countries.13–15 In addition, we found that children who presented late appeared less likely to have a good visual outcome. Late presentation has also been reported as one of the main reasons for poor outcome of cataract surgery in children.16,17 All the patients had visual acuity worse than 6/18 at presentation, with more than two thirds of them presenting blind. This is similar to reports from Kenya 4 and India 18 where most of the children were blind at presentation.
Closed globe injury was more common in our series as a cause of traumatic cataract. This is similar to a study in Ethiopia 3 but contrary to reports from rural India 19 and China 11 were most of the cataracts were due to open globe injury. This difference may simply be a reflection of the epidemiology of pediatric ocular injury in our environment. Previous studies in Northern 20 and Eastern 21 Nigeria show that closed globe injuries are more common in children.
The objects that caused the injuries were of a wide variety including sticks, belts, broomsticks, door handles, belt, and broken bottles. This is similar to earlier reports from Nigeria and India5,20,22 showing that a wide variety of objects cause ocular injuries. However, in India other objects like firecrackers, bows, and arrows were reported, which did not feature in our series. Notwithstanding, it is important to ensure supervision of children while at play. In addition, corporal punishment should be discouraged as some children got injured in their eyes while being punished by teachers and caretakers.
There were a range of associated ocular injuries with the most severe morbidities being corneal scars, angle recession with elevated IOP, and retinal detachment. Two of the patients presented with corneal lacerations that needed suturing at time of cataract surgery. These findings are similar to findings by Ram and colleagues, 22 Bekibele and Fasina, 5 and Gradin and Yorston. 4 Furthermore, some of the cataracts were associated with preexisting ruptured lens capsule, zonular dialysis, and posterior capsule plaques. These associated features added more technical complexity to the surgery.
More than half of the patients had membranous/partially absorbed cataract in which the anterior and posterior capsules were partially or completely adherent while more than a third had full cataracts. This proportion of membranous cataracts is more than that noted by a study in India where membranous cataract accounted for 12% of the morphological types of traumatic cataract. 23 Membranous morphology makes implantation of an IOL very challenging as it makes it difficult to perform a good capsulorrhexis/capsulotomy. Furthermore, our results show that it is associated with poorer visual outcome similar to findings from a previous study. 23
Almost all the eyes (96.2%) had small incision cataract surgery with implantation of IOL. Other studies have reported successful IOL implantation ranging from 65%–100%.4,23,24 We consider IOL implantation to be a successful outcome of surgery as it is easier to rehabilitate uni-ocular cataracts with IOL insertion than with the use of contact lenses especially in settings like ours where contact lenses are not readily available. In addition, visual rehabilitation with contact lens poses a great challenge in our locality in terms of affordability, acceptability, and hygiene. Single piece polymethyl methacrylate (PMMA) IOL was inserted in two-thirds of the eyes and was implanted either in the capsular bag or sulcus while less than a third had a foldable acrylic lens inserted into capsular bag. PMMA IOL was similarly reported in some earlier studies4,25 as the most frequently used type of IOL.
Fibrinous uveitis was a common postoperative complication similar to earlier reports.4,18,26 Furthermore, the occurrence of fibrinous uveitis was similar among those implanted with PMMA and foldable IOL. As such, fibrinous uveitis is an important complication to watch out for in children with pigmented iris after surgery for traumatic cataract with lens implantation. Most surgeries were performed at least 3 months after the primary injuries, and thus the inflammation noticed in these patients could be attributed mainly to the cataract surgery and not the primary ocular injury.
Furthermore, a third of the patients had primary posterior capsulotomy and vitrectomy for management of the posterior capsule. In Kenya, anterior vitrectomy was similarly performed in 30% of their patients. 4 Intraoperative management of posterior capsule and anterior vitreous in pediatric cataract is a very important component to improve outcome and prevent visual axis opacification. In addition, appropriate management of vitreous loss from a ruptured posterior capsule reduces the risk of retinal detachment after surgery. None of the patients in this series had retinal detachment as a complication of surgery as at 3 months postoperative follow-up.
A few children (7.6%) had a second surgery in the same eye to treat other morbidities such as retinal detachment. The rate of second surgeries in our series is less than the 30% reported by Shah and colleagues 19 in India; however, they had more eyes with open globe injury. Second surgeries increase the cost of care and number of visits to the hospital for such families. In counseling parents of children with traumatic cataracts, it is important to discuss the likelihood of multiple surgeries, however small the probability, so that they are prepared, especially in settings were out of pocket payment for health is more common, like ours.
The best corrected visual acuity was ⩾6/18 in 41% of the eyes and ⩾6/60 in 64% of the eyes by the third month post surgery. There was improvement in visual acuity in a large number of the eyes between the immediate postoperative period and 3 months after surgery. This gives a good outlook as we believe that with longer follow-up and active visual rehabilitation, more children will achieve improvement in vision. A previous report from Nigeria 5 reported BCVA of 6/18 or better in 35% of the eyes and another from Kenya 4 reported better than 6/18 in 64.7%. Similarly, from India, Shah and colleagues 19 reported 6/12 or better in 35.33% at 6 weeks, Eckstein and colleagues 27 reported 6/12 or better in 67% at 3 years, and Memon and colleagues 18 reported 6/18 or better in 70% at 6 months. It is important to note that there is some variation in the duration of follow-up across these studies, which makes comparison of visual outcome difficult.
Overall, there was good visual outcome in a significant proportion of the children and we attribute this to improved surgical techniques and optical rehabilitation with intra-ocular lenses. However, some of the eyes had residual visual impairment which may be due to amblyopia from delayed presentation and other associated ocular injuries noted in a subset of the children. It is therefore important to prioritize ocular injury prevention in order to reduce childhood blindness from ocular injury
Conclusion
Traumatic cataract accounted for less than a quarter of all childhood cataracts in our center. Majority of the eyes had successful IOL implantation at surgery, and the best corrected visual acuity improved in a moderate proportion of these patients during postoperative follow-up. Overall, there was good surgical outcome in a significant proportion of the patients.
Footnotes
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.