
Abstract
Purpose:
To determine the role of microvascular endothelial dysfunction as risk factor for primary open angle glaucoma.
Methods:
A cross-sectional study was conducted involving 114 Malay patients with POAG seen at the eye clinic of Hospital Universiti Sains Malaysia. Patients aged between 40 and 80 years who were diagnosed with other types of glaucoma, previous glaucoma filtering surgery or other surgeries except uncomplicated cataract surgery and pterygium surgery were excluded. A total of 101 patients who were followed up for dry eyes, age-related cataracts or post cataracts extraction surgery were recruited as control subjects. Those with family history of glaucoma or glaucoma suspect were excluded. Microvascular endothelial function was assessed using laser Doppler fluximetry and the process of iontophoresis. Iontophoresis with acetylcholine (ACh) and sodium nitroprusside (SNP) was used to measure microvascular endothelium-dependent and endothelium-independent vasodilatations, respectively.
Results:
In general, POAG patients demonstrated lower ACh% and AChmax values compared with controls. There was significant difference in microvascular endothelial function [ACh%: mean, 95% confidence interval = 503.1 (378.0, 628.3), and AChmax: mean, 95% confidence interval = 36.8 (30.2, 43.5)] between primary open angle glaucoma cases (p < 0.001) and controls [ACh%: mean, 95% confidence interval = 1378.4 (1245.4, 1511.3), and AChmax: mean, 95% confidence interval = 79.2 (72.1, 86.2)]; this difference remained significant even after controlling for potential confounders. Similar difference was also found in SNP% and SNPmax between POAG and controls (p < 0.001). Age and diastolic blood pressure were inversely correlated with microvascular endothelial function.
Conclusion:
There was an impairment of microvascular endothelial function and endothelial-independent vasodilatation in POAG patients. Microvascular endothelial function is a potential risk factor for POAG.
Introduction
The pathogenesis of glaucoma is still unclear today. Mechanical and vascular theories have been proposed.1,2 Although glaucoma is generally associated with increased intraocular pressure (IOP), nearly one-third to one-half of patients with primary open angle glaucoma (POAG) consistently has IOPs within the normal range of less than 22 mmHg.3–5
The increased prevalence of vascular disorders in patients with glaucoma suggests that this condition is an ocular manifestation of a generalized vascular defect.6,7 This is supported by evidence of functional abnormalities in both the systemic8,9 and the ocular10,11 circulations of patients with glaucoma.
A pressure independent mechanism has been proposed, holding the imbalance of optic nerve head (ONH) perfusion responsible for ischaemia in the retinal nerve fibre layer (RNFL).12,13 However, perfusion pressure is more dynamic and affected by the resistance to flow. It is regulated by the size (calibre) of the vessel lumen. 14 Autoregulation is believed to be responsible for maintaining ONH perfusion.15,16 Ischaemia, or vascular dysregulation, is believed to occur because of an imbalance between nitric oxide (NO) (vasodilator) and endothelin-1 (vasoconstrictor) released from the vascular endothelium. 17
Microvascular endothelial function can be assessed using laser Doppler fluximetry (LDF) and the process of iontophoresis, using an endothelial-dependent vasodilator such as acetylcholine (ACh) with an endothelium-independent vasodilator such as sodium nitroprusside (SNP). LDF is a noninvasive device used to assess changes in tissue microcirculation blood flow.
There is minimal knowledge on glaucoma in Malays. Based on a retrospective review, Malays with primary angle closure were found to progress faster than Chinese patients in Malaysia. 18 In addition, there were evidences of the effect of ethnicity on clinical presentation of glaucoma.19,20 The objective of this study was to determine the association between microvascular endothelial dysfunction and POAG in Malay patients. Factors affecting microvascular endothelial dysfunction in Malay patients were also evaluated.
Methods
A cross-sectional study was conducted involving 114 Malay patients diagnosed with POAG and 101 controls between 40 and 80 years. POAG patients and controls were recruited from the glaucoma clinic of Hospital University Sains Malaysia (HUSM). Written consent was obtained after full explanation was given to patients and controls. This study received approval from the research and ethics committee of the School of Medical Sciences, Universiti Sains Malaysia (USMKK/PPP/JEPeM (234.3) 12 ), and was conducted in accordance to Declaration of Helsinki for human research.
Patients who were diagnosed with any other glaucoma, for example, steroid-induced, pseudoexfoliative and pigmentary glaucoma, were excluded. Those with underlying ocular conditions which may interfere with POAG diagnosis, for example, media opacities including cataract, vitreous haemorrhage, post pan-retinal photocoagulation, tilted disc and retinal disease, were also excluded. Mainly, control patients were those that were examined or followed up for dry eyes, age-related cataracts or post cataracts extraction surgery. Control patients with any type of glaucoma or family history of glaucoma were excluded. Patients and controls with peripheral vascular disease or other conditions like sickle cell anaemia, known to influence vascular function,21–23 were also excluded. Systemic inflammatory diseases such as rheumatoid arthritis, inflammatory bowel diseases, lupus, psoriasis and spondyloarthritis manifest endothelial dysfunction. 24 Patients and control subjects with systemic inflammatory diseases were not enrolled in this study. Subjects with scar marks or burns on the forearm that could affect the assessment of microvascular endothelial function were excluded. Malays in this study were based on article 160 25 of the Malaysian constitution.
Upon arrival at the laboratory for study measurements, the recruited subjects were asked to empty their pockets and remove their shoes to be weighted for body mass index (BMI) calculation. A weighing machine (SECA 789, Germany) was used to measure body weight in kilograms. Their height was also measured using the flip board that was attached to the weighing machine. BMI was calculated by dividing the patient’s weight in kilograms by the square of his or her height in metres (kg/m2).
The recruited subjects were asked to rest for 10 min prior to measurement of their blood pressure (BP). The brachial BP (systolic and diastolic pressure) was measured using an automated BP sphygmomanometer (MX3, Omron, Japan) on the right arm of the recruited subjects. Measurements were taken twice with a 5-min interval between the measurements. The average of the two BP measurements was recorded.
The recruited subjects were asked to fast in order to obtain the fasting blood sugar (FBS) and fasting lipid profile (FLP). Venesection was conducted from medial cubital vein. If the recruited subjects were known to have diabetes mellitus and hyperlipidaemia, the latest FBS and FLP were traced from their medical record. However, if the latest level of FBS and FLP was done more than 3 months ago, the latest level was then obtained during this visit. Venesection was also conducted for those without any known medical history of diabetes mellitus and hyperlipidaemia.
Microvascular endothelial function was evaluated using LDF and the process of iontophoresis, the procedures of which have been reported.26,27 Briefly LDF is a noninvasive instrument employed to monitor changes in peripheral circulation. 28 This device operates based on the backscattering of laser light. Monochromatic infrared laser beam with the wavelength of 780 nm is widely used to illuminate the microvascular bed. 29 This beam is delivered to the skin or tissue via flexible optical fibre or also known as probe. As the beam passes through the tissue, the beam undergoes changes in wavelength as it hits moving blood cells (Figure 1). This change is called as Doppler shifts. 28 The wavelength shift produced is captured by the photo detector. This signal is then processed by computer software to determine the amount of the frequency shifted. 30 The magnitude and frequency distribution of these changes in wavelength are related to the number and velocity of red blood cells. 31 The laser light penetrates cutaneous microcirculation and measures 1–1.5 mm of skin depth. 32 Thus, the measurement of underlying compartment predominantly consists of the reflection from the thermoregulatory perfusion in arterioles, venous plexuses and arterio-venous anastomosis.33,34

Schematic illustration of a typical laser Doppler probe and light patterns in a skin microvascular bed.
Iontophoresis is a noninvasive method to introduce charged substances through the skin with a small electrical current, to evaluate both endothelium-dependent and endothelium-independent vasodilatations. Iontophoresis of ACh tests endothelium-dependent vasodilatory function, while iontophoresis of a NO donor, SNP, is used to test endothelium-independent vasodilatation.
The recruited patients and control subjects were requested to fast, and refrain from consuming caffeinated drinks or beverages, and food with high salt content at least 12 h before the procedure. Two iontophoresis chambers were attached to the surface of the forearm using double adhesive discs to simultaneously deliver Ach (Fluka Chemie Gmbh, Japan) and SNP (Riedel-de Haen, C.O.O. Switzerland) to the skin. The chambers were positioned at least 5 cm apart so that vasoactive response at one site would not influence the other site. Each chamber was then filled with 1% of 0.4 ml of ACh or SNP, respectively, using a micropipette. A dual-channel DRT4 LDF (Moor Instruments, Axminster, UK) with DP1T-V2 laser probes (Moor Instruments) was used in this study. Laser Doppler probes were carefully inserted with minimal pressure into the chambers. An iontophoresis protocol of five current pulses (lasting 2 min each) separated by 1-min current-free intervals was used. 26 A current strength of 0.007 mA, density of 0.01 mA/cm2 and charge density of 6 mC/cm2 were used. 26 Skin perfusion responses to iontophoresis were measured using the following parameters:

The primary parameters used to assess microvascular endothelial function are percent change in perfusion due to Ach iontophoresis (ACh%) and maximum absolute change in perfusion due to Ach iontophoresis (AChmax)
Prior to starting the study, to ensure reliability of the measurements, intra-day and inter-day coefficient of variation (CV) were measured for both ACh% and AChmax on 10 healthy subjects. The intra-day and inter-day CV was 13.4% and 13.0% for ACh%, and 11.6% and 12.5%, respectively, for AChmax, all microvascular. Measurements were made by a single operator (S.M.I.B.) throughout this study and the protocols were standardized throughout the study.
Data in this study were analyzed using SPSS version 22.0 software. The difference in demographic data and clinical presentation between POAG and controls was determined using Fisher’s exact test for categorical data and independent t test for numerical data. To determine the potential role of microvascular endothelial function as part of pathogenesis of POAG, multiple analysis of variance (MANOVA) and multiple analysis of covariance (MANCOVA) were used. Factors previously reported to affect microvascular endothelial function include age, sex, BMI, haematocrit %, total cholesterol levels, FBS levels, diabetes, hypertension and hyperlipidaemia. These were used as covariates for endothelial dysfunction. Simple linear regression and multiple linear regressions were applied for covariates.
Results
A total of 215 Malay subjects (114 POAG patients, 101 controls) were recruited. The mean IOP of 114 POAG patients at the recruitment period was 15.0 (3.6) mmHg. The mean RNFL thickness was 66.6 (15.5) µm (Table 1). Based on Humphrey visual field (HVF) assessment, the mean for mean deviation (MD) was −11.1 (8.9) at the recruitment period (Table 1). Majority of the recruited POAG patients were in the mild stage of the disease (55, 48.2%), while 25.4% were moderate and 26.3% were severe. Malay patients with POAG were older than the controls. However, there was no significant difference in age and sex between the two groups (Table 2). There were significantly higher number of POAG patients with systemic hypertension compared with controls (Table 2), and because of this, POAG patients have higher SBP and DBP as compared with controls (Table 2).
Demographic data and clinical characteristic of POAG and controls.

BMI, body mass index; DBP, diastolic blood pressure; FBS, fasting blood sugar; POAG, primary open angle glaucoma; SBP, systolic blood pressure.
p < .05 is considered statistical significance based on independent t test.
p < .05 is considered statistical significant based on Fisher’s exact test. Bold is for p-value that seem significant.
Microvascular endothelial function in Malay patients with POAG and controls.
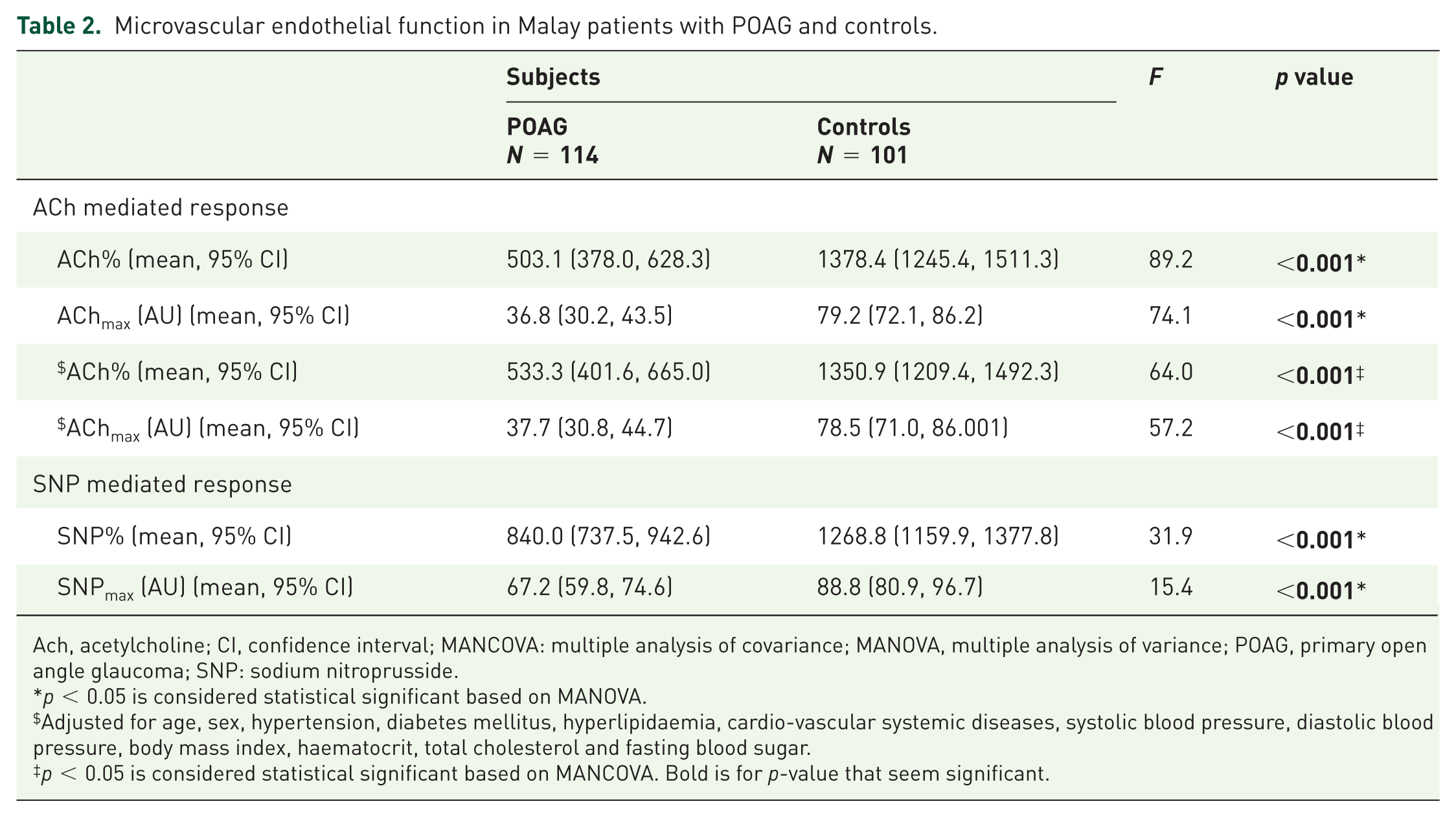
Ach, acetylcholine; CI, confidence interval; MANCOVA: multiple analysis of covariance; MANOVA, multiple analysis of variance; POAG, primary open angle glaucoma; SNP: sodium nitroprusside.
p < 0.05 is considered statistical significant based on MANOVA.
Adjusted for age, sex, hypertension, diabetes mellitus, hyperlipidaemia, cardio-vascular systemic diseases, systolic blood pressure, diastolic blood pressure, body mass index, haematocrit, total cholesterol and fasting blood sugar.
p < 0.05 is considered statistical significant based on MANCOVA. Bold is for p-value that seem significant.
There was a statistical significant difference in ACh and SNP mediated responses between POAG and control subjects (Table 2). POAG patients showed significant reduction in ACh% and AChmax (Table 2). Even after adjustment for confounding factors, there was still a statistically significant difference between controls and POAG patients for ACh% and AChmax (Table 2). Confounding factors that were included in the analysis are age, sex, hypertension, diabetes mellitus, hyperlipidaemia, cardio-vascular systemic diseases, systolic BP, diastolic BP, BMI, haematocrit, total cholesterol and FBS.
Age, systolic, diastolic BP and sex were identified as potential factors affecting microvascular endothelial function in simple linear regression (Tables 3 and 4). Based on multiple linear regressions, age and diastolic BP were found as significant factors affecting microvascular endothelial function in Malay subjects (Table 5). There was a negative linear relationship between age and ACh%. For every 1 year increase in age, there is a 15-fold [95% confidence interval (CI) = (−26.12, −3.37); p = 0.011] decrease in ACh% (Table 5). Diastolic BP of the recruited subjects showed negative linear relationship with ACh%. For every 1 mmHg increase in diastolic BP, there is a 13-fold [95% CI = (−26.64, −0.19); p = 0.018] decrease in ACh% (Table 5).
Simple linear regression between predictors affecting ACh%.
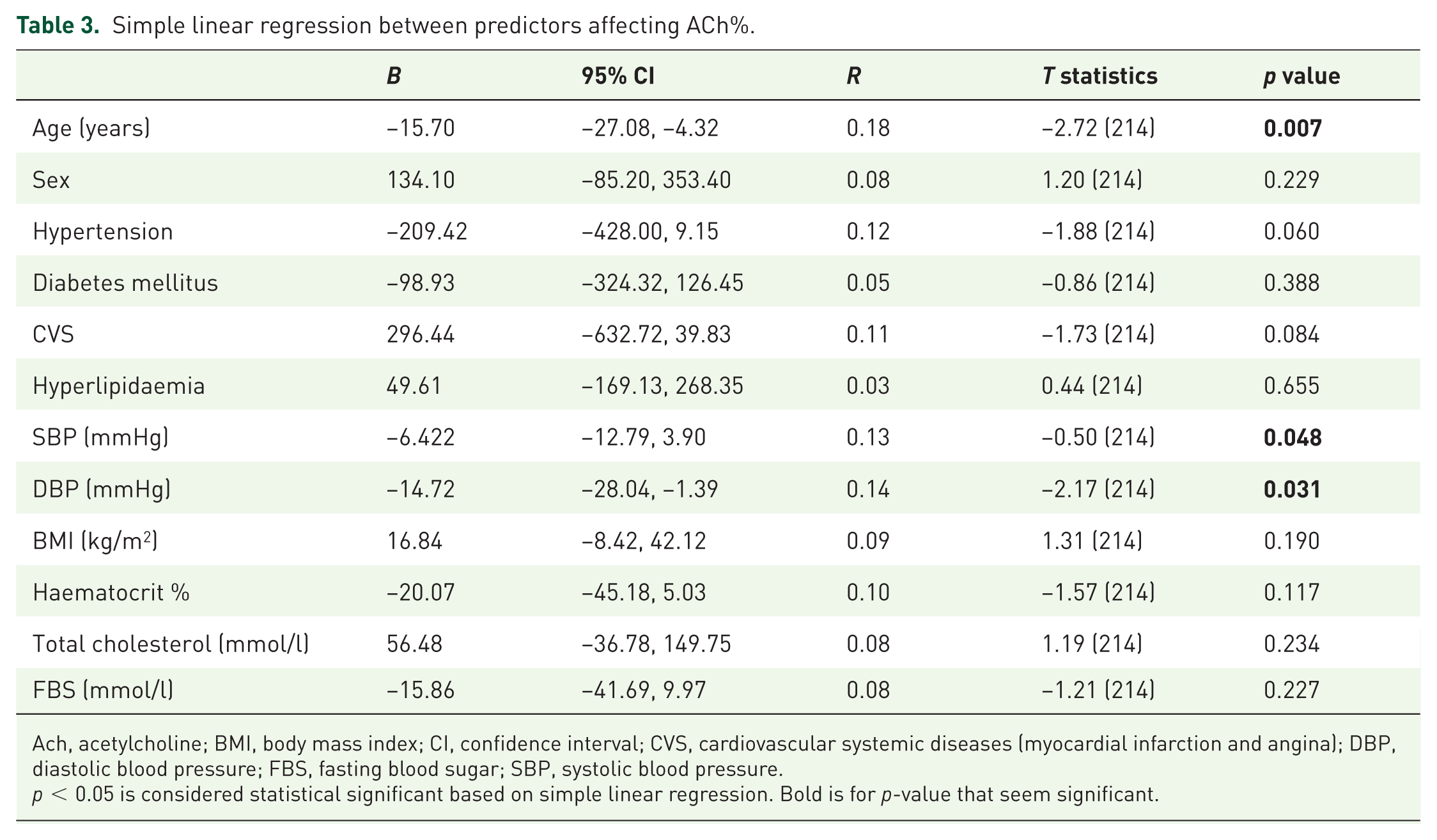
Ach, acetylcholine; BMI, body mass index; CI, confidence interval; CVS, cardiovascular systemic diseases (myocardial infarction and angina); DBP, diastolic blood pressure; FBS, fasting blood sugar; SBP, systolic blood pressure.
p < 0.05 is considered statistical significant based on simple linear regression. Bold is for p-value that seem significant.
Simple linear regression between predictors affecting AChmax.

Ach, acetylcholine; BMI, body mass index; CI, confidence interval; CVS, cardiovascular systemic diseases (myocardial infarction and angina); DBP, diastolic blood pressure; FBS, fasting blood sugar; SBP, systolic blood pressure.
p < 0.05 is considered statistical significant based on simple linear regression. Values which are significant at p<0.05 are shown in Bold.
Multiple linear regression of predictors affecting ACh% and AChmax.

Ach, acetylcholine; B: adjusted regression coefficient; CI, confidence interval; DBP, diastolic blood pressure.
Backward multiple linear regression method applied. Model assumption is fulfilled. There was no interaction among independent variables. No multicollinearity detected.
p < 0.05 is considered statistical significant based on multiple linear regression. Bold is for p-value that seem significant.
Discussion
In this study, the results indicate that microvascular endothelial function may play a role in the pathogenesis of POAG in Malay patients; Malay patients with POAG have significant reduction of microvascular endothelial function. Vasodilatory response to ACh assesses functional ability of the endothelium to produce the vasodilator NO, which diffuses to the underlying vascular smooth muscle, causing relaxation. Vascular response to SNP assesses endothelium-independent vasodilation, impairment of which may be associated with alterations in vascular smooth muscle cells or structural vascular alterations.
Both endothelium-dependent and endothelium-independent vasodilatations can be impaired in individuals with cardiovascular diseases.35,36 In the pathogenesis of vascular diseases, generally endothelial dysfunction precedes the development of structural changes, and frank vasculopathy. As the disease progressed and prolonged, it is possible that both endothelial-dependent and endothelium-independent vasodilatations are blunted. 35 In this study, vasodilatory response to SNP (endothelial-independent vasodilatation) is also impaired in POAG patients, compared with controls. However, the degree of impairment appears to be much greater in the AChmax response (2.15-fold reduction) compared with the reduction in SNPmax response (1.32-fold reduction). This may suggest that defects in the endothelium-dependent rather than endothelium-independent responses are more predominant in our POAG patients.
We are not aware of other similar studies conducted to compare microvascular endothelial function in vivo in POAG and control subjects. However, two previous authors had studied macrovascular endothelial function (using brachial artery and the process of flow mediated dilatation), which found similar association of vascular endothelial dysfunction with susceptibility to POAG development in a different population.17,37 These techniques assessed macrovascular endothelial function.
On contrary, there was evidence to suggest negative role of microvascular endothelial function in glaucoma. Buckley and associates monitored endothelium-dependent relaxation in 11 glaucoma patients and 12 healthy normal controls. 38 There was no difference in endothelium-dependent relaxation suggestive of absence of microvascular endothelial dysfunction. However, this was an in vitro study (compared with ours, which is an in vivo study), using arteries dissected from gluteal fat biopsies involving small number of patients. A recent study conducted on a smaller number of glaucoma patients also found no difference in endothelium-dependent vasodilatation response in glaucoma and controls. 39 Their result was most likely confounded by the small number of recruited subjects in their study (20 POAG and 30 healthy controls). The results of this study also cannot be directly compared with ours as they have also assessed endothelial function using flow mediated dilatation of a larger vessel, the brachial artery.
Microvascular endothelial function may be affected by factors such as age, sex and the co-existence of systemic diseases. In this study, a multivariate analysis was conducted to identify the possible confounding factors that may affect microvascular endothelial function. Ageing is known to cause reduction in the endothelial cells and reduction of their function. 40 Ageing also causes arteriolosclerosis that may affect the ability of the vessel to dilate. 41 It was demonstrated that arginase I may compete for L-arginine with eNOS as age increases. This results in reduced production of NO and endothelial dysfunction. 42 In this study, the mean age of POAG patients was 64.0 (8.5) years and mean age of controls was 62.7(9.7) years. As expected, based on multiple linear analysis, there was negative linear relationship between age and microvascular endothelial function in this study.
Similar negative linear relationship of DBP and microvascular endothelial function was also observed in our study. Ageing process increases atherosclerosis changes and the incidence of systemic hypertension. 43 Systemic hypertension and POAG are believed to be associated with oxidative stress. 44 Oxidative stress leads to reduce endothelial function. 45 Oxidative stress in hypertensive patients leads to diminished NO and correlates with the degree of impairment of endothelium-dependent vasodilation. 46
There is compelling evidence that impaired NO signalling plays an important role in the endothelial cell dysfunction associated with POAG. They found associations between functional eNOS gene variants and POAG cases versus controls.47–50 The vascular endothelium produces NO, a potent vasodilator, under basal conditions and also in response to physiological provocation.51–53 NO is formed from L-arginine by the enzyme nitric oxide synthase (NOS).54,55 There are three types of NOS, namely, endothelial NOS (eNOS), inducible NOS (iNOS) and neuronal NOS (nNOS). eNOS is the most widely available form in the vascular endothelium and is responsible for regulation of blood flow in a tissue.56,57 CAV1 and CAV2 are members of the caveolin gene family that are expressed in most human cell types [including the trabecular meshwork (TM) in normal and glaucomatous tissue]. 58 The proteins formed by these genes interact with eNOS to reduce the production of nitric oxide. CAV1 is upregulated in the TM 1 h after an increase in IOP. 59 A large genome-wide association study in Iceland identified an association with POAG and a SNP on chromosome 7q31. 59 This SNP is within a linkage disequilibrium block that contains CAV1 and CAV2.
In this study, we measure microvascular endothelial function peripherally using LDF and process of iontophoresis, based on the concept of underlying generalized vascular endothelial dysfunction which affects peripheral vessels at the ONH and the endothelial cells that lined the trabecular meshwork. 60 Impairment of a vasodilatory response to ACh suggests endothelial dysfunction.61,62 Microvascular endothelial dysfunction is believed to affect the perfusion to the ONH and resistance to the aqueous outflow.63–65 Thus, microvascular endothelial dysfunction, through both the mechanical (reduction of aqueous outflow) and vascular mechanisms (impairment of perfusion to ONH), may play a role in increasing the susceptibility to glaucoma.
However, endothelial function in the peripheral vessels and end arteries in the eye may differ. The retinal arteries lose their internal elastic lamina as they bifurcate at optic disc. That differentiates them from arteries of other tissues, and as a compensatory mechanism, they have thicker muscularis. Thicker muscularis of retinal arteries leads to more vasodilation in response to chemical stimuli. The endothelial cells of retinal arteries are not fenestrated and linked by tight junctions, but in peripheral vessels, there are no tight junctions. 64 There may be other factors that affect the blood perfusion to ONH contributing to glaucomatous optic neuropathy. The technique adopted in this study allowed indirect evaluation of microvascular endothelial function and vascular dilatation.
Another limitation of this study is inability to fully confirm endothelial dysfunction as the sole cause of microvascular abnormality in our POAG patients. Abnormalities in vascular structure and vascular smooth muscle response may also contribute to the pathogenesis of POAG especially as the disease progresses and patients get older. Perhaps conducting a future study on newly diagnosed POAG patients may help to provide more information on the different roles of endothelial-independent and endothelium-dependent responses in the pathogenesis of POAG in Malay patients.
Conclusion
In conclusion, POAG patients have reduced microvascular endothelial function compared with control, non-POAG patients. This suggests a potential role of microvascular endothelial functions in the aetiology of POAG in Malay patients. Impairment in peripheral endothelial-dependent vasodilatation may lead to inadequate perfusion and cause glaucomatous damage.
Footnotes
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in parts by Universiti Sains Malaysia Research University Individual grant no. 1001\PPSP\812101, Universiti Sains Malaysia, Health campus, Kelantan, Malaysia.